Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
[CANCER RESEARCH55. 5276-5282, November 15, 19951
Chemosensitivity Testing of Human Tumors Using a Microplate Adenosine
Triphosphate Luminescence Assay: Clinical Correlation for Cisplatin
Resistance of Ovarian Carcinoma'
Peter
K Andreotti,2
Ira Gleiberman,
Ian A. Cree,
Christian
M. Kurbacher,
Diana
M. Hartmann,
Dee Linder,
Guy Harel,
Phillip A. Caruso, Sharon H. Ricks, Michael Untch, Christian Sartori, and Howard W Bruckner
BATLE LE Laboratories [P. E. A., D. M. H., D. L, G. H.) and Northridge Medical Center (L G., P. A. C., S. H. RI, Fort Lauderdale. Florida 33334; Department of Pathology.
institute of Ophthalmology, University of London, London ECI V9EL, England (I. A. CI; Department of Obstetrics and Gynecology, University of Bonn, D-53105 Bonn, Germany
(C. M. K.): Klinikum Grosshadern, Frauenklinik, Universitat Munchen, 81377 Munich, Germany [M. UI; DCS innovative Diagnostik Systeme, D-22397, 65 Hamburg, Germany
(C. S.); and Derald H. Ruttenberg Cancer Center, Mount Sinai School ofMedicine, New York, New York 10029 fH. W. B.)
ABSTRACT
randomized
studies
demonstrating
efficacy
and benefit
have limited
their application to patient care.
An ATP luminescence assay (TCA 100) was used to measure chemo
ATP luminescence is a sensitive and precise method for measuring
therapeutic
drug sensitivity and resistance of dissociated tumor cells
cell viability (10—22).Since 1984, a number of groups have used ATP
cultured for 6 days in serum-free medium and 96-well polypropylene
luminescence to test the chemosensitivity of both cell lines and tumors
microplates. Studies were performed with surgical, needle biopsy, pleural,
or asciticfluid specimensusing 10,000—20,000
cells/well.ATP measure (7, 13—20).The TCA-100 method described in this report uses AlT
luminescence to measure chemotherapeutic drug sensitivity and re
ments were used to determine
tumor growth inhibition.
Single agent and
sistance
of dissociated tumor cells cultured for 6 days in serum-free
drug combinations
were evaluated
using the area under the curve and
medium and polypropylene microplates to inhibit the survival of
50% inhibitory
concentration
(ICse) Ft@SUItS for a series of test drug
non-neoplastic cells (21—27).This method was developed from a
concentrations. The ATP luminometry method had higj sensitivity, line
arity, and precision for measuring the activity of single agents and drug
previously published technique using medium containing serum and
combinations.Assayreproducibilitywas high with intraassayand inter agarose-coated microplates (28). Both solid tumors and hematological
assay coefficients of variation of 10—15%for percentage of tumor growth
malignancies have been tested with the TCA-100 (23, 24). High
inhibition,
5—10% for area under curve, and 15—20% for ICse F@5U1t5.
sensitivity allows replicate testing of six single agents or drug com
Good correlation (r = 0.93) between the area under the curve, and ICse
binations at seven concentrations with less than two million cells. The
results was observed. Cytological studies with 124 specimens demon
system provides dose-response results and is able to detect heteroge
strated selective growth of malignant cells in the serum-free culture
neity of drug sensitivity between tumors (22) and drug combination
system. Studies with malignant and benign specimens also showed selec
effects consistent with clinical experience (26).
tive growth of malignant cells in the serum-free medium used for assay.
This report describes technical parameters and principal consider
The assay had a success rate of 87% based on criteria for specimen
ations for testing single agents and drug combinations against human
histopathology, magnitude ofcell growth, and dose-response drug activity.
Cisplatinresultsfor ovariancarcinomaare presentedfor 81 specimens tumors using the TCA-100. Results are presented for 81 specimens
from 70 untreated
patients and 33 specimens
from 30 refractory
patients.
from 70 untreated patients and 33 specimens from 30 refractory
A model for interpretation of these results based on the correlation of patients which that indicate the assay has >90% accuracy for cisplatin
clinical response with the area under the curve and ICse results indicates
resistance of ovarian carcinoma.
that the assay has >90% accuracy for cisplatin resistance of ovarian
carcinoma. Additional studies are in progress to evaluate the clinical
efficacy of this assay.
MATERIALS AND METHODS
Specimen
Preparation.
INTRODUCTION
biopsy
The feasibility of patient-specific chemotherapy based on in vitro
testing has been shown using a variety of different TCA3 methods
(1—3).Correlations of TCA results with clinical outcome have mdi
cated predictive accuracies of 57—83%for drug sensitivity and >90%
for drug resistance (1, 2, 4—7).These success rates are comparable to
estrogen receptor assays for breast cancer (8, 9). Although studies
have demonstrated predictive accuracy for different TCA methods,
technical limitations for some methods and the lack of prospective
ascitic fluid specimens
specimens
penicillin,
The costs of publication of this article were defrayed in part by the payment of page
charges. This article must therefore be hereby marked advertisement in accordance with
18 U.S.C. Section 1734 solely to indicate this fact.
I This
work
was
supported
in
part
by
BAThE
LE
(Ft.
Lauderdale,
FL)
and
DCS
Innovative Diagnostik Systeme (Hamburg, Germany).
2 To
whom
requests
for
reprints
should
be
addressed,
at
ASD,
Inc.,
3940
NW.
75th
Terrace, Ft. Lauderdale, FL 33319.
3 The
abbreviations
used
are:
TCA,
tumor
chemosensitivity
assay;
CAM,
complete
assay medium; TDC, test drug concentration; 4-HC, 4-hydroperoxy-cyclophosphamide;
DDP, cisplatin; DOX, doxorubicin; TAX, Taxol; VP-16, etoposide; 5-RI, fluorouracil;
MMC, mitomycin C; MO, no inhibition control; MI, maximum inhibition control; PAP,
Papanicolaou; TGI, tumor growth inhibition; AUC, area under curve; IC,0, 50% inhibitory
concentration; CP, 4-HC + cisplatin; CAP, 4-HC + doxorubicin + cisplatin; FBS, fetal
bovine serum; CV, coefficient of variation; AP, DOX + DDP.
were
performed
with
in DMEM
(GIBCO)
containing
@.tWmlstreptomycin,
and 100
were collected
surgical
@tg,/mlkanamycin.
and transported
or needle
300 units!ml
Pleural
in vacuum
and
bottles
(McGaw S9901) with 25—50units!ml sodium heparin (Upjohn). Peripheral
blood and bone marrow specimens were collected in vacutainer tubes with
sodium heparin or EDTA. Specimens were obtained according to protocols
approved by the hospital Institutional Review Board after patient informed
consent was obtained. Specimens were tested only after selection of appropri
ate tissue for histological and other clinical diagnostic evaluation.
Solid tumors were minced into 0.5—2.0-mm3
fragments under sterile con
ditions after excising excess fat and normal tissue. Fragments were then
dissociated
Received 5/18/94; accepted 9/19/95.
300
Studies
transported
into a cell suspension
of single
cells
and small
aggregates
by
incubation in 5—10
ml sterile Tumor Dissociation Enzyme Reagent for 4—18h
at 37°C. Bone marrow,
peripheral
blood,
and pleural
and ascitic
fluid speci
mens were prepared by Ficoll-Hypaque density gradient centrifugation (His
topaque; Sigma). Ficoll-Hypaque was also used to reduce erythrocyte contam
ination and increase cell viability for some solid tumor specimens. Cells were
washed twice and resuspended for assay in LMA4 CAM at 1.0—2.0X 10@'
cells!ml. CAM containing 10% serum was used in some studies as indicated in
the text.
TCA-100 Reagents and Chemotherapeutic Drugs. TCA-100 reagents
were obtained from BAThE LE (Fort Lauderdale,
FL) or DCS Innovative
Diagnostik Systeme (Hamburg, Germany). Therapeutic grade drugs from
commercial sources were stored, prepared, and used before expiration dates
5276
Downloaded from cancerres.aacrjournals.org on August 11, 2017. © 1995 American Association for Cancer
Research.
AlP CHEMOSENSITWITY TESTING
according
to the manufacturer.
Single
agents
and drug
combinations
z
0
E
were
tested at six dilutions corresponding to 200%, 100%, 50%, 25%, 12.5%, and
6.25% of a standard TDC. TDC values were determined by pharmacokinetic
I
z
and clinical information (29—33)and empirical clinical evaluation of assay
results. Standard TDC values were 3.0
@Wmlfor 4-HC, 3.8
@Wmlfor DDP,
0.5 @g/ml
for DOX, 6.8 @Wml
for TAX, 48.0 @Wml
for VP-16, 22.5 @Wml
for
5-FU, and 0.23 @Wml
for MMC. Drug combinations were tested by combining
single agents. Fresh drug solutions were used, except 4-HC (Scios Nova, Inc.)
was divided into 5-mg/mI aliquots and stored at —20°C
until use.
Chemosensitivity Assays. Cultures of 10,000—20,000cells!well were
tested in 96-well round-bottomed polypropylene microplates (Costar 3790).
Each microplate was used to test four to six single agents or drug combinations
at six concentrations in triplicate or duplicate as described previously (21, 22,
26, 27). Microplates contained 6—12MO control wells and 6—12MI control
wells. Controls were set up by adding 0.1 ml cell suspension to 0.1 ml CAM
I
in MO wells and 0.1 ml maximum AlT inhibitor in MI wells. Test drug
dilutions were set up in culture microplates
PERCENTTEST DRUGCONCENTRATION
by doubling dilutions of fresh
800% TDC solutions in 0.1 ml CAM/well before adding 0.1 ml cells!well.
ATP Extraction and Luminometry. Afterincubationof the culturesfor 6
to 7 days at 37°Cin a >98% humidified, 95% air-5% CO2atmosphere, cellular
AlP was extracted and stabilized by mixing 0.05 ml tumor cell extraction
reagent into each well. AlP was measured in a Berthold LB-96P or LB-953
luminometer using 0.05 ml culture extract injected with 0.05 ml luciferin
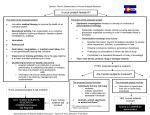
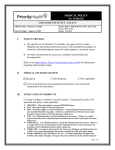
Fig. 1. Single agent and drug combination sensitivity and resistance. Results for 4-HC,
DDP, and CP (4-HC + CE) for a primary untreated ovarian carcinoma patient (H. B.; A,
., @),
whoshowed
acomplete
clinical
response
tofirst-line
CPtherapy,
andarecurrent,
previously treated ovarian carcinoma patient (A. C.; @,
0, 0), who showed progressive
disease during CP therapy. Results for patient H. B. show assay characteristics for drug
sensitivity. Results for patient A. C. show assay characteristics
for drug resistance.
luciferase counting reagent. A 10-s count integration time with a 4-s delay was
used. For experiments in Fig. 2, cells suspended in CAM at 4.0 X 10@viable
cells/ml
were
serially
diluted
in microplate
wells
containing
0.1 ml CAM.
CAM (0.1 mE/well)was then added to give cell dilutions in 0.2 ml. The cells
and controls of 0.2 ml CAM/well without cells were immediately extracted and
counted. An Al? standard curve was performed for all studies using 0.05-ml
aliquots of a 250 ng,/mlAlT standard serially diluted 1:3 in dilution buffer.
Microplates
were stored
Cytology
and
at —20°Cfor repeat
Immunocytochemistry.
measurements
Cytological
if required.
examination
before
and after TCA-100 culture was performed in multiple laboratories with 124
specimens including 39 breast tumors, 78 ovarian tumor or ascites specimens,
and 7 other solid tumors. Cytospin preparations of dissociated tumor cells,
A. C. show characteristicsfor drugresistancewith low AUC values of
PAP. Slides were reviewed by direct microscopy, and the percentage of
1194, 4382, and 5115 for 4-HC, DDP, and CP, respectively, and
<40% TGI for the single agents and CP combination. AC does not
show sigmoidal dose-response curves or a significant CP drug com
bination effect.
Results for patient H. B. are illustrative for using AUC, IC50, and
percentage of TO! for interpretation. The 11.8% AUC increase for CP
compared to 4-HC indicates only a modest combination effect and
increase in sensitivity for CP. The corresponding IC50 decrease from
32.1% to 10.9% TDC indicates a significant combination effect and a
three-fold increase in sensitivity for CP. This interpretation based on
malignant cells before and after culture for 6 to 7 days was visually estimated.
IC50 @5
more consistent with stronger CP sensitivity evident by 100%
ascites,
or day 6—7 MO control
wells were stained
with periodic
acid-Schiff
(n = 49) or PAP (n = 64). Giemsa and hematoxylin and eosin were used on
occasion. Immunostaining was performed for 30 cases by the avidin-biotin
complex method (Biomen; Finchampstead) using monoclonal antibodies
(DAKO Ltd.) against vimentin, cytokeratins (CAM5.2, EP4), or p53 (D07)
kindly
provided
by Professor
B. Lane (Department
of Anatomy,
University
of
Dundee, Scotland). Cytological studies with malignant and benign specimens
tested in CAM and medium containing serum (Table 3) were performed using
@
later at the time of assay. Results for patient H. B. show characteristics
for drug sensitivity. These include high AUC values of 15,609,
13,384, and 17,444 for 4-HC, DDP, and CP, respectively, and 100%
TGI for 4-HC and CP. Patient H. B. also showed sigmoidal dose
response curves for 4-HC and CP and a significant CP drug combi
nation effect evident by decreasing IC50 values of 32.1%, 28.6%, and
10.9% TDC for 4-HC, DDP, and CP, respectively. Results for patient
Analysls of Results. Percentageof TGI for each test drug concentration TO! at the 200—100%TDC. In contrast, the 16.6% AUC increase for
was calculated:
4-HC compared to DDP provides a better measure than IC50 for the
stronger 4-HC sensitivity, since both drugs have essentially identical
TDC - MI
1.0 —MO —MI
=
TGI
IC50values and 4-HC shows 100% TO! compared to only 85.2% for
DDP.
where MO = mean counts for no inhibition control cultures, MI = mean counts
for maximum inhibition control cultures, and TDC = mean counts for replicate
test drug cultures.
AUC values were calculated using the trapezoidal rule. IC50values were
calculated by interpolation.
Percentage of coefficient of variation was calcu
lated by SD!mean. The Wilcoxon rank sum nonparametric statistics were used
to determine the significance of differences in AUC values with different cell
concentrations.
Student's t test was used to compare AUC and IC50 values for
DDP refractory and untreated patients.
RESULTS
Drug Sensitivity and Resistance Parameters. Fig. 1 shows 4-HC,
DDP, and CP (4 HC + DDP) results for a primary, untreated ovarian
carcinoma patient (H. B.) who had an objective complete response to
cP therapy, and a recurrent ovarian carcinoma patient (A. C.) who
received first-line CP therapy (6 times) and then showed continued
progressive disease during further C? therapy (twice) 11—12months
AlP Sensitivity and Assay Reproducibility.
Analysis of Al?
standard curves has shown that the luminometry method has a lower
limit of sensitivity of 1.9 pg AlT, linearity (r > 0.98) up to 12.5 ng of
Al?, and mean intraassay and interassay coefficients of variation of
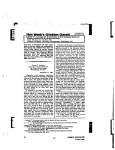
4.88 and 7.28% (data not shown). Fig. 2 shows sensitivity, linearity,
and reproducibility for the measurement of cellular Al? with the
extraction and luminometry method. Linearity (r > 0.98) for 39—
20,000 cells/well was observed for ovarian adenocarcinoma, lym
phoma, and bone marrow cells. A peripheral blood acutemyelogenous
leukemia specimen (77% blasts) showed sensitivity to 78 cells/well.
The mean intraassay coefficient of variation for triplicate Al? meas
urements was 6.92%.
Table 1 shows representative sensitivity and reproducibility results
for measuring single agents and drug combinations. These data were
obtained by testing an ovarian adenocarcinoma pleural effusion spec
imen twice on the same day by three investigators. Standard assays
with 20,000 cells/well were performed for triplicate measurements of
5277
Downloaded from cancerres.aacrjournals.org on August 11, 2017. © 1995 American Association for Cancer
Research.
AlP
Primary Ovarian
Lymphoma
Blood AML
@
a.
Adenocarcinoma
Specimen Evaluability and CUltUre. Three criteria have been
Bone Marrow
100
TESTING
in triplicate against seven specimens. The mean coefficient of varia
tion for MO controls was 6.34%.
io6
1,000
@
@
@
@
@
CI{EMOSENSITIVITY
used to determine the evaluability of a specimen and assay results: (a)
the specimen must have confirmed malignant cytology and/or histol
ogy; (b) viable MO control cells must be evident after 6—7days of
culture and have mean MO values >50,000; and (c) dose-response
curves for drug activity must be observed.
io5
1O@
10
:D
.
-J
@
i
1@O
160
1,000
10,000
NUMBER OF CELLS
Fig. 2. Cellular ATE measurement. Sensitivity (39—78cells/well), linearity (r > 0.98),
and reproducibility (CV. = 6.92%) for measuring ATP from clinical specimens with the
TCA-IOO extraction and luminometry method.
4-HC, DOX, DDP, and CAP (4-HC + DOX -i-DDP). Reproducibility
for TOl and AUC was highest at high levels of drug activity. Mean
intraassay and interassay coefficients of variation for percentage of
TO! were 9.96 and 10.93%. The mean coefficient of variation was
4.96% for TGI > 30%. High reproducibility was also observed for
AUC values with intraassay and interassay coefficients of variation
7.63%. Variability for TO! < 30% had little effect on AUC values.
The mean interassay coefficient of variation for IC50 was 14.85% with
intraassay CVs > 20% for DOX and CAP, which had low IC50 values.
Additional data also indicate greater reproducibility as drug activity
increases. Mean coefficients of variation were 1.76, 6.85, 14.5, and
24.79% for 100 to 70%, 70 to 50%, 50 to 30%, and 30 to 0% TO!
(n = 90, 56, 58, 132) for 56 single agents or drug combinations tested
MO
control
results
are
shown
in Table
2 for
97 (87%)
Table 1 intraassay and inlerassay reproducibilizy of
TCA-100Drug%
concentrationAUCIC5020010050.0
Test
drug
25.012.56.254-HC99.694.152.0
27.518.318.71473048.04-HC99.796.756.9
24.125.114.51510144.74-HC98.791.051.7
28.522.224.61451348.24-HC99.790.749.2
31.723.320.21451051.04-HC99.792.549.9
25.114.19.41442750.14-HC99.894.657.9
33.626.411.21516841.9Mean99.593.352.9
28.421.616.41474147.3SD0.42.13.3
3.34.25.32933.1CV
11.996.60DOX98.389.661.4
(%)0.392.266.26
11.7819.4332.1
55.543.537.41550419.3DOX98.388.570.7
54.550.939.61582412.0DOX98.195.176.5
59.349.238.01659113.5DOX98.694.167.3
62.150.039.41626412.5DOX98.392.467.3
54.737.735.31586021.5DOX98.996.274.4
59.047.938.91662414.9Mean98.492.669.6
57.546.538.11611115.6SD0.32.85.0
2.84.61.54153.6CV
4.879.853.832.5722.85DDP62.637.623.3
(%)0.273.027.18
15.86.02.97186149.6DDP63.744.728.1
22.415.912.48199127.9DDP66.744.235.9
28.720.823.78800125.8DDP70.646.636.1
25.124.414.69125114.2DDP61.042.330.3
22.212.710.87924141.2DDP70.243.431.1
26.415.56.58595124.6Mean65.843.130.8
23.415.911.88305130.5SD3.72.84.4
4.15.86.663411.6CV
17.4836.7655.497.638.90CAP99.797.493.0
(%)5.596.4814.43
68.552.943.21768910.6CAP99.797.792.9
58.553.340.51751710.9CAP99.697.694.1
68.255.449.2177807.1CAP99.897.393.7
68.357.145.6177578.6CAP99.697.090.5
68.247.533.41747614.0CAP99.997.694.6
71.654.543.8178499.9Mean99.797.493.1
67.253.442.61767810.2SD0.10.21.3
4.13.04.91372.1CV
(%)0.090.231.41
of
1 12 fluid
or solid tumor specimens with malignant cytology which were evalu
able in one laboratory. Mean and median MO controls for the 97
specimens were 268,976 and 174,534. MO controls ranged from the
lower acceptable limit of 5.0 X iO@to 1.6 X 108 for rapidly growing
ascites or pleural fluid specimens with high percentages (>90%) of
malignant cells. MO:MI ratios > 100:1 were routinely obtained with
mean and median MI controls of 745 and 411. Fifteen (13%) of 112
specimens with malignant cytology were nonevaluable. These in
cluded 10 that failed to survive in the culture system and 5 that did not
show acceptable dose-response curve results. For 21 specimens with
indefinite or no convincing evidence of malignancy, 16 failed to
survive in the culture system and 5 benign proliferative or premalig
nant specimens showed survival. These included a pseudolymphoma,
histiocytoma, fibroadenoma, and two lymph node biopsies. Seven
pleural or ascitic fluid specimens with high percentages (>80%) of
histiocytes or mesothelial cells were nonevaluable based on >50%
survival of benign cells after 6 days of culture.
For some specimens, such as needle biopsies, 10,000—20,000 cells/
well were tested instead of the standard 20,000 cells/well. The effect
of cell concentration on sensitivity was therefore evaluated with 41
paired combinations of single agents or drug combinations tested
6.075.6211.430.7721.06
5278
Downloaded from cancerres.aacrjournals.org on August 11, 2017. © 1995 American Association for Cancer
Research.
AlP
CHEM0SENS@VITY
Table 2 MO control values for evaluable tumor specimen?
Tumor type tested
n
Mean/median (X 10@)
Range (X 10@)
Unknown primary
Breast
10
11
276.5/193.3
231.5/176.9
129.1—544.0
87.0—605.6
Colorectal
Gastric
Head and neck
Liver/bile duct
10
4
2
2
136.9/121.3
175.8
137.3
146.7
50.8—338.1
126.8—275.2
98.4—176.2
132.3-161.0
Lung
4
184.7
Melanoma
Mesothelioma
2
2
170.9
84.3
Ovarian
39
Pancreatic
Renal cell
Sarcomas
5
3
3
a Tumor
cells were
tested
62.8—268.5
108.2—233.8
78.7—89.9
327.5/302.1
58.6—1,244.7
170.3
368.5
720.1
at 10,000—20,000
78.7—354.4
61.9—852.0
142.1—1,653.0
cells/well
in CAM
for 6 to 7 days.
MO
results are expressed as luminometer counts/lO s.
against four ovarian specimens at 10,000 and 20,000 cells/well.
Higher AUC values (>15%) were obtained with 10,000 cells/well for
32 of 41 paired combinations. This difference was statistically signif
icant, but the mean increase in AUC values was only 7.75% and did
not affect the interpretation of results.
Culture Media and Malignant Cell Growth. Results for seven
studies shown in Table 3 illustrate the advantage for using CAM
without, FBS. For study TC, a benign liver nodule was tested in CAM
and CAM containing 10% human serum or FBS from two sources.
Cytology before culture showed 70—80% inflammatory cells with
nonmalignant atypical cells. MO values in CAM and CAM-10%
human serum were below the lower acceptable limit of 5.0 X i04, and
therefore the assays were nonevaluable. In contrast, MO values were
1.2—1.7x iO@ for the cultures with FBS. Cytology after culture
showed few leukocytes in the CAM and predominantly histiocytes
with 30—40%atypical cells in cultures with FBS. Similar results were
obtained for studies BM and SW using benign lymph node and skin
biopsy specimens. Assays were nonevaluable in CAM with MO
values below 5.0 x iø@,whereas MO values were 2.0—3.7X 10@for
assays in CAM or RPM! 1640 with FBS. Cytology after culture
showed the survival of histiocytes and leukocytes in the node speci
men cultured in CAM + FBS and epithelial cells with leukocytes in
TESTING
the skin biopsy cultured in RPM! 1640 + FBS. These results were
similar to six studies with normal peripheral blood mononuclear cells
showing MO values of 0.9—3.5X 10@in CAM or RPM! 1640 with
FBS and < 3.0 x 10―in CAM without FBS (34).
Effects of FBS on cell survival and drug sensitivity for malignant
specimens are illustrated by studies OM, MV, RF, and MM in Table
3. Surgical biopsy specimens for recurrent ovarian adenocarcinoma
and unknown primary adenocarcinoma were tested in CAM,
CAM + FBS, and RPM! 1640 + FBS. Cell preparations that were
tested contained 40—85% malignant glandular cells or poorly differ
entiated adenocarcinoma cells with 15—60%leukocytes, histiocytes,
and/or mesothelioma cells. Higher MO values (1.6—7.3-fold) were
obtained with media containing FBS. These results were consistent
with an observed increase in the total number of cells in the cultures
with FBS, and 33 similar studies showing a mean 1.8-fold increase in
MO values for assays using media with FBS. Cytology before and
after culture showed >85% malignant cells after culture in CAM
compared to <75% malignant cells after culture in media with FBS.
Differences in 4-HC, DDP, DOX, VP-16, and 5-FU sensitivity also
were observed for studies OM, MV, and RF. Significant differences in
drug sensitivity were not observed for study MM, which showed
>85% malignant cells before and after culture in CAM or
CAM + FBS.
The selective growth of malignant cells in CAM was evaluated
using cytology before and after culture with 124 specimens. The mean
proportion of malignant cells before culture was 54% (10—
95% ±22%). After culture, the mean proportion of malignant cells
was 83% (30—100%±14%). The mean increase in the percentage of
malignant cells before and after culture was 29% (—10—80%
±20%),
showing that there was a significant selection of malignant cells in all
but 3 of 124 specimens. Thirty-two (64%) of 50 specimens with
20—50%malignant cells before culture showed >80% malignant cells
after culture, and 58 (92%) of 63 specimens with >50% malignant
cells before culture showed >80% malignant cells after culture. Im
munostained preparations (n = 30) showed a mean of 56% (15—
90% ± 22%) malignant cells before culture and 92% (—10—
80% ±22%) after culture. The mean increase in malignant cells was
Table3 Differences in MO controls andAUC values
mcdiii'Mean
for specimenstested
indifferent
culture
MOStudy/specimenCulture
medium(X10@)4-HCDDPDOXVP-165-FUTC/benign
0.9n.e.@'liver
inflammatory noduleCAM103
pancreaticcarcinomaCAM
biopsy, suspected
13,944BM/benign
3.2n.e.n.e.n.e.n.e.n.e.cell
axiliary node, non-smallCAM48.7
lung adenocarcinomaCAM
7.116,2148,5798,46612,068nd.―SW/benign
skin biopsy, suspectedCAM12.1
0.7n.e.n.e.n.e.n.e.n.e.angiosarcomaGM/serosal
±
+ 10% PHSC
CAM + 10% FBS F-2442
CAM ÷10% FBS 16-501C41.8
+ 10% FBS201.3
13,2539,513
8,46415,804
14,90915,563
14,98813,422
±
±
1640 + 10% FBS
biopsy, recurrentRPMI2,766ovarian
±1.9
167.4 ±22.4
123.7 ±8.414,641
±
±45.1
128.2 ±10.117,636
CAM370.6
8,79212,164
5,61117,612 15,376nd.
9,5731,267
adenocarcinomaMV/serosal
+ 10% FBS
biopsy, recurrentCAM
nd.―ovarian
±92.4
CAM929.4
734.9 ±68.35,947
10,13513,648 4,13214,833 7,99214,196
6,96613,843
adenocarcinomaRF/chest
+ 20% FBS
wall biopsy, unknownCAM
nd.2,597primary
CAM1,154.1
±123.9
326.9 ±2.26,052
1640 + 10% FBS
CAM1,769.3
125.5 ±2.110,963
12,90111,423
13,32813,144
14,31013,7212,894
CAM
255.8±12.2
11,122
12,351
14,968
6,1787,714
4,58811,889 10,74111,884
adenocarcinomaMM/lymph
node biopsy, unknownRPMI
4,660primary
±132.6
adenocarcinoma
a Tumor
b n.e.,
cells were
nonevaluable;
C Pooled
human
d nd.,
not done.
male
tested
MO
AB
at 18,000—20,000
controls
were
below
+ 10% FBS
cells/well
the lower
in CAM
13,868
for 6 to 7 days.
acceptable
limit
of 5 X
i0@.
serum.
5279
Downloaded from cancerres.aacrjournals.org on August 11, 2017. © 1995 American Association for Cancer
Research.
5,552
@
@4
ATP CHEMOSENS1TIVITYTESTING
VP-16, TAX, 4-HC, and DOX. VP-16 was the strongest single
agent with activity greater than AP, CP, and TAX + DDP. Con
sistent with the low sensitivity and clinical resistance for DDP, the
DDP-based combinations AP, CP, and TAX + DDP did not show
activity that was markedly greater than DOX, 4-HC, or TAX alone.
CAP (4-HC + DOX + DDP) showed a combination drug effect and
stronger activity, consistent with the strong single agent activity of
both DOX and 4-HC. TAX + DOX showed the strongest drug
combination effect and activity.
Compared to similar studies with ovarian, breast, lung, and un
A
known
primary
tumors,
the AUC values
for 5-FU,
DDP,
and MMC
were below the 40th percentile (n = 22—44).AUC values were in the
55—70percentage for DOX (n = 48), 69—84percentage for 4-HC
(n
41), 76—91percentage for TAX (n = 43), 83—98percentile for
TAX + DOX (n = 39), and 85—100percentile for VP-16 (n = 34).
These findings identify 5-FU, DDP, and MMC as ineffective, and
DOX, 4-HC, TAX, and VP-16 as potentially more effective options
for second-line therapy.
Heterogeneity of Sensitivity and Interpretation of Results. Fig.
B
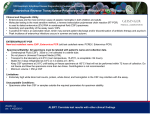
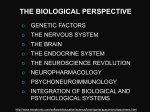
Fig. 3. Breast carcinoma cytologic morphology before and after culture in cytospm
preparations stained by monoclonal antibody CAMS.2 for cytokeratins. A, before culture
showing good cell dissociation with one positive cell surrounded by many negative cells;
B, after culture showing a clump of positively stained cells.
36% (—10—80%
±22%) in these samples. Fig. 3 shows the morphol
ogy of cells before and after culture of a breast carcinoma specimen
stained
for cytokeratins.
Application for Single Agents and Drug Combinations. Table 4
illustrates application for single agents and drug combinations for
a patient with unknown primary adenocarcinoma (60—70% poorly
differentiated adenocarcinoma cells) who developed resistance to
initial therapy with 5-FU + DDP. The clinically resistant drugs
5-FU and DDP showed the lowest sensitivity with < 70% TO! at
the 200% TDC. MMC and MMC + 5-FU + DDP showed similar
weak activity. Stronger single agent activity was observed for
DDPDrug
4 shows AUC and IC50 results for DDP tested against ovarian
carcinoma specimens. These included 81 specimens from 70 un
treated patients and 33 specimens from 30 refractory patients who
had progressive disease during DDP-based therapy, or early recur
rence (<6 months) after completion of DDP-based therapy. The
results illustrate the heterogeneity of sensitivity observed for DDP.
Good correlation between AUC and IC50 values was observed with
r = 0.93 for the untreated patients and r = 0.89 for the refractory
patients. The data in Fig. 4 illustrate a model for interpretation of
assay results based on empirical correlation of AUC and !C50
values with clinical response. Based on clinical studies that have
indicated a high quality clinical response rate of approximately
33% for primary ovarian carcinoma patients given single agent
DDP therapy (31,32), results for the most sensitive 27 (33%) of 81
untreated specimens would define the expected cut-off for DDP
sensitivity and resistance. DDP refractory patients would have
AUC values <12,610—18,782 (14,401 ±1,728) and IC50 values
>0.2—1.8(1.1 ±0.6) @.tg/mlobserved for the 33% most sensitive
untreated specimens. A@shown in Fig. 4, 31 of (93.9% specificity)
33 of the refractory specimens showed the expected low AUC and
high IC50 values, and only 2 of (6.1% false-positive) 33 refractory
specimens showed high AUC or low IC50 values within the cut-off
range for sensitivity. AUC and IC50 values for the 33 refractory
specimens (7739 ±3768 and 4.7 ±2.1 @g/ml)were significantly
different (P < 0.001) than corresponding values for the 27 of 81
primary specimens used to define the cut-off for resistance and
sensitivity.
Table 4 TCA-IfZ@resultsfor recurrent unknown primary adenocarcinoma after therapywith
concentrationAUCICso20010050.0
Test
5-FU +
drug
tested%
25.012.56.25TAX
78.266.954.9183194.9CAP99.999.996.7
+ DOX99.999.995.1
41.122.514.41714029.1VP-1698.389.878.9
61.043.328.91624917.2TAX
58.156.648.9159637.1TAX99.989.166.8
+ DDP99.985.773.8
54.550.347.61582512.4CP99.999.863.0
24.813.212.51547041.5AP99.998.354.2
29.619.01731518745.74-HC99.997.452.6
20.419.710.91487447.9DOX99.983.044.2
21.718.911.61349857.5MMC
8.83.3—2.49286105.9MMC65.548.536.0
+ 5-FU + DDP93.947.223.0
20.017.47.18823108.8DDP56.136.617.5
2.37.67.16343168.75-FU68.930.88.6
0.30.1—5.16068150.4
5280
Downloaded from cancerres.aacrjournals.org on August 11, 2017. © 1995 American Association for Cancer
Research.
ATP CHEMOSENS@VITY TESTING
E
a'
0
ci
In
Cytological studies with solid tumor and pleural and ascitic fluid
specimens in different laboratories have shown that the assay selects
for malignant cell growth. Specimens with >20% malignant cells are
suitable for assay, although we believe it is important to perform
cytology on dissociated or pleural specimens to ensure this. Differ
entiation between epithelial and nonepithelial cells can be difficult,
but immunostaining with Ber-EP4, an antibody directed against a Mr
350,000 mucin-associated glycoprotein, allowed discrimination be
tween mesothelial and malignant cells in ascitic fluid (38). A higher
proportion of cells were thought to be malignant by immunostaining,
with >90% at the end of the assay probably due to the difficulty of
morphological recognition of all of the malignant cells present in
periodic acid-Schiff- or PAP-stained preparations.
AREAUNDERCURVE
The magnitude of cell viability is important for determining evalu
ability
and interpreting results. Studies have indicated that a low
Fig. 4. DDP AUC and IC50 heterogeneity and correlation for resistance. Heterogeneity
and correlation (r = 0.93) for DDP AUC and lC.,@)values for 81 specimens from 70
background level of normal cell survival may be detectable after 6
primary untreated ovarian carcinoma patients and 33 specimens from 30 refractory
days of culture due to the sensitivity of the method, and false-positive
patients who showed progressive disease during DDP- based therapy. Inset, AUC cut-off
results may be obtained in assays with low MO control values. A
of 12,610 and IC@()cut-off of I .8 @eg/mlfor the most sensitive 33% (27/81) untreated
specimens.
lower limit for cell viability defined by the MO control values or Al?
concentration has therefore been used as a criterion for evaluability.
DISCUSSION
The survival of some benign proliferative and premalignant speci
mens in the culture system indicates that the assay is not completely
The TCA-100 has a number of advantages for chemosensitivity
specific for malignant cells. Some ascitic and pleural fluid specimens
testing of clinical specimens. It requires only 6—7days, has a high
containing relatively small subpopulations of malignant cells (<20%)
evaluability rate (87%), and has high sensitivity to measure both
have shown survival of benign cells in the culture system. This may
proliferating and nonproliferating tumor cells. The assay has the
be due to autocrine support of benign cells. It is essential to evaluate
sensitivity, reproducibility, linearity, and precision to measure as few
the histopathology of the specimen or the cells tested to determine
as 39—78cells/well (Fig. 2), and cell line studies can be performed
evaluability. Dose-response drug activity has also been established as
using only 2000—5000cells/well (12, 26, 35). High sensitivity of the
an essential criterion for evaluability.
assay facilitates replicate testing of multiple drugs or combinations at
Differences between in vivo pharmacokinetics and in vitro drug
different concentrations, even with small specimens such as needle
exposure
conditions are a principal consideration. Continuous in vitro
biopsies or endoscopy samples (22).
drug
exposure
simplifies the testing of multiple drugs and combina
Assay reproducibility is ±10—15%
for percentage of TGI, <±10%
tions
and
allows
detection of clinically relevant drug combination
for AUC, and ±15—20%
for IC50 results. System reproducibility is a
effects
(Fig.
1
and
Table 4). Studies have indicated that a culture
function of the level of drug activity. Less than ±10%variability has
period of 5—6days is required to observe maximum drug activity and
been observed for 100—50%TO! results, while higher variability of
combination effects (26). Experience has shown that it is necessary to
±15—25%
has been observed for TO! results below 50%. Assay
empirically determine TDC values and algorithms for interpretation to
variability has a greater effect on IC50 values than AUC values (Table
correlate
results with clinical response. Reported peak plasma con
1). However, good correlation (r = 0.93) between AUC and IC50
values has been obtained (Fig. 4). Algorithms based on AUC, IC50, centration values (29, 30) have been found to give results for some
drugs that are not consistent with response rates determined by din
dose-response curve slope, and ability of a drug to achieve 100% TGI
ical studies (31—33).In studies with 42 untreated breast carcinomas
are being developed for predicting the response to individual drugs
using TDC values based on peak plasma concentration values and a
(21, 27).
one-level cut-off method to determine sensitivity and resistance, the
MO control results (Table 2) indicate that a subpopulation of the
test cell preparation is measured for drug sensitivity after 6 days in sensitivity frequencies for 4-HC (cyclophosphamide) and DOX cor
related with reported clinical response rates (33). However, the sen
culture. Mean MO controls of 84.3—720.1 X iO@ observed for dif
ferent tumors (Table 2) correspond to approximately 2000—5000 sitivity frequency for 5-FU was greater than that of both 4-HC and
DOX and reported response rates. These and other findings have
cells/well based on the results in Fig. 2. An evaluability rate of 87%
indicated the need to further develop specific algorithms for interpret
has been obtained using a standard concentration of 20,000 cells/well.
Increased drug sensitivity has been observed with specimens tested at ing results based on continuous drug exposure.
10,000—20,000 cells/well. However, the observed increase in sensi
The results in Fig. 4 show statistical significance for cisplatin
tivity at lower cell concentrations was comparable to interassay var
resistance for 31 of(93.9%) 33 ovarian carcinoma specimens based on
iation, and did not affect the ability to measure drug effects or the empirical correlation of AUC and IC50 values with untreated and
interpret results.
refractory specimens. These and other results from retrospective,
A defined serum-free assay medium improves the specificity of the
prospective, and double-blind studies have indicated predictive accu
culture system for malignant cells in a specimen (Table 3) and
racy for the test system in the range of 70—80% for drug sensitivity
provides better quality control. Other investigators have also used
and 90—93%for drug resistance.4 Multicenter studies with more than
serum-free culture media for chemosensitivity testing (20, 36, 37).
800 patients are in progress to correlate clinical parameters with TDC,
FBS increases the growth or survival of both malignant and normal
AUC, and IC50 values and algorithms for interpretation of results in
cells in the culture system and alters drug activity (Table 3). The CAM
order to perform prospective clinical studies.
culture system is designed to support the growth of tumor cells by
endogenous cell factors and to limit the survival of normal cells in
4 P.
E.
Andreotti,
C.
M.
Kurbacher,
I. A.
Cree,
M.
Untch,
and
H.
W.
Bruckner,
6-day cultures (34).
manuscript in preparation.
5281
Downloaded from cancerres.aacrjournals.org on August 11, 2017. © 1995 American Association for Cancer
Research.
AlP CHEMOSENSITIVITYTESTING
REFERENCES
21. Kurbacher, C. M., Mallman, P., Kurbacher, J. A., Sass, G., Andreotti, P. E., Rahmun,
A.,Hubner,H.,andKrebs,D.In vitroactivityof titanocenedichloride
versuscisplatin
I . Bellamy, W. T. Prediction of response to drug therapy of cancer. A review of in vitro
assays. Drugs, 44: 690—708,1992.
2. Fruehauf, J. P., and Bosanquet, A. G. In vitro determination
of drug response: a
discussion of clinical applications. In: V. T. DeVita, Jr., S. Hellman, and S. A.
Rosenberg (eds.), Cancer: Principles and Practices of Oncology, Ed., pp. 1—16
Philadelphia: J. B. Lippincott Co., 1993.
3. Black, M. M., and Speer, F. D. Further observations
on the effects of cancer
chemotherapeutic agents on the in vitro dehydrogenase assay activity of cancer tissue.
J. NatI. Cancer Inst., 14: 1147—1158,
1954.
4. Von Hoff, D. D., Kronmal, R., Salmon, S. E., Turner, J., Green, J. B., Bonorris, J. S.,
Moorhead, E. L, Hynes, H. E., Pugh, R. E., Belt, R. J., and Alberts, D. S. A
Southwest Oncology Group study on the use of a human tumor cloning assay for
predicting response in patients with ovarian cancer. Cancer (Phila.), 67: 20—27,1991.
5. Weisenthal, L. M., and Kern, D. H. Prediction of drug resistance in cancer chemo
therapy: the Kern and DiSC Assays. Oncology, 5: 93—103,1991.
6. Leone, L A., Meitner, P. A., Myers, T. J., Grace, w. R., Gajewski, W. H., Fingert,
H. J., and RotmanB. Predictivevalueof the fluorescentcytoprintassay(FCA):a
retrospective correlation study of in vitro chemosensitivity and individual responses
to chemotherapy. Cancer Invest., 9: 491—503,1991.
7. Sevin, B-U., Perras, J. P., Averette, H. E., Donato, D. M., and Penalver, M. Chemo
sensitivity testing in ovarian cancer. Cancer (Phila.), 71: 1613—1620,1993.
8. Wittliff, J. L. Steroid hormone receptors in breast cancer. Cancer (Phila.), 53:
630—643,
1984.
9. McGuire, w. L. Estrogen receptors in human breast cancer. J. Clin. Invest., 52:
14:1961—1966,
1994.
22. Hunter, E. M., Sutherland. L. A., Cree, I. A., Dewar, J. A., Preece, P. E., Wood,
R.A. B.,Linder,D.,andAndreotti,P. E. Heterogeneityin humanbreastcarcinoma:
use of an adenosine triphosphate (ATE) chemiluminescence assay. Eur. J. Surg.
Oncol., 19: 242—249,1993.
23. Andreotti, P. E., Linder, D., Hartmann, D. M., Becker, K., Herbst, K., Cree, I. A., and
Bruckner, H. W. AlP tumor chemosensitivity assay: application for solid tumors and
leukemia. In: A. A. Szalay, P. E. Stanley, and L. J. Kricka (eds.), Bioluminescence
and Chemiluminescence: Current Status, pp. 271—275Chichester: John Wiley &
Sons, 1993.
24. Andreotti, P. E., Bruckner, H. W., Cree, I. A., Becker, K., Cuttner, J., Caruso, P. A.,
and Gleiberman, I. Bioluminescence Sensitivity Testing. Proc. Am. Assoc. Cancer
Res., 34: 214, 1993.
25. Cree, I. A., Hunter, E. M., Sutherland, L. A., Subedi, A. M., Dewar, J. A., Preece,
P. E., andAndreotti,P. E. Breastcancerchemosensitivity
testingby ATElumines
cence assay. In: A. A. Szalay, P. E. Stanley, and L. J. Kricka (cdx), Bioluminescence
and Chemiluminescence: Current Status, pp. 276—280 Chichester: John Wiley &
Sons, 1993.
26. Andreotti, P. E., Linder, 0., Hartmann, D. M., Cree, I. A., Pazzagli, M., and Bruckner,
H. W. TCA-100tumorchemosensitivityassay:differencesin sensitivitybetween
cultured tumor cell lines and clinical studies. J. Biolumin. Chemilumin., 9: 373—378,
1994.
27. Kurbacher, C. M., Nagel, W., MaIlman, P., Kurbacher, J. A., Sass, G., Hubner, H.,
Andreotti, P. E., and Krebs, D. In vitro activity of titanocenedichlonde in human renal
73—77,
1973.
10. Ahmann, F., Garewal, H., Schifman, R., Celniker, A., and Rodney, S. Intracellular
adenosine triphosphate as a measure of human tumor cell viability and drug modu
lated growth. In Vitro Cell Dcv. Biol., 23: 474—480, 1987.
cell carcinoma compared to conventional antineoplastic agents. Anticancer Res., 14:
11. Maehara, Y., Anal, H., Tamada, R., and Sugimachi, K. The AlP assay is more
sensitive than the succinate dehydrogenase inhibition test for predicting cell viability.
Eur. J. Cancer Clin. Oncol., 23: 273—276,1987.
12. Petty, R. 0., Sutherland, L. A., Hunter, E. M., and Cree, I. A. Comparison of MiT
and ATE-based assays for the measurement of viable cell number. J Biolumin.
Chemilumin., 10: 29—34,1995.
13. Kangas, L., Gronroos, M., and Nieminen, A. L. Bioluminescence
and doxorubicin in primary and recurrent epithelial ovarian cancer. Anticancer Res.
of cellular ATE: a
new method for evaluating cytotoxic agents in vitro. Med. Biol., 62: 338—343,1984.
14. Garewal, H. S., Ahmann, F. R., Schifman, R. B., and Celniker, A. ATP assay: ability
to distinguish cytostatic from cytocidal anticancer drug effects. J. NatI. Cancer Inst.,
77: 1039—1045,1986.
15. Kuzmits, R., Rumpold, H., Muller, M., and Schopf, G. The use of bioluminescence
to evaluate the influence of chemotherapeutic drugs on Al? levels of malignant cells.
J. Clin.Chem.Clin.Biochem.,24: 293—298,
1986.
16. Sevin, B-U., Peng, Z., Perras, J., Penalver, G., and Averette, H. Application of an
AlP bioluminescence assay in human tumor chemosensitivity testing. Gynecol.
Oncol., 31: 191—204,1988.
17. Untch, M., Sevin, B-U., Perras, J., Angioli, R., Baibl, A., Nguyen, H. N., Hightower,
R.D.,andAverette,H. E.Chemosensitivity
of thenewanthracyclinepirarubicinand
other chemotherapeutic agents in primary and recurrent ovarian tumors in vitro.
Gynecol. Oncol., 47: 172—178,1992.
18. Gerhardt, R. T., Perras, J. P., Sevin, B-U., Petru, E., Ramos, R., Guerra, L., and
Averette, H. E. Characterization of in vitro chemosensitivity of perioperative human
ovarian malignancies by adenosine triphosphate chemosensitivity assay. Am. J.
Obstet. Gynecol., 165: 245—255,1991.
19. Maehani, Y., Anai, H., and Masuda, H. In vitro chemosensitivity testing evaluated by
intracellular Al? level: ATP assay. Jpn. J. Cancer Chemother., 13: 2342—2345,1986.
20. Terashima, M., Ikeda, K., Kawamura, H., Ishida, K., Saito, K., Yanagawa, 1., and
Tsukada, Y. A comparative study of the AlP assay in serum-free media and the
adhesive tumor cell culture system as a drug sensitivity test for human esophageal
cancer. Cancer Res. Ther. and Control, 3: 297—301,1993.
1529—1534, 1994.
28. Andreotti, P. E., Thornthwaite,
J. T., and Morse I. S. Al?
tumor chemosensitivity
assay. In: P. E. Stanley and L. J. Kricka (eds.), Bioluminescence and Chemilumines
cence: Current Status, pp. 417—420Chichester: John Wiley & Sons, 1991.
29. Dorr, R. T., and Fritz, W. L. Cancer Chemotherapy Handbook. New York: Elsevier,
1980.
30. Alberts, D. S., and Chen, H. S. B. Tabular summary of pharmacokinetic parameters
relevant to in vitro drug assay. In: S. Salmon (ed), Human Tumor Stem Cells, pp.
351—359.New York: Alan R. Lisa, 1980.
31. Thigpen, J. T. Chemotherapy of cancers of the female genital tract. In: M. C. Perry
(ed), The Chemotherapy Sourcebook, pp. 1039—1067. Baltimore: Williams &
Wilkins, 1992.
32. Cannistra, S. A. Cancer of the ovary. N. Engl. J. Med., 329: 1050—1059, 1993.
33. Kardinal, C. G. Chemotherapy of breast cancer. In: M. C. Perry (ed), The Chemo
therapy Sourcebook, pp. 948—988. Baltimore: Williams & Wilkins, 1992.
34. Andreotti, P. E., tinder, D., Hartmann, 0. M., Johnson, L. J., and Harel, G. A. AlP
lymphocyte activation assay: application for lymphokines and cytokines. In: A. A.
Szalay, P. E. Stanley, and L. J. Kircka (eds.), Bioluminescence and Chemilumines
cence: Current Status, pp. 257—261.Chichester: John Wiley & Sons, 1993.
35. Petty, R. D., Cree, I. A., Sutherland, L. A., Hunter, E. M., Lane, D., Preece, P. E., and
Andreotti, P. E. Expression of the p53 tumor suppressor gene product is a determinant
of chemosensitivity. Biophys. Biochem. Res. Commun., 199: 264—70,1994.
36. Schroy, P. C., Cohen, A., Winawer, S. J., and Friedman, E. A. New chemotherapeutic
drug sensitivity assay for colon carcinomas in monolayer culture. Cancer Res., 48:
3236—3244, 1988.
37. Zirvi, K. A., and Hill, G. J. Comparison of growth and drug response of human tumor
cells in serum-free and serum-supplemented media in human tumor clonogenic assay.
J. Surg.Oncol.,38: 88—93,
1988.
38. Diaz-Arias, A. A., Lay, T. S., Bickel, J. 1., and Chapman, R. K. Utility of BER-EP4
in the diagnosis of adenocarcinoma in effusions: an immunocytochemical study of
232 cases. Diagn. Cytopathol., 9: 516—521, 1993.
5282
Downloaded from cancerres.aacrjournals.org on August 11, 2017. © 1995 American Association for Cancer
Research.
Chemosensitivity Testing of Human Tumors Using a Microplate
Adenosine Triphosphate Luminescence Assay: Clinical
Correlation for Cisplatin Resistance of Ovarian Carcinoma
Peter E. Andreotti, Ian A. Cree, Christian M. Kurbacher, et al.
Cancer Res 1995;55:5276-5282.
Updated version
E-mail alerts
Reprints and
Subscriptions
Permissions
Access the most recent version of this article at:
http://cancerres.aacrjournals.org/content/55/22/5276
Sign up to receive free email-alerts related to this article or journal.
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Department at [email protected].
To request permission to re-use all or part of this article, contact the AACR Publications
Department at [email protected].
Downloaded from cancerres.aacrjournals.org on August 11, 2017. © 1995 American Association for Cancer
Research.