Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
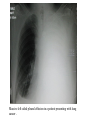
Case study A 70-year-old women presents with slowly increasing dyspnoea. She cannot lie flat without feeling more short of breath. She has a history of HTN and osteoarthritis, and she has been taking NSAIDs with increasing frequency over the previous few months. On physical examination, she appears dyspnoeic at rest, her BP is 140/90 mm Hg, and pulse is 90 bpm. Her jugular venous pressure is elevated to the angle of the jaw. The left lung field is dull to percussion with decreased air entry basally. Crackles are heard in the right lung field and above the line of dullness on the left. Lower extremities have pitting oedema to the knee. Pleural fluid •The pleural cavity is a potential space lined by mesothelium of the visceral and parietal pleurae. •The pleural cavity normally contains a small amount of fluid. •This fluid is a plasma filtrate derived from capillaries of the parietal pleura. •It is produced continuously at a rate dependent on capillary hydrostatic pressure, plasma oncotic pressure, and capillary permeability •Pleural fluid is reabsorbed through the lymphatics and venules of the visceral pleura. •An accumulation of fluid, called an effusion, results from an imbalance of fluid production and reabsorption. •Excessive amounts of such fluid can impair breathing by limiting the expansion of the lungs during ventilation . Types of fluids Four types of fluids can accumulate in the pleural space: 1. Serous fluid (hydrothorax) 2. Blood (haemothorax( 3. Chyle (chylothorax) 4. Pus (pyothorax or empyema( Diagnosis • Pleural effusion is usually diagnosed on the basis of medical history and physical exam ,and confirmed by chest x-ray . • Once accumulated fluid is more than 300 ml, there are usually detectable clinical signs in the patient, such as 1. Decreased movement of the chest on the affected side, 2. Stony dullness to percussion over the fluid, 3. Diminished breath sounds on the affected side, 4. In large effusion there may be tracheal deviation away from the effusion . Imaging A pleural effusion will show up as an area of whiteness on a standard posteroanterior X-ray . Chest radiographs acquired in the lateral decubitus position (with the patient lying on his side) are more sensitive and can pick up as little as 50 ml of fluid. At least 300 ml of fluid must be present before upright chest films can pick up signs of pleural effusion (e.g., blunted costophrenic angles) Massive left sided pleural effusion in a patient presenting with lung cancer . CT scan of chest showing loculated pleural effusion in left side. Some thickening of pleura is also noted . SPECIMEN COLLECTION Thoracentesis is indicated for any undiagnosed pleural effusion or for therapeutic purposes in patients with massive symptomatic effusions; • • A needle is inserted through the back of the chest wall in the sixth, seventh, or eighth intercostal space on the midaxillary line, into the pleural space. The fluid may then be evaluated for the following: 1. Chemical composition including protein ,lactat dehydrogenaseLDH , albumin ,amylase ,pH ,and glucose. 2. Gram stain and culture to identify possible bacterial infections 3. Cell count and differential 4. Cytopathology to identify cancer cells, some infective organisms 5. Other tests as suggested by the clinical situation – lipids ,fungal culture ,viral culture ,specific immunoglobulins Contraindications • An uncooperative patient or a coagulation disorder that can not be corrected are absolute contraindications • Relative contraindications include cases in which the site of insertion has known bullous disease (e.g .emphysema( and use of mechanical ventilation. TRANSUDATES AND EXUDATES Transudates are usually bilateral owing to systemic conditions leading to increased capillary hydrostatic pressure or decreased plasma oncotic pressure Exudates are more often unilateral, associated with localized disorders that increase vascular permeability or interfere with lymphatic resorption Classical teaching stressed that exudates and transudates can be distinguished on the basis of total protein concentrations above (exudates) or below (transudates) 3.0 g/dL Accordingly, an exudate meets one or more of the following criteria: (1) Pleural fluid/serumv protein ratio greater than 0.5; (2) pleural fluid/serum LD ratio greater than 0.6; and (3) pleural fluid LD level greater than two thirds of the serum upper limit of normal. GROSS EXAMINATION Transudates are typically clear, pale yellow to straw-colored, and odorless, and do not clot. Approximately 15% of transudates are blood tinged. A bloody pleural effusion (hematocrit >1%) suggests trauma, malignancy, or pulmonary infarction. A pleural fluid hematocrit greater than 50% of the blood hematocrit is good evidence for a hemothorax Exudates may grossly resemble transudates, but most show variable degrees of cloudiness or turbidity, and they often clot if not heparinized. A feculent odor may be detected in anaerobic infections. Turbid, milky, and/or bloody specimens should be centrifuged and the supernatant examined. If the supernatant is clear, the turbidity is most likely due to cellular elements or debris. If the turbidity persists after centrifugation, a chylous effusion is likely. MICROSCOPIC EXAMINATION Cell Counts Leukocyte counts have limited utility in separating transudates (<1000/μL) from exudates (>1000/μL). Although red cell counts above 100,000/μL are highly suggestive of malignancy, trauma, or pulmonary infarction, they are not specific for these conditions. Differential Leukocyte Count and Cytology Cytologic analysis will establish the diagnosis of metastatic carcinoma in 70% or more of cases