Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
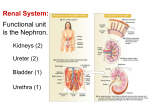
INVESTIGATION OF RENAL AND URINARY TRACT DISEASE Tests of function Glomerular filtration rate (GFR) GFR is the rate at which fluid passes into nephrons after filtration and measures renal excretory function. GFR is proportionate to body size so the reference range is usually expressed after correction for body surface area as 120 ± 25 mL/min/1.73 m2. Direct measurement of GFR by injecting and measuring the clearance of compounds that are completely filtered and not reabsorbed by the nephron (inulin, radiolabelled ethylenediamine-tetraacetic acid (EDTA)) is inconvenient and is usually reserved for special circumstances (e.g. for potential live kidney donors). Serum levels of endogenous compounds excreted by the kidney give useful information. Blood urea is not the best test, as it increases with high protein intake (including absorption of blood from the gut after a gastrointestinal haemorrhage) and in catabolic states, and is reduced in liver failure (low production from protein) and anorexia or malnutrition (low protein intake). Serum creatinine reflects GFR more reliably than urea, as it is produced from muscle at a constant rate and almost completely filtered at the glomerulus. If muscle mass remains constant, changes in creatinine concentration reflect changes in GFR . However, the reference range for creatinine values is wide because of variations in muscle mass; in patients with low muscle mass (e.g. the elderly) serum creatinine may not be above the reference range until GFR is reduced by > 50%. Measuring GFR • Direct measurement using labelled EDTA or inulin • Creatinine clearance (CrCl) – Minor tubular secretion of creatinine causes CrCl to exaggerate GFR when renal function is poor, and can be affected by drugs (e.g. trimethoprim, cimetidine) – Needs 24-hr urine collection (inconvenient and often unreliable) Estimating GFR with equations • Cockcroft and Gault (C&G) equation – Reasonably accurate at normal to moderately impaired renal function – Estimates CrCl, not GFR – Requires patient weight The Modification of Diet in Renal Disease (MDRD) study equation – Performs better than C&G at reduced GFR – Requires knowledge of age and sex only – Can be reported automatically by laboratories Urinalysis Examination of an aliquot of urine provides important information on kidney function. Dipsticks may be used to screen for blood and protein semi-quantitatively . Urine microscopy can detect red cells of glomerular origin and red cell casts, indicative of intrinsic renal disease. Flow cytometry can also be used to screen for white blood cells and bacteria. Crystals (e.g. of calcium oxalate, cysteine or urate) may be seen in renal calculus disease, although calcium oxalate and urate crystals are also sometimes found in normal urine that has been left to stand. Urine pH can provide diagnostic information in the assessment of renal tubular acidosis , and a persistently low specific gravity may be found in diabetes insipidus . Timed (usually 24-hour) urine collections are now used less often to measure GFR or protein excretion , but are still required to measure excretion rates of sodium and of solutes that can form renal calculi such as calcium, oxalate and urate . Other dynamic tests of tubular function, including concentrating ability , ability to excrete a water load and ability to excrete acid , are valuable in some circumstances. Imaging techniques Plain X-rays may show the renal outlines (if perinephric fat and bowel gas shadows permit), opaque calculi and calcification within the renal tract. Ultrasound This quick, non-invasive technique is the first and often the only method required for renal imaging. It can show renal size and position, detect dilatation of the collecting system , distinguish tumours and cysts, and show other abdominal, pelvic and retroperitoneal pathology. Doppler techniques can show blood flow in extrarenal and larger intrarenal vessels. The resistivity index is the ratio of peak systolic and diastolic velocities, and is influenced by the resistance to flow through small intrarenal arteries. It may be elevated in various diseases, including acute glomerulonephritis and rejection of a renal transplant In addition, it can image the prostate and bladder, and estimate completeness of emptying in suspected bladder outflow obstruction. In CKD ultrasonographic density of the renal cortex is increased and corticomedullary differentiation is lost. However, renal ultrasound is operatordependent, and it is often less clear in obese patients. Intravenous urography (IVU) While intravenous urography has been largely replaced by ultrasound and/or CT urography for routine renal imaging, the technique provides excellent definition of the collecting system and ureters, and remains superior to ultrasound for examining renal papillae, stones and urothelial malignancy . The disadvantages of this technique are the need for an injection, time requirement, dependence on adequate renal function, and exposure to irradiation and contrast medium Renal arteriography and venography The main indication for renal arteriography is to investigate suspected renal artery stenosis or haemorrhage. Therapeutic balloon dilatation and stenting of the renal artery may be undertaken, and bleeding vessels or arteriovenous fistulae occluded. Computed tomography (CT) CT is particularly useful for characterising mass lesions within the kidney , or combinations of cysts with masses. It gives clear definition of retroperitoneal anatomy regardless of obesity. Even without contrast medium it is better than IVU for demonstrating renal stones. In CT urography, after a first scan without contrast, scans are repeated during nephrogram and excretory phases. This gives more information but entails a substantially larger radiation dose than IVU. Magnetic resonance imaging (MRI) • MRI offers excellent resolution and distinction between different tissues . Magnetic resonance angiography (MRA) uses gadolinium-based contrast media, which may carry risks for patients with very low GFR . MRA can produce good images of main renal vessels but may miss branch artery stenoses. Radionuclide studies These are functional studies requiring the injection of gamma ray-emitting radiopharmaceuticals which are taken up and excreted by the kidney, a process which can be monitored by an external gamma camera. Renal biopsy Indications • Acute renal failure that is not adequately explained • CKD with normal-sized kidneys • Nephrotic syndrome or glomerular proteinuria in adults • Nephrotic syndrome in children that has atypical features or is not responding to treatment • Isolated haematuria or proteinuria with renal characteristics or associated abnormalities • • • • Contraindications Disordered coagulation or thrombocytopenia. Aspirin and other antiplatelet agents increase bleeding risk Uncontrolled hypertension Kidneys < 60% predicted size Solitary kidney (except transplants) (relative contraindication) • • • • Complications Pain, usually mild Bleeding into urine, usually minor but may produce clot colic and obstruction Bleeding around the kidney, occasionally massive and requiring angiography with intervention, or surgery Arteriovenous fistula, rarely significant clinically Thank you