Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
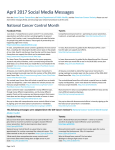
Serving Adolescents and Young Adults: What We’re Doing at USC and Other Institutions in the U.S. Your speaker • • • • Melanie Goldfarb, M.D. Endocrine Surgeon USC / Norris Comprehensive Cancer Center AYA “Thyroid champion” for the USC AYA program What were going to talk about • AYA cancers – Introduction – What is AYA ? – Challenges, uniqueness of AYA cancers & patients – AYA nationwide; AYA@USC • AYA Thyroid cancers – What little we know – Historical philosophy for diagnosis and treatment – Areas for research What is AYA ? What is AYA ? • Describes cancers among Adolescents and Young Adult population ages 15 – 39 • Currently 65,000 – 70,000 AYA cancers diagnosed each year in the US – Over 4,000 AYA cancers in Los Angeles basin alone • Cancer is the this age group’s leading disease-related cause of death What are Common “AYA” Cancers? Ages 15-29 Top 3 Cancer incidence is illustrated in (Top) females and (Bottom) males ages 15 to 29 years in the US. Surveillance, Epidemiology, and End Results (SEER) database from 1995 to 2000 (Bleyer A, O’Leary M, Barr R, Ries LAG, eds. NIH Pub. No. 06-5767. #4 #4 25- to 29 year olds #4 AYA patients are unique Life transitions • Adolescence ► Young Adult ►Adulthood – Shifts in family and peer groups – Changing and evolving sexual health and relationships – Growing independence – Highly mobile Independence • Newfound independence and self awareness + feelings of invincibility and invulnerability – Reduced adherence to treatment & follow-up – Increased likelihood of late stage diagnosis – Challenges in communication • AYA – family • AYA – physician • AYA – peers • Family - physician 11 Unique needs • Disruptions in education, employment, and social life • Questions about future fertility • Establishing financial independence • Navigating the health care system • Very premature confrontation with mortality • Changes in physical appearance • “Long-term follow-up” is really long-term • Pregnant or a new parent Survivorship • The majority of AYA patients become longterm survivors with many potential years of life ahead of them Survivorship • High-risk population with the potential to develop a wide array of late effects – For many late effects the risk does not plateau with aging – Usually a clinically silent period with intervals as long as 2 to 3 decades – Desire to escape the trauma of their cancer experience may mean that AYA survivors do not follow-up with their health care; they are hoping to put the experience of being sick behind them System challenges of treating the AYA population Lack of Dedicated AYA centers • Very few pediatric and adult centers have programs that assist AYA patients – Unable to address the many unique needs of AYA • Very few centers have reserved inpatient and outpatient space – AYA patients are surrounded by patients much older or younger than themselves – Increases sense of isolation and reinforces their perception of being different from their peers Access to care • Higher rates of being unemployed, under- or uninsured • Lack of a primary care physician • Difficulty in obtaining appropriate referral • Continuum of access to care Lack of Research & clinical trials Enrollment in clinical trials lags greatly among AYA population: A very similar experience to pediatric cancers in the 1970’s. AYA Participation in US Clinical Trials (A. Bleyer) Research and clinical trials??? • • • • Mobile population – difficult to track “Avoidance” of the issue in AYA patients Not want further disruptions to their life Not appreciate need for follow-up and research • Companies and centers have not recognized the need for dedicated AYA trials and research AYA nationwide AYA programs in the US • Only a handful of established programs – Most in early stages of development 21 AYA programs in the US Ages 15-29 Ages 18-39 Ages 15-39 Ages 15-29 Ages 15-25 Ages 15-39 Ages 15-21 Ages 15-30 22 AYA community is growing • • • • • • • • • • • www.ihadcancer.com www.stupidcancer.com www.planetcancer.org www.15-40.org http://www.facebook.com/ayacancer http://www.teenslivingwithcancer.org http://www.livestrong.org/ http://www.ulmanfund.org http://www.youngcancerspouses.org/ http://www.pregnantwithcancer.org/ http://imermanangels.org/index.php 23 AYA in the media Goals of Risk-Based Healthcare of AYA Cancer Survivors • Multidisciplinary team approach with communication between the primary healthcare provider, specialists of pediatric and adult medicine, and allied/ancillary service providers • Healthcare of the whole person, not a specific disease or organ system, including individual’s family, cultural & spiritual values • Sensitivity to the issues of the cancer experience, including expressed and unexpressed fears of the survivor • Comprehensive, anticipatory, proactive care that includes a systematic plan of prevention and surveillance • Longitudinal care that is considered a continuum from cancer diagnosis to eventual death, regardless of age • Continuity of care consisting of a partnership between the survivor and a single healthcare provider or program who can coordinate necessary services Oeffinger KC. Curr Probl Cancer. 2003;27:143-167. Empowering the AYA patient • Individual self-advocacy – Seeks out information – Communicates with their healthcare team as an equal partner – Is involved in their treatment decisions • Regional and national advocacy – Community building: like-minded individuals connect and support each other – Combine efforts of family, community, and societal members to promote awareness and change AYA@USC • USC/CHLA will have the largest AYA program in Southern California • USC’s program will be the only NCI designated comprehensive cancer center with an AYA program in California and the Southwestern US • www.uscnorris.com/about/programs/aya.html Goals • Establish a cooperative, multi-disciplinary, patientcentered care model to treat the AYA patient • Improve AYA patient population’s quality and survival outcomes • Develop a robust research program emphasizing basic, clinical, and translational research • Create models of care, best practices, and protocols for treating and curing the AYA patient • Emphasize the knowledge transfer and education of healthcare professionals on AYA • Communicate and raise awareness to the USC and Los Angeles basin communities about AYA Services for AYA patients and families • Overall disease education • Anxiety and depression • Reproductive Health including fertility preservation • Genetic counseling – Tumor – Family history • Physical and Occupational tx – Group/ Individual Support • Peer • Family • Friends • Spousal • Children – Relationship health – Financial resource planning – Religious/ Faith needs – Employment and educational counseling – Peer / Professional Networking – Pain management – Dietary and nutrition needs – Legal AYA “Collaborative” Model: Integrated Research Core • Collaborative relationship with AYA Care Team – AYA Patient Coordinator, nursing staff – AYA Medical director – Psychosocial services – Support services – Survivorship • Integrated Clinical, Basic, and Population studies • Emphasis on quality outcomes through strengthened clinical care and psycho-social support AYA Thyroid Cancers What little we know…. • Mean age at presentation for all thyroid cancers is 3rd decade (AYA) • Younger (<20) (AYA) and older (>60) present with more extensive disease • ONLY cancer where age (< 40 or 45) is part of staging!! (AYA) In all age groups… • Thyroid cancer is increasing • Majority are papillary or a follicular variant • Excellent overall survival • Females better long-term survival vs males Risk Factors • Most important risk factor is a history of head and neck radiation, especially at very young ages – In a study of 16,500 leukemia survivors, thyroid carcinoma was #1 second malignancy in patients with a history of HD and NHL and #3 in patients with a history of leukemia (Maule et al, 2007). – 53X increase risk at 2 years from initial cancer dx (Tucker et al, 1991) – Cancer risk continues for up to 30 years – Average latency period 8.4 years (Winship & Rosvoll, 1970) Thyroid nodules • 13% in autopsy studies ages 18-39 (AYA) (Oertel, Humana Press 2000) – 1.5% young kids and up to 70% in adults • About 25% of “pediatric” thyroid nodules (< 21 yrs old) are malignant – 4-5X increased incidence of malignancy compared to adults – ? AYA But… • Almost all studies are done in either the “adult” (≥ 18 or 21 years old) or “pediatric” age group (≤ 18 or 21 years old) • It’s difficult to tease out AYA specific conclusions Where does AYA fit ? Comparison of children and adults with PTC Parameter Children (%) Adults (%) p DNA nondiploid 10 25 0.047 Nodal metastases 90 35 0.001 Extrathyroidal invasion 24 16 0.100 Distant metastases 7 2 0.001 Local soft tissue recurrence 12 5 0.080 Regional nodal recurrence 30 7 0.001 Late distant metastases 6 5 1.000 • Greater PTC causal mortality in patients > 40 years old Zimmerman et al 1988 Historical philosophy for diagnosis and treatment Importance of age – Staging and Prognosis Importance of age • Young patients (<20 years old) – Thyroid more sensitive to external radiation – Tumors more likely to be sensitive to RAI – Tumors “classic”/solid variant > regular PTC – Genetic mutations: RET/PTC > BRAF – Increased recurrence rate – Higher survival rate – Higher rates of lymph node involvement, multicentricity, distant mets Importance of age • 20 - 44 years old – Generally low-risk patients – Lower recurrence rates – RAI sensitive tumors AYA paper • Differences in expression in a few candidate genes • But no distinct difference in cluster gene profiles or number of mutations Menno R. Vriens, et al. Clinical and Molecular Features of Papillary Thyroid Cancer in Adolescents and Young Adults Treatment strategy in 2011 The basics *** Surgeon Performed Head and Neck Ultrasound *** • Neck ultrasound has become an extension of the physical exam for many clinicians • Information on: size, shape, composition of nodules, other thyroid lobe for additional nodule,; suspicious lymph nodes • Preoperative planning Surgery • Total thyroidectomy - ? tumors < 1cm • Lymph nodes ? – Any suspicious LN on ultrasound in conjunction with a suspicious nodules is cancer until proven otherwise – No “berry picking” of lymph nodes – Controversy over routine central neck dissection • Cosmetically favorable incision Post-op care • Thyroid hormone suppression • RAI ??? – Definitely for extensive disease – Controversy over “low-risk” group – most of AYA Areas for research in AYA Thyroid Cancer Questions • Initial presentation – Are more nodules self-discovered ? – Are there longer times from first “symptom” to diagnosis? (differences in “access to care”; maybe AYA patients less likely to have PCP or insurance) Questions • History of head and neck radiation – How often to screen – Different tumors? – Do screening modalities work the same (ultrasound characteristics and FNA biopsy) Questions • Does everyone need post-operative RAI? – Risk vs benefit – Can molecular markers play a role in risk assessment – How often and how to screen for second malignancies RAI and second malignancies Anna M. Sawka et al. Second Primary Malignancy Risk After Radioactive Iodine Treatment for Thyroid Cancer: A Systematic Review and Meta-analysis RAI and second malignancies N. Gopalakrishna Iyer, et al. Rising Incidence of Second Cancers in Patients With LowRisk (T1N0) Thyroid Cancer Who Receive Radioactive Iodine Therapy In 2005, close to 70% of low-risk cancer patients getting RAI therapy Last 20 years, rates second malignancy, especially leukemia, greatly increased Questions • Why are AYA thyroid cancers different? – Effect of estrogen ? – Genetic mutations ? – Intrinsic biological difference in thyroid gland ? – Better immune system ? Summary • AYA: patients 15-39 years old • “Overlooked” patient population • AYA patients have – Different predominant cancer types (Thyroid) – Unique needs surrounding their cancer care – Unique tumor biology • Benefit from a multidisciplinary care approach Thank You