Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
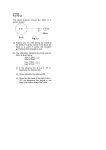
Proton Beam Range Verification using Proton Activated Fiducials and Off-site PET J Cho, G Ibbott, M Gillin, C Gonzalez-Lepera, U Titt and O Mawlawi The University of Texas MD Anderson Cancer Center, Houston, TX AAPM Best in Physics, Indianapolis, 2013 Talk session: Novel Imaging Tech & Appl 4:40PM August 7th (Wed) at 500 Ballroom In-Air Irradiation Motivations Embedded Irradiation: Lung tissue 30 min PET scan after 126 min delay The conventional proton range verification using PET takes advantage of endogenous tissue activation in combination with Monte Carlo simulation. However, this approach has the following limitations: Weak tissue activation at the end of the proton beam Perfusion driven activity washout Short decay half-life (need of costly in-room PET) Monte Carlo uncertainties in Elemental tissue composition conversion Nuclear cross sections Biological washout model The purpose of this work was to develop a novel proton range verification method that is not subject to the above limitations. By taking advantage of patient-implantable fiducial markers that are strongly activated by low energy protons and decay with relatively long half-lives, a proton range verification can be realized using commonly available off-site PET scanners. (a) (a) (a) (b) Fig. 2: 68Zn and 63Cu have large cross sections at low proton energies and decay with relatively long half-lives. As a result, they are activated strongly at the proton distal fall-off region where proton energy is low. Endogenous tissue elements (12C and 16O) are shown for comparison. Fig. 4: 68Zn (98% enriched) and Cu foils and polycarbonate sheets (as a tissue substitute) are placed at 4 distal fall-off depths and irradiated by a proton beam. Cu has 69% 63Cu. (b) Fig. 7: (a) Balsa wood (as lung substitute) with embedded 68Zn and Cu foils at 4 distal fall-off depths and irradiated by a proton beam. (b) CT scan and treatment plan of the balsa wood show isodose curves relative to each depth. Fig. 9: (a) Foil locations relative to PDD. (b) Foil at depth 4 is marginally activated and foil at depth 5 is not activated. Therefore, the proton range can be estimated with ±5mm uncertainty. (b) Fig. 11: A coronal plane view with a row of 25mm3 Cu foils. (a) PET/CT fusion images. (b) Treatment plan generated isodose curves with respect to CT image. With the borderline of 95% isodose curve, Cu foils located at higher dose are activated. Embedded irradiation: Soft tissue Parodi et al, NIH public access 2007 30 min PET scan after 48 min delay Background Fig. 5: Depths of PC (polycarbonate), 68Zn and Cu relative to PDD and their PET/CT fusion images. Only 68Zn and 63Cu show PET signals at deeper depths (not PC). 68Zn and 63Cu signals are strong despite its volume is 7.6 times smaller than PC. (a) Fig. 1: Proton range uncertainty can result in overdosage in critical organs or underdosage in tumor. It is crucial to verify the proton range accurately. (a) Conclusions (b) Fig. 3: Hypothetical images of proton activated fiducial markers made of 68Zn or 63Cu implanted in a patient prior to proton therapy. (a) One marker is implanted near the proton distal falloff and one just outside the proton range. (b) The marker implanted near the distal fall-off is activated (red) and the other marker outside the proton range is not activated (green). In this regard, the proton range can be approximated to be fall somewhere between the two fiducials. Signal reduced (b) Fig. 6: Comparison of measured PDD and activity (PET signal) with Monte Carlo simulation. Activity fall-offs follow the dose fall-off with 1~2 mm offsets. Fig. 8: PET/CT fusion images of each depth in the beam’s eye view. Signals from foils are much stronger than balsa wood. Signals are reduced with depth. Foil is marginally activated at depth 4. Fig. 12: A coronal plane view with a row of 25mm3 68Zn foils. With the borderline of 50% isodose curve, 68Zn foils located at higher dose are activated. Foil 1 is not activated because protons activating this foil is too high (see fig. 2). Fig. 10: (a) Soft-tissue phantom made of beef cut diagonally is embedded with 68Zn and Cu foils and is irradiated by a proton beam. Each of 5 different coronal planes contains a different row of foils. (b) Locations of embedded foils relative to PDD. Higher activation of 68Zn and Cu at the proton dose distal fall-off region and their long half-lives indicate the possibility of using those materials as patient implantable fiducial markers for proton range verification using off-site PET scanners.