Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Traveler's diarrhea wikipedia , lookup
History of virology wikipedia , lookup
Staphylococcus aureus wikipedia , lookup
Bacterial morphological plasticity wikipedia , lookup
Germ theory of disease wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Bacterial cell structure wikipedia , lookup
Triclocarban wikipedia , lookup
Human microbiota wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Gastroenteritis wikipedia , lookup
Hepatitis B wikipedia , lookup
Schistosomiasis wikipedia , lookup
Infection control wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Anaerobic infection wikipedia , lookup
Urinary tract infection wikipedia , lookup
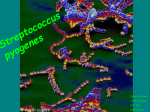
P.O. Box 131375, Bryanston, 2074 Ground Floor, Block 5 Bryanston Gate, 170 Curzon Road Bryanston, Johannesburg, South Africa 804 Flatrock, Buiten Street, Cape Town, 8001 www.thistle.co.za Tel: +27 (011) 463 3260 Fax: +27 (011) 463 3036 Fax to Email: + 27 (0) 86‐557‐2232 e‐mail : [email protected] Please read this bit first The HPCSA and the Med Tech Society have confirmed that this clinical case study, plus your routine review of your EQA reports from Thistle QA, should be documented as a “Journal Club” activity. This means that you must record those attending for CEU purposes. Thistle will not issue a certificate to cover these activities, nor send out “correct” answers to the CEU questions at the end of this case study. The Thistle QA CEU No is: MT- 13/00142. Each attendee should claim THREE CEU points for completing this Quality Control Journal Club exercise, and retain a copy of the relevant Thistle QA Participation Certificate as proof of registration on a Thistle QA EQA. MICROBIOLOGY LEGEND CYCLE 33 – ORGANISM 4 STREPTOCOCCUS PYOGENES Streptococcus pyogenes is a spherical, Gram-positive bacterium that is the cause of group A Streptococcal infections. S. pyogenes displays Streptococcal group A antigen on its cell wall. S. pyogenes typically produces large zones of beta-hemolysis when cultured on blood agar plates, and are therefore also called Group A (beta-hemolytic) Streptococcus (GABHS). Streptococci are catalase-negative. In ideal conditions, S. pyogenes has an incubation period of approximately 1–3 days. Gram stain of Streptococcus pyogenes Colonies of Streptococcus pyogenes on blood agar exhibiting beta (clear) hemolysis Streptococcus pyogenes is one of the most frequent pathogens of humans. It is estimated that between 5-15% of normal individuals harbour the bacterium, usually in the respiratory tract, without signs of disease. As normal flora, S. pyogenes can infect when defences are compromised or when the organisms are able to penetrate the constitutive defences. When the bacteria are introduced or transmitted to vulnerable tissues, a variety of types of suppurative infections can occur. Thistle QA is a SANAS accredited organisation, No: PTS0001 Accredited to ISO 17043 Certificate available on request or at www.sanas.co.za Page 1 of 3 P.O. Box 131375, Bryanston, 2074 Ground Floor, Block 5 Bryanston Gate, 170 Curzon Road Bryanston, Johannesburg, South Africa 804 Flatrock, Buiten Street, Cape Town, 8001 www.thistle.co.za Tel: +27 (011) 463 3260 Fax: +27 (011) 463 3036 Fax to Email: + 27 (0) 86‐557‐2232 e‐mail : [email protected] Classification of Streptococci Hemolysis on blood agar The type of haemolytic reaction displayed on blood agar has long been used to classify the streptococci. Beta-haemolysis is associated with complete lysis of red cells surrounding the colony, whereas alpha-haemolysis is a partial or "green" haemolysis associated with reduction of red cell haemoglobin. Non haemolytic colonies have been termed gamma-haemolytic. Haemolysis is affected by the species and age of red cells, as well as by other properties of the base medium. Group A Streptococci are nearly always beta-haemolytic; related Group B can manifest alpha, beta or gamma haemolysis. Most of the oral Streptococci and Enterococci are non haemolytic. The property of haemolysis is not very reliable for the absolute identification of Streptococci, but it is widely used in rapid screens for identification of S. pyogenes. Antigenic types The cell surface structure of Group A Streptococci is among the most studied of any bacteria. The cell wall is composed of repeating units of N-acetylglucosamine and N-acetylmuramic acid, the standard peptidoglycan. Historically, the definitive identification of Streptococci has rested on the serologic reactivity of "cell wall" polysaccharide antigens as originally described by Rebecca Lancefield. Eighteen group-specific antigens (Lancefield groups) were established. The Group A polysaccharide is a polymer of N-acetylglucosamine and rhamnose. Some group antigens are shared by more than one species. This polysaccharide is also called the C substance or group carbohydrate antigen. Diagnosis Usually, a throat swab is taken to the laboratory for testing. A Gram stain is performed to show Gram-positive cocci in chains. Then, the organism is cultured on blood agar with an added bacitracin antibiotic disk to show beta-hemolytic colonies and sensitivity (zone of inhibition around the disk) for the antibiotic. It is then cultured on non-blood containing agar; the catalase test is performed which should show a negative reaction for all Streptococci. S. pyogenes is CAMP and hippurate tests negative. Serological identification of the organism involves testing for the presence of group A specific polysaccharide in the bacterium's cell wall using the Phadebact test. Pathogenesis Streptococcus pyogenes owes its major success as a pathogen to its ability to colonize and rapidly multiply and spread in its host while evading phagocytosis and confusing the immune system. Acute diseases associated with Streptococcus pyogenes occur chiefly in the respiratory tract, bloodstream, or the skin. Streptococcal disease is most often a respiratory infection (pharyngitis or tonsillitis) or a skin infection (pyoderma). Some strains of streptococci, show a predilection for the respiratory tract; others for the skin. Generally, streptococcal isolates from the pharynx and respiratory tract do not cause skin infections. Thistle QA is a SANAS accredited organisation, No: PTS0001 Accredited to ISO 17043 Certificate available on request or at www.sanas.co.za Page 2 of 3 P.O. Box 131375, Bryanston, 2074 Ground Floor, Block 5 Bryanston Gate, 170 Curzon Road Bryanston, Johannesburg, South Africa 804 Flatrock, Buiten Street, Cape Town, 8001 www.thistle.co.za Tel: +27 (011) 463 3260 Fax: +27 (011) 463 3036 Fax to Email: + 27 (0) 86‐557‐2232 e‐mail : [email protected] S. pyogenes is the leading cause of uncomplicated bacterial pharyngitis and tonsillitis commonly referred to as strep throat. Other respiratory infections include sinusitis, otitis, and pneumonia. Infections of the skin can be superficial (impetigo) or deep (cellulitis). Invasive streptococci cause joint or bone infections, destructive wound infections (necrotizing fasciitis) and myositis, meningitis and endocarditis. Two post streptococcal sequelae, rheumatic fever and glomerulonephritis, may follow streptococcal disease, and occur in 1-3% of untreated infections. These conditions and their pathology are not attributable to dissemination of bacteria, but to aberrant immunological reactions to Group A Streptococcal antigens. Scarlet fever and streptococcal toxic shock syndrome are systemic responses to circulating bacterial toxins. Treatment and prevention Penicillin is still uniformly effective in treatment of Group A Streptococcal disease. It is important to identify and treat Group A Streptococcal infections in order to prevent sequelae. No effective vaccine has been produced, but specific M-protein vaccines are being tested. Frequency Infections with group A Streptococcus are observed worldwide. Prevalence of Streptococcal pyoderma is higher in regions near the tropics. Aside from this observation, no geographic barriers to infection with this ubiquitous organism are recognized. Rheumatic fever is most frequently observed in the age group most susceptible to group A Streptococcal infections (i.e., children aged 5-15 y). The attack rate following upper respiratory tract infection is approximately 3% in individuals with untreated or inadequately treated infection. Mortality/Morbidity Infection with group A Streptococci leads to various clinical manifestations responsible for considerable morbidity and, with increasing frequency, mortality. In addition, infection with this organism leads to postsuppurative sequelae, particularly acute rheumatic fever and post streptococcal glomerulonephritis (PSGN). References 1. Todar’s Online Textbook of Bacteriology – Kennet Todar PHD 2. EMedicine Paediatrics – Mark R Schleiss 3. http://en.wikipedia.org/wiki/Streptococcus_pyogenes Questions 1. What are the morphological characteristics of Streptococcus pyogenes? 2. Discuss the classification and pathogenesis of Streptococcus pyogenes. 3. What is the recommended treatment for Streptococcus pyogenes? Thistle QA is a SANAS accredited organisation, No: PTS0001 Accredited to ISO 17043 Certificate available on request or at www.sanas.co.za Page 3 of 3