Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
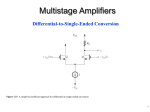
[CANCER RESEARCH 42. 2906-2908, 0008-5472/82/0042-OOOOS02.00 July 1982] Normal Sister Chromatid Exchange Frequency in Long-Term Survivors with Acute Leukemia1 Susumu Inoue2, Laura Brown, Yaddanapudi Ravindranath, and Mark J. Ottenbreit Children s Hospital of Michigan [S. I., L. B., Y. R.¡,and Department Michigan 48201 of Pediatrics, ABSTRACT We hypothesized that the sister chromatid exchanges assay in acute leukemia long-term survivors may detect: (a) long-term effects of combined chemo- and radiotherapy; and possibly (b) those individuals with inherently deficient DMA repair. Accord ingly, we determined the sister chromatid exchanges frequency in 26 blood specimens from 24 acute leukemia long-term survivors (patients) and 14 blood specimens from 13 control subjects (controls). The patients consisted of 23 children with acute lymphocytic and one child with acute myelocytic leuke mia. The median length of chemotherapy was 5 years. Eighteen of the 24 patients also received prophylactic fractional central nervous system irradiation for the first 3 years of treatment, and one patient received therapeutic irradiation to the central nervous system. The median off-therapy period at the time of study was 2.5 years with a range of 0 to 7.5 years. The controls consisted of the parents of the patients and laboratory personnel. A mean exchange score per cell was established for each specimen (25 to 30 cells/specimen were scored), and it ranged from 3.0 to 9.7 in the patients and from 3.0 to 11.5 in the controls. A mean ± S.D. calculated from those means was 6.0 ±1.8 for the patients and 6.9 ±2.8 for the controls. They were not significantly different. We conclude that chemo- and radiotherapy produced no persistent DMA alterations detectable by this method. INTRODUCTION Prognosis of ALL3 in children has improved markedly, and more than 50% of the patients now achieve long uninterrupted remission and are taken off chemotherapy (16). About 15% of these children, however, relapse following the cessation of therapy (16). The majority of these relapses is presumed to be a relapse of the original leukemia. An alternative mechanism of a relapse would be a new mutation or cancer transformation after the original leukemic cells were completely irradicated. That this could occur has been amply documented in the literature (3, 4,13,19). It could be hypothesized that some of the relapses that occur after cessation of treatment may be in reality due to the emergence of a new leukemic clone, as opposed to the resurgence of the original leukemic cells. It has become evident recently that patients treated with chemother apy and/or radiotherapy for the primary cancer are at an increased risk of developing a second cancer, including leu' Supported by Children's Leukemia Foundation of Michigan. 2 To whom requests for reprints should be addressed, at: Children's Hospital of Michigan, 3901 Beaubien Boulevard, Detroit, Mich, 48201. 3 The abbreviations used are: ALL, acute lymphocytic leukemia; SCE, sister chromatid exchange. Received December 7. 1981; accepted March 30, 1982. 2906 Wayne State University School of Medicine [S. I., Y. R., M. J. O.], Detroit, kemia, suggesting that these therapy modalities were directly responsible for malignant mutation (3, 12, 18). In addition to the exogenous factors, "proneness" of the individual to de velop cancer (or genetic factors of considered. For example, so-called syndrome characterized by increased frequency, such as Fanconi's anemia the host) must also be chromosomal instability chromosome breakage or Bloom's syndrome, is an established heritable condition with an increased risk of cancer. Recent investigations of another chromosomal phenomenon, SCE, showed that the SCE assay would be a simple and sensitive assay system to determine mutagenicity of various carcinogens (extrinsic factors) (15, 20) and perhaps to detect DNA repair deficiency (one of the host factors) (20). If some of the relapses that occur after prolonged uninterrupted remission are due to a new mutation event, this could be due to: (a) prolonged exposure to chemotherapeutic agents and/or irra diation; (b) inherent susceptibility of the host to develop cancer repeatedly; or (c) a combination of both. We hypothesized that these factors, singly or in combination, may be reflected as an increased SCE frequency. We have conducted a prospective study to test this hypoth esis, and this paper describes our preliminary findings of this ongoing study. MATERIALS AND METHODS Study Population. The patient group consisted of 24 children with acute leukemia (all but one with ALL) who had been in remission for 5 years or longer and were no longer receiving any treatment at the time of study. These 24 patients received chemotherapy for 3 to 7.25 years with a median of 5 years. In addition, 19 of the 24 patients received prophylactic fractional central nervous system irradiation to the skull and spine (100 rads to each) every 10 weeks for the first 3 years (15 courses). Three of the patients had received 2 courses of chemotherapy because they relapsed while off treatment. At the time of the study, the off-therapy period ranged from 0.25 to 7.25 years with a median of 2.5 years. In 23 of the 24 patients, the chemotherapy consisted of a cyclic treatment of vincristine, 6-mercaptopurine, and prednisone alternated with p.o. mpthotrexate (Protocols I and II) (6). One patient received only p.o. 6-mercaptopurine, methotrexate, and prednisone (composite cyclic therapy) (6). Details of the patients are shown in Table 1. As of this writing, none of the patients relapsed. The control group consisted of 13 individuals (6 parents of the patients and 7 laboratory personnel). Method. Ten ml of heparinized blood were drawn, and the RBC were sedimented. The buffy coat cells were washed twice in a-medium and cultured in the dark in a-medium without thymidine with 20% fetal calf serum and with 25 fig 5-bromodeoxyuridine per ml of media for 3 days. Harvesting of the cells and preparation of the slides were made according to the method described previously (11). The slides were then exposed to fluorescent light for 15 min that was generated by an Osram HBO 220-watt high-pressure mercury lamp that was fitted to a CANCER RESEARCH Downloaded from cancerres.aacrjournals.org on August 3, 2017. © 1982 American Association for Cancer Research. VOL. 42 SCE in Leukemia Survivors Table 1 groupPatient12«3456a7891011121314a15161718192021222324DiagnosisALLALLALLALLALLALLALLALLALLALLALLALLALLALLALLALLALLALLALLALLALLALLALL Patient systemirradia oftreatment5yr8 tionYesYesYesYesYesYesYesYesYesYesYesYesYesYesYesYesYesYesYesNoNoNoNoNoOff-therapyperiod03 mos.5yr4 yr 6 mos.9 mos.1yr1 mos.5yr9yr5yr5yr3yr5yrSyr5yr4yr9yr5yr5yr5yr5yr5yr5 yr 6 yr1 mos.1 yr 6 mos.1 yr 8 mos.1 yr 9 mos.1 yr 9 mos.2yr2 yr 10 mos.2 yr 6 mos.2 yr 6 mos.2 yr 6 mos.3 yr 8 mos.3 yr 2 mos.3 yr 3 mos.3 yr 6 mos.4yr4 yr 6 mos.SyrSyr5 yr 10 mos.Syr7 yr 6 mos.7yr7yrCentralnervous yr 3 mos.6 yr 6 mos.7 yr 8 yr 6 mos.Range0-82-90-162-123-181-92-122-182-114-140-232-150-110-91-123-142-102-142-111-13 ±1.8° a In Cases 6 and 14, a bone marrow relapse; and in Case 2, a meningeal elapse occurred off therapy. A second course of chemotherapy and prophylactic irradiation were given in the former 2 and therapeutic irradiation were given in the third. Off-therapy period in these patients indicates the time after cessation of the second course. 6 AML, acute myelocytic leukemia. c Mean ±S.D. Zeiss microscope and filtered through a Zeiss BG12 filter. The slides were heated to 60° in 2-fold standard saline citrate (0.15 M sodium Table 2 Control group chloride:0.015 M sodium citrate, pH 7.4), for 2 hr and stained with Giemsa. At least 25 cells with a maximum of 30 cells were analyzed for the SCE frequency. SCE Range Mean Nonsmokers12345678910Smokers111213Control0-110-80-142-80-60-63-162-122-122-135-284-203 RESULTS The results are shown in Table 2. In summary, for the patient group, the mean SCE frequency for each specimen ranged from 3.0 to 9.7/cell. The mean ± S.D. of these individual means was 6.0 ±1.8. For the control group, the mean ranged from 3.0 to 11.5/cell. The mean ±S.D. for the control group was 6.9 ± 2.8. When the control group was divided into smokers (more than 1 pack/day) and nonsmokers, mean ± S.D. for the former was 10.7 ±0.6 and for the latter was 5.4 ± 1.5. The difference between the control smokers and nonsmokers was significant (p < 0.001). The difference between the patients and control nonsmokers was not significant (p > 0.3). 1.5a± 0.6± 2.8" Mean ±S.D. DISCUSSION It is currently unknown precisely what the SCE assay deter mines (7, 20). Of the 4 chromosome instability or DNA repair deficiency syndromes, Fanconi's anemia, Bloom's syndrome, ataxia telengiectasia, and xeroderma pigmentosum, only Bloom's syndrome is associated with increased spontaneous SCE incidence (2, 5, 7, 9, 20). This increase in SCE frequency, therefore, cannot be explained only on the basis of known DNA repair mechanism (20). Some agents, such as irradiation, that consistently cause chromatid and chromosomal breaks do not cause increased SCE. On the other hand, in the in vitro system, a concentration of chemicals that does not cause a significant number of breaks consistently raised the SCE frequency (15). In this regard, the SCE assay has been accepted widely as a more sensitive system to screen mutagens compared to break- JULY 1982 Downloaded from cancerres.aacrjournals.org on August 3, 2017. © 1982 American Association for Cancer Research. 2907 S. /noue ef a/. age analysis. Furthermore, in a Chinese hamster cell culture, the SCE incidence and the cell mutation rate proportionately increased with the progressively increasing doses of chemicals (1). We believe that the SCE assay is, in spite of the disadvan tages, the best and simplest assay system to test our hypoth esis. In this study, we found no patient with a significantly increased SCE frequency over that of controls. Although the mean age of controls (all adults) is much higher than that of patients, it was shown previously that sex and age have little influence on the SCE levels (5). As was reported by other investigators (8), control group smokers (more than a pack a day) exhibited a higher SCE rate compared to the nonsmokers. The past repetitious exposures to the chemotherapeutic drugs and craniospinal irradiation have not led to any increased frequency compared to the controls. This observation is con sistent with the findings reported by other workers (8, 14, 17). Otter ef al. (14) found an SCE frequency significantly higher than in controls in children with ALL before the beginning of treatment and while they were receiving the chemotherapy. However, in 4 ALL long-term survivors who were off treatment, their frequencies were comparable to the controls. Lambert ef al. (8) reported normal frequencies in the patients treated with 5-fluorouracil, vincristine, Adriamycin, cyclophosphamide, bleomycin, thioTEPA, methotrexate, and prednimustine. Ra posa (17) showed that cyclophosphamide treatment alone, or in combination with other drugs, induced an increased inci dence, but the frequency returned to the pretreatment level after 10 days. Our findings on SCE are in sharp contrast to the chromo somal breakage study reported by Miller ef al. (10). These authors reported a highly increased frequency in children who had been treated with chemo- or radiotherapy for primary cancers including leukemia, compared to their own pretherapy frequencies and the frequencies of their parents and siblings. The most prominent type of abnormality was translocation. Although the chemotherapeutic regimens and radiation dose used in these patients are not comparable to those in our series, a portion of their study population, namely the children with ALL, received roughly the same drug regimens as ours. The ALL patients like other patients in the series of Miller ef al. showed a much higher frequency of chromosomal aberration compared to the controls. An interesting finding in their report is that, while patients with Wilm's tumor and other cancers showed predominently translocation, aberrations in ALL pa tients were mainly simple deletions. The authors also showed persistence of the high frequency of aberrations as late as 11 years after cessation of chemo- and/or radiotherapy, although the diagnosis of these patients with persistent aberrations was not mentioned. This apparent difference in results between our study and the study done by Miller ef al. may be due to the difference in the methods used (SCE versus breakage). The study of Miller ef al. included solid-tumor patients in more than 2908 50% of the subjects, and this difference in the patient popula tion studied also may account for the discrepancy in the results. None of the patients in our study relapsed nor developed any cancer thus far. The question of whether patients with an increased SCE incidence, if found, may be at an increased risk of developing cancer could be answered by only a large-scale prospective study of a long duration. REFERENCES 1. Carrano, A. V., Thompson, L. H., Lindi, P. A., and Minkler, J. L. Sister chromatid exchange as an indicator of mutagenesis. Nature (Lond.), 277. 551-553. 1978. 2. Chaganti. R. S. K.. Schonberg, S., and German, J. A manyfold increase in sister chromatid exchanges in Bloom s syndrome lymphocytes. Proc. Nati. Acad. Sei. U. S. A., 77. 4508-4512, 1974. 3. Coleman, C. N., Williams, C. J., Flint, A., Glatstein, E. J., Rosenberg, S. A., and Kaplan. H. S. Hématologie neoplasia in patients treated for Hodgkin's disease. N. Engl. J. Med., 297. 1249-1252, 1977. 4. Fialkow, P. J., Thomas, E. D., Bryant, J. I., and Neiman, P. E. Leukemic transformation of engrafted human marrow cells in vivo. Lancet, 7: 251255, 1971. 5. Galloway. S. M., and Evans, H. J. Sister chromatid exchanges in human chromosomes from normal individuals and patients with ataxia telengiectasia. Cytogenet. Cell Genet.. 75. 17-29, 1975. 6. Inoue, S.. Ravindranath, Y.. Lusher, J. M., and Ito. T. Hematological param eters and marrow in vitro colony forming cells in acute lymphoblastic leukemia after cessation of treatment. Acta Haematol. Jpn., 43: 61-70. 1980. 7. Kato, H., and Stick, H. F. Sister chromatid exchanges in aging and repairdeficient human fibroblasts. Nature (Lond.). 260. 447-448. 1976. 8. Lambert, L., Ringborg, U., Harper, E., and Lindblad, A. Sister chromatid exchanges in lymphocyte cultures of patients receiving chemotherapy for malignant disorders. Cancer Treat. Rep., 62. 1413-1419, 1978. 9. Latt. S. A., Stetten. G., Juergens, L. A.. Buchanan, G. R., and Gerald, P. S. Induction by alkylating agents of sister chromatid exchanges and chromatid breaks in Fanconi's anemia. Proc. Nati. Acad. Sei. U. S. A. 72. 4066-4070, 1975. 10. Miller, R. C., Hill, R. B., Nichols, W. W., and Meadows, A. T. Acute and longterm cytogenetic effects of childhood cancer chemotherapy and radiother apy. Cancer Res.. 38. 3241-3246. 1978. 11. Moorehead, P. S., and Nowell, P. A. Chromosome cytology. Methods Med. Res., 70. 310-322. 1964. 12. Mosijczuk, A. D., and Ruymann, F. B. Second malignancy in acute lymphocytic leukemia. Am. J. Dis. Child., 735. 313-316, 1981. 13. Newburger, P. E., Latt. S. A., Pesando. T. M., Gustashaw. K., Powers, M., Chaganti, R. S. K., and O'Reilly. J. J. Leukemia relapse in donor cells after 14. 15. 16. 17. 18. 19. 20. allogeneic bone marrow transplantation. N. Engl. J. Med., 304: 712-714, 1981. Otter, M., Palmer, C. G., and Baehner, R. L. Sister chromatid exchanges in lymphocytes from patients with acute lymphoblastic leukemia. Hum. Genet., 52. 185-192, 1979. Perry, P., and Evans. H. J. Cytological detection of mutagen-carcinogen exposure by sister chromatid exchange. Nature (Lond.), 257. 121-125, 1975. Pinkel, D. Treatment of acute leukemia. Pediatr. Clin. North Am., 23. 117130, 1976. Raposa, T. Sister chromatid exchange studies for monitoring DNA damage and repair capacity after cytostatics in vitro and in lymphocytes of leukemic patients under cytostatic chemotherapy. Mutât. Res., 57. 241-251, 1978. Reimer, R. R.. Hoover, R., Fraumeni, J. F., and Young, R. C. Acute leukemia after alkylating therapy of ovarian cancer. N. Engl. J. Med., 297. 177-181, 1977. Thomas, E. D., Bryant, J. I., Buckner, C. D., Clift, R. A., Fefer, A., Johnson, F. L., Neiman, P., Ramberg. R. E.. and Storb, R. Leukemic transformation of engrafted human marrow cells in vivo. Lancet, 7. 1310-1313, 1972. Wolff. S. Sister chromatid exchange. Annu. Rev. Genet., 77. 183-201. 1977. CANCER RESEARCH VOL. 42 Downloaded from cancerres.aacrjournals.org on August 3, 2017. © 1982 American Association for Cancer Research. Normal Sister Chromatid Exchange Frequency in Long-Term Survivors with Acute Leukemia Susumu Inoue, Laura Brown, Yaddanapudi Ravindranath, et al. Cancer Res 1982;42:2906-2908. Updated version E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://cancerres.aacrjournals.org/content/42/7/2906 Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from cancerres.aacrjournals.org on August 3, 2017. © 1982 American Association for Cancer Research.