Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
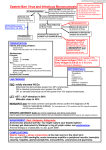
The Journal of Immunology Increased Frequency of EBV-Specific Effector Memory CD8ⴙ T Cells Correlates with Higher Viral Load in Rheumatoid Arthritis1 Jan D. Lünemann,2* Oliver Frey,2† Thorsten Eidner,‡ Michael Baier,§ Susanne Roberts,* Junji Sashihara,¶ Rudolf Volkmer,储 Jeffrey I. Cohen,¶ Gert Hein,‡ Thomas Kamradt,3† and Christian Münz3,4* EBV is a candidate trigger of rheumatoid arthritis (RA). We determined both EBV-specific T cell and B cell responses and cell-associated EBV DNA copies in patients with RA and demographically matched healthy virus carriers. Patients with RA showed increased and broadened IgG responses to lytic and latent EBV-encoded Ags and 7-fold higher levels of EBV copy numbers in circulating blood cells. Additionally, patients with RA exhibited substantial expansions of CD8ⴙ T cells specific for pooled EBV Ags expressed during both B cell transformation and productive viral replication and the frequency of CD8ⴙ T cells specific for these Ags correlated with cellular EBV copy numbers. In contrast, CD4ⴙ T cell responses to EBV and T cell responses to human CMV Ags were unchanged, altogether arguing against a defective control of latent EBV infection in RA. Our data show that the regulation of EBV infection is perturbed in RA and suggest that increased EBV-specific effector T cell and Ab responses are driven by an elevated EBV load in RA. The Journal of Immunology, 2008, 181: 991–1000. R heumatoid arthritis (RA)5 is a chronic inflammatory disease with an unknown etiology. Data from clinical trials as well as from animal models demonstrate a role for both T and B lymphocytes in RA pathogenesis (1, 2) and certain HLA-DR class II alleles; for example, HLA-DRB1*01 and HLA- *Laboratory of Viral Immunobiology, Christopher H. Browne Center for Immunology and Immune Diseases, Rockefeller University, New York, NY 10021; †Institut für Immunologie, ‡Klinik für Innere Medizin III, and §Institut für Medizinische Mikrobiologie, Universitätsklinikum Jena, Jena, Germany; ¶Medical Virology Section, Laboratory of Clinical Infectious Diseases, National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, MD 20892; and 储Institut für Medizinische Immunologie, Charitè Universitätsmedizin Berlin, Berlin, Germany Received for publication February 20, 2008. Accepted for publication May 13, 2008. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 J.D.L. is a recipient of the Dana Foundation and Irvington Institute’s Human Immunology Fellowship from the Cancer Research Institute and is supported by a Pilot Grant from the National Multiple Sclerosis Society (PP1145) and an Institutional Clinical and Translational Science Pilot and Collaborative Project Grant (to the Rockefeller University Hospital). C.M. is supported by the Dana Foundation’s Neuroimmunology Program, the Arnold and Mabel Beckman Foundation, the Alexandrine and Alexander Sinsheimer Foundation, the Burroughs Wellcome Fund, the Starr Foundation, the National Cancer Institute (R01CA108609 and R01CA101741), the National Institute of Allergy and Infectious Diseases (RFP-NIH-NIAID-DAIDS-BAA06-19), the Foundation for the National Institutes of Health (Grand Challenges in Global Health), and an Institutional Clinical and Translational Science Award (to the Rockefeller University Hospital). T.K. is supported by the Deutsche Forschungsgemeinschaft (SFB 604 C5) and the Gemeinnützige Hertie-Stiftung (1.319.110/03/03). J.S. and J.I.C. are supported by the intramural research program of the National Institute of Allergy and Infectious Diseases. J.S. is partially supported by the Japan Herpes Virus Infection Forum. 2 J.D.L. and O.F. contributed equally to this work and share first authorship. 3 T.K. and C.M. contributed equally to this work and share senior authorship. 4 Address correspondence and reprint requests to Dr. Christian Münz, Christopher H. Browne Center for Immunology and Immune Diseases, Rockefeller University, Box 390, 1230 York Avenue, New York, NY 10021. E-mail address: munzc@ rockefeller.edu 5 Abbreviations used in this paper: RA, rheumatoid arthritis; EA, early Ags; EBNA, EBV nuclear Ag; Flu-HA, influenza hemagglutinin peptide; HCMV, human CMV; HD, healthy donors; SEB, Staphylococcus enterotoxin B; VCA, viral capsid Ag. www.jimmunol.org DRB1*0401 are the strongest risk-conferring genes (3). It is, however, unclear to date if pathogenic T cells in RA predominantly recognize self or pathogen-derived Ags. The fact that concordance rates for RA are only between 15 and 30% among monozygotic twins strongly argues for environmental factors, such as pathogens that trigger or perpetuate the disease (4). EBV has been suspected for more than 25 years to be involved in RA pathogenesis (5–9). EBV is a gammaherpesvirus that infects ⬎90% of the human adult population. After primary infection in childhood or adolescence, EBV persists life-long in B lymphocytes. In latently infected B cells, only some viral proteins are expressed and confer resistance to apoptosis, possibly preventing activation-induced cell death of autoreactive B cells. The frequency of EBV-infected B cells in the blood is low (0.5–50 per million) and stable over time. Periodically, activation of infected B cells by Ag receptor triggering leads to reactivation of EBV into lytic cycle for transmission of infectious virus in the saliva of healthy virus carriers. Strong T cell responses against lytic and latent EBV Ags can be detected in healthy asymptomatic carriers and are critically important for the control of latent infection. CD4⫹ Th cell responses against EBV nuclear Ag 1 (EBNA1) can be consistently detected in healthy virus carriers. EBNA1-specific T cells produce IFN-␥, and they can recognize and kill EBV-infected cells and thereby prevent the outgrowth of EBV-transformed B cells or lymphoma cells. EBV-specific CD8⫹ CTLs undergo massive clonal expansion during acute EBV infection when CD8⫹ T cells, recognizing one particular EBV peptide, can comprise ⬎40% of all CD8⫹ T cells in the blood (10). Compared with healthy EBV carriers, patients with RA show higher titers of IgG Abs specific for both latent and lytic EBVencoded Ags (11–13). Several groups reported that T cell responses to selected EBV Ags are altered in frequency (14 –16) and are functionally impaired in RA patients (5, 6, 14). Higher frequencies of EBV-infected B cells (17) and up to 10-fold increased 992 EBV IN RA Table I. Patients and healthy blood donors Number Number (female/male) Age (years ⫾ SD) Disease duration (years ⫾ SD) Disease activity (RADAI ⫾ SD) Disease activity (DAS28 ⫾ SD)a RA HD 25 19/6 58.75 ⫾ 9.138 12.9 ⫾ 7.9 3.7 ⫾ 1.42 4.0 ⫾ 0.97 20 8/12 58.16 ⫾ 6.35 n/a n/a n/a a The disease activity scores using 28 joint counts (DAS28) were obtained in 20 patients with RA. viral copy number in circulating mononuclear cells (18) have also been detected in RA patients. Herein, we investigated both EBVspecific T cell and B cell responses as well as EBV regulation in 25 patients with RA and 20 demographically matched healthy virus carriers. Our data show that EBV infection is perturbed in patients with RA and support the concept that RA-associated immune dysfunctions drive enhanced EBV replication in B cells, thereby stimulating increased EBV-specific effector T cell and Ab responses. Materials and Methods Patients and healthy control individuals Twenty-five patients with RA diagnosed according to the 1987 American College of Rheumatology criteria (19) were recruited between March 2006 and April 2007 at the Department of Internal Medicine at the University of Jena. At the time of blood collection, patients’ medical records were reviewed, and current medications, pertinent laboratory data, and RA disease history were recorded by the treating physicians. Disease activity was assessed with a standardized patient questionnaire and a RA disease activity index (in all 25 patients) (20) as well as the disease activity score using 28 joint counts (in 20 of 25 patients) were calculated. All patients had normal white blood cell counts at the time of blood drawing. None of the patients received more than 20 mg prednisolone. Ten of the patients were treated with methotrexate, and six patients were under treatment with a TNF-␣blocking agent. One patient was treated with azathioprine and another with mycophenolate mofetil. In a subgroup analysis, we compared patients receiving immunosuppressive therapy (methotrexate, anti-TNF, azathioprine, mycophenolate mofetil) (n ⫽ 14/25) with those not receiving immunosuppressive or immunomodulatory therapy (n ⫽ 11/25) compared with healthy donors and noted no significant differences in any parameter tested. Age- and sex-matched healthy donors were recruited from a family physician’s private practice. We excluded patients with autoimmune or other chronic inflammatory disease, metabolic disorders, and a recent history of infection. Not all patients and controls were included in every analysis; rather, subsets of both groups were chosen as indicated in the results section and figure legends. Demographic and clinical characteristics are given in Table I. The study was approved by the local Institutional Review Board, and all subjects provided informed consent. ELISA and Western blot The detection of EBV and human CMV (HCMV)-specific IgG Abs was performed by ELISA following the manufacturer’s instructions (Dade Behring/Siemens). The ELISA plate for detection of EBV-specifc IgG was coated with a defined mixture of relevant virus Ags, which included epitopes derived from early Ags (EA), viral capsid Ag (VCA), and EBNA1. The Western blot for the distinct detection of recombinant EBVencoded Ags (EAp54, EAp138, VCAp23, VCAp18, EBNA1) was performed according the manufacturer’s instructions (Mikrogen). The ELISA plate for detection of HCMV-specifc IgG was coated with cell lysates from HCMV-infected cells. To determine anti-EBNA1 IgG isotype titers (21), the C-terminal domain of EBNA1 (aa 458 – 641) was recombinantly expressed with the expression vector pET15b (Novagen and a gift of Drs. Dan Zhang and Michael O’Donnell, New York, NY) in Escherichia coli BL21 (DE3) pLysS cells. Production was induced with 1 mM isopropyl -D-thiogalactoside (Invitrogen). The protein was purified and the identity determined by Western blot analysis with EBNA1-specific Ab (MAB8173; Chemicon International). Ninety-six-well polystyrene plates (Nalgene Nunc International) were coated with 1 g/well of rEBNA1458 – 641 protein in PBS or PBS alone overnight at 4°C. Plates were blocked with 200 l/well 5% nonfat milk powder for 30 min, followed by 30 min in PBS containing 5% BSA. Test plasma samples, diluted 1/10, 1/100, 1/200, 1/500, 1/1000, and 1/2000 in 3% BSA, were added for 30 min at room temperature. Plates were washed three times with TBST (10 mM Tris, 140 mM NaCl, 0.05% Tween 20). Biotin mouse anti-human IgG1, IgG2, and IgG3 Abs (BD Pharmingen) were added at 1/1000 and the anti-human IgG4 Ab was added at 1/5000 in TBST for 30 min at room temperature. After plates were washed three times in TBST, avidin-bound HRP was added for 20 min at room temperature, followed by tetramethylbenzidine substrate (R&D Systems) to develop the reaction for 10 min at room temperature and 1 M H2SO4 to stop the reaction. Plates were read in a microplate reader (Dynex Technologies). Samples were processed blinded to the clinical diagnosis. Titers were defined by the 10% effect concentration (EC10) value of individual titration curves. EBNA1 membranes Cellulose-bound peptides were prepared according to the standard SPOT synthesis protocol (22) by a MultiPep SPOT-robot (Intavis Bioanalytical Instruments) on a -alanine-modified cellulose membrane (23). Altogether, 211 12-mer peptides, overlapping by 9 aa, were covalently linked to the membrane via two -alanine residues. The membrane was activated with 96% ethanol for 10 min, washed three times with TBS for 10 min, and blocked with blocking buffer (Sigma-Aldrich) for 3 h at 4°C. After an additional washing step, the membrane was incubated with serum samples diluted 1/1000. Bound Abs were detected using a rabbit anti-human IgGalkaline phosphatase Ab (DakoCytomation) in a 1/1000 dilution. As a color substrate, 5-bromo-4-chloro-3-indolyl phosphate/NBT (Sigma-Aldrich) was used. The intensity of the spots was semiquantitatively evaluated on a 0 –3 point scale by an investigator blinded to the origin of the sample. Peptide preparation Peptides were synthesized by the Proteomics Resource Center, Rockefeller University. All peptides were created using a Protein Technologies Symphony multiple-peptide synthesizer (Rainin Instrument) on Wang resin ( p-Alkoxy-benzyl alcohol resin; Bachem and Midwest Bio-Tech) using N-Fmoc (9-fluorenylmethyloxycarbonyl) nitrogen terminal-protected amino acids (AnaSpec). Couplings were conducted using HBTU (2-(1Hbenzotriazole-1-yl)-1,1,3,3-tetramethyluronium hexafluorophosphate) and HOBT (1-hydroxybenzotriazole) in NMP (N-methylpyrrolidinone) as the primary solvent. Simultaneous resin cleavage and side-chain deprotection were achieved by treatment with concentrated, sequencing-grade trifluoroacetic acid with triisopropylsilane, water, and also ethanedithiol (if indicated by Cys or Met in sequence) added as ion scavengers in a ratio of 95:2:2:1 (all chemical reagents were purchased from Fisher Scientific, Fluka, and AnaSpec). Peptides were then released in 8 M acetic acid, filtered from resin, rotary evaporated, and redissolved in HPLC-grade water for lyophilization. All crude lyophilized products were subsequently analyzed by reverse-phase HPLC (Waters Chromatography) using a Merck Chromolith Performance C18 column. Individual peptide integrity was determined and verified by MALDI mass spectrometry using a PerkinElmer/Applied Biosystems Voyager spectrometer system. Overlapping peptides of 12- to 22-aa length (average of 15-aa length) with 11-aa overlap were designed for the EBNA1400 – 641 sequence of the B95-8 EBV strain using the peptide-generator tool of the HIV sequence database at the Los Alamos National Laboratory (PeptGen: HIV Molecular Immunology Database; http://www.hiv. lanl.gov/content/sequence/PEPTGEN/peptgen.html (accessed October 29, 2003)). Ten peptides (11 for pool no. 5) were combined in each of five different pools (see Table III). For CD8⫹ T cell epitopes from EBV and HCMV, we synthesized nonamer peptides that are part of the CEF control peptide pool of the National Institutes of Health AIDS Research and Reference Reagent Program (24) (Table II). Where indicated, influenza HA306 –318 (PKYVKQNTLKLAT) served as a control peptide. Intracellular cytokine staining assay Heparinized whole blood (0.5 ml) was stimulated with peptide mixtures for 6 h in the presence of 1 g/ml of costimulatory mAbs to CD28 (L293) and CD49d (L25) (BD Biosciences) and brefeldin A at a concentration of 10 g/ml (Sigma-Aldrich). EBNA1 peptide pools were added at a final concentration of 3.5 M per peptide per reaction. Immunodominant T cell epitopes from EBV and HCMV proteins were added at a final concentration of 1 M per peptide. Negative controls included costimulatory Abs and brefeldin A at the same concentration without peptides. Staphylococcus enterotoxin B (SEB; 1.5 g/ml) stimulation served as a positive control. After 6 h of incubation at 37°C in 5% CO2, each sample received 4 l of 0.5 M EDTA and 4.5 ml FACS lysing buffer (BD Immunocytometry Systems) before storage at ⫺80°C overnight. After thawing, cells were resuspended in 0.5 ml of permeabilization solution (0.25% BSA, 0.02% The Journal of Immunology 993 Table II. HLA class I-restricted EBV- and HCMV-encoded Ags Ag Sequence Restriction Virus EBNA3A (158 –166) EBNA3A (325–333) EBNA3A (379 –387) EBNA3A (458 – 466) EBNA3A (603– 611) EBNA3B (416 – 424) EBNA3C (258 –266) EBNA3C (281–290) BZLF1 (190 –197) BRLF1 (28 –37) BRLF1 (134 –143) BRLF1 (148 –156) BMLF1 (259 –267) HCMV pp65 (417– 426) HCMV pp65 (495–503) HCMV pp65 (512–521) QAKWRLQTL FLRGRAYGL RPPIFIRRL YPLHEQHGM RLRAEAQVK IVTDFSVIK RRIYDLIEL EENLLDFVRF RAKFKQLL DYCNVLNKEF ATIGTAMYK RVRAYTYSK GLCTLVAML TPRVTGGGAM NLVPMVATV EFFWDANDIY HLA-B8 HLA-B8 HLA-B7 HLA-B35 HLA-A3 HLA-A11 HLA-B27 HLA-B44 HLA-B8 HLA-A24 HLA-A11 HLA-A3 HLA-A2 HLA-B7 HLA-A2 HLA-B44 EBV EBV EBV EBV EBV EBV EBV EBV EBV EBV EBV EBV EBV HCMV HCMV HCMV Proliferation assay by CFSE dilution PBMCs were isolated from blood samples via density centrifugation. PBMCs were washed in PBS and incubated at 37°C in 1.25 M CFSE (Molecular Probes) in PBS at a concentration of 107 cells per ml for 10 min. Cells were washed in PBS and resuspended in RPMI 1640 with 5% PHS at a concentration of 1 ⫻ 106 cells per ml. PBMCs were distributed in 1 ml at 1 ⫻ 106 cells per well into 48-well plates. Cells were stimulated with the respective pools of peptides with a final concentration of 3.5 mol per EBNA1 peptide and 1 mol of the other EBV-encoded and HCMV pp65-derived Ags. SEB was used as a positive control at a final concentration of 1.5 g/ml. At the conclusion of a 6-day incubation at 37°C and 5% CO2, cells were harvested and washed once in PBS and stained with the indicated combinations of directly fluorochrome-labeled Abs against CD3, CD8, CD62L (SK11), CD27 (CLB-27/1), CD28, and CD45RO (all from Invitrogen or BD Pharmingen) for 30 min at 4°C. The cells were washed once with PBS and resuspended in 200 l FACS buffer before FACS analysis. The samples were measured on a BD LSR II flow cytometer. Gating and calculations for precursor frequencies were performed with FlowJo software. The frequencies of proliferating Ag-specific T cells were determined by subtracting the background frequency from the frequency of Ag-stimulated positive samples. Luminex assay sodium azide, 0.5% saponin in PBS) and left at room temperature for 10 min. After an additional centrifugation, the permeabilization solution was decanted and cells were stained with directly fluorochrome-labeled Abs against CD3 (S4.1; Invitrogen), CD4 (S3.5; Invitrogen), CD8 (RPA-T8), IFN-␥ (25723.11), and CD45RO (UCHL-1; all from BD Pharmingen) for 15 min at room temperature. After two washes, cells were resuspended in 200 l of FACS buffer solution (0.25% BSA and 0.02% sodium azide in PBS). At least 50,000 events were collected on a BD LSR II flow cytometer (BD Biosciences) by gating on CD3⫹ lymphocytes. Frequencies of CD3⫹-gated CD4⫹ and CD8⫹ Ag-specific IFN-␥ producing T cells were calculated using FlowJo software (Tree Star). According to criteria previously used in ELISPOT analyses (25), a positive response required a frequency at least 2-fold above background (no Ag) and at least 10 IFN-␥⫹ events. The frequencies of Ag-specific T cells were determined by subtracting the background frequency from the frequency of Ag-stimulated positive samples. A Cell supernatants from growing T cell cultures were analyzed at day 6 for cytokines and using the Protein Multiplex Immunoassay kit (Biosource International) as per the manufacturer’s protocol. In brief, Multiplex beads were vortexed and sonicated for 30 s, and 25 l was added to each well and washed twice with wash buffer. The samples were diluted 1/2 with assay diluent and loaded onto a Multiscreen BV 96-well filter plate (Millipore) with 50 l of incubation buffer already added to each well. Serial dilutions of cytokine standards were prepared in parallel and added to the plate. Samples were then incubated on a plate shaker at 600 rpm in the dark at room temperature for 2 h. The plate was applied to a MultiScreen Vacuum Manifold (Millipore) and washed twice with 200 l of wash buffer. Biotinylated anti-human MultiCytokine Reporter (100 l; Biosource International) was added to each well. The plate was incubated on a plate shaker at 600 rpm in the dark at room temperature for 1 h. The plate was applied to a MultiScreen Vacuum Manifold and washed twice with 200 l of wash buffer. Streptavidin-PE was diluted 1/10 in wash buffer, and 100 l was EBV IgG Titer 1600 CMV 40000 1200 30000 800 20000 400 10000 0 0 HD B HD RA RA EBNA1 VCAp18 VCAp23 EAp138 EAp54 RA, seropositive (%) 84 100 100 24 32 HD, seropositive (%) 82 100 100 0 0 p-value n.s. n.s. n.s. 0.03 0.006 FIGURE 1. Increased EBV-specific IgG titer and frequent IgG recognition of EBV-encoded early Ags in RA. A, RA patients show increased IgG responses to EBV- (Mann-Whitney U test: p ⫽ 0.03) but not to HCMV-encoded Ags. Displayed are titers of Abs specific for EBV-encoded EA, VCA, and EBNA1 and specific for HCMV-infected cell lysates. B, EBV IgG-containing sera were subsequently tested for their Ag specificity by immunoblotting. While VCA- and EBNA1-specific Abs were present in the majority of both RA patients and healthy virus carriers, EBV-EA targeting IgG were exclusively detectable in RA sera (Fisher’s exact test: p ⫽ 0.03 for EAp138; p ⫽ 0.006 for EAp54). 994 added directly to each well. The plate was incubated on a plate shaker at 600 rpm in the dark at room temperature for 30 min. The plate was then applied to the vacuum manifold, washed twice, and each well was resuspended in 100 l wash buffer and shaken for 1 min. The assay plate was then transferred to the Bio-Plex Luminex 100 XYP instrument (Millipore) for analysis. Cytokine concentrations were calculated using Bio-Plex Manager 3.0 software with a five-parameter curve-fitting algorithm applied for standard curve calculations. EBV IN RA Table III. EBNA1 peptides Peptide Pool No. 1 Viral loads EBV DNA was quantified from PBMCs by quantitative real-time PCR using a TaqMan PCR kit and an Applied Biosystems model 7500 sequence detector (26). DNA was extracted from PBMCs using the QIAamp DNA blood mini kit (Qiagen) following the manufacturer’s protocol. A region from the BamHI W fragment of EBV was amplified using primers 5⬘GGACCACTGCCCCTGGTAAA-3⬘ and 5⬘-TTTGTGTGGACTCCTG GGG-3⬘ and detected with fluorogenic probe 5⬘-FAM-TCCTGCAGCTA TTTCTGGTCGCATCA-TAMRA-3⬘. The human bcl-2 gene was amplified using primers 5⬘-CCTGCCCTCCTTCCGC-3⬘ and 5⬘-TGCAT TTCAGGAAGACCCTGA-3⬘ and detected with fluorogenic probe 5⬘-FAMCTTTCTCATGGCTGTCC-TAMRA-3⬘. The EBV BamHI W fragment copy number per cell was calculated using the formula n ⫽ 2 ⫻ W/B, where n is the EBV BamHI W copy number/cell, W is the EBV BamHI W copy number, and B is the bcl-2 copy number. All samples were tested in at least duplicate, and the mean results were determined. 2 3 Statistical analysis Statistics were performed using commercial software (Prism 4, GraphPad Software). Comparisons between RA patients and healthy donors were based on the nonparametric Mann-Whitney U test. Categorical differences between the two cohorts were analyzed by Fisher’s exact test. For correlation analyses between clinical disease parameters and T cell responses, we used the nonparametric Spearman correlation. Results 4 Increased EBV-specific IgG titer and frequent IgG recognition of EBV-encoded early Ags in RA First, we evaluated IgG Ab responses to EBV- and HCMV-encoded Ags in 25 patients with RA compared with 20 demographically matched healthy donors (HD). The ELISA plate for detection of EBV-specific IgG was coated with a mixture of epitopes derived from EA, VCA, and EBNA1. The ELISA plates for the detection of HCMV-specific IgG were coated with lysates from HCMV-infected cells and noninfected control lysates. Differences in Ab reactivities against infected compared with noninfected cell lysates are reported. As shown in Fig. 1, both patients with RA and HD were universally infected with EBV. HCMV responses could be detected in 73% of HD and 69% of RA patients, respectively. EBV-specific, but not HCMV-specific, IgG titers were significantly higher in the RA cohort ( p ⫽ 0.03) (Fig. 1A). Next, we tested the Ag specificity of EBV targeting IgG by immunoblotting. Healthy donors as well as RA patients were both universally seropositive for EBNA1 and viral capsid-specific IgG. In contrast, IgG responses to EBV-EA were only observed in RA patients but not in healthy donors (Fig. 1B). These data show that patients with RA exhibit elevated IgG responses toward EBV and a broader recognition of EBV-encoded Ags compared with healthy EBV carriers, whereas immune responses against HCMV were similar in both groups. Expansion of EBV-specific CD8⫹ immediate effector T cells in RA Employing an ex vivo flow cytometry-based intracellular IFN-␥ staining assay, we determined EBV- and HCMV-specific CD4⫹ and CD8⫹ T cell responses in 25 patients and 20 healthy virus carriers. For restimulation of PBMCs, either a mixture of MHC class I-restricted T cell epitopes derived from three latent (EBNA3A, EBNA3B, EBNA3C) and three lytic (BZLF1, BRLF1, and BMLF1) Ags (Table II) or a peptide library of the C-terminal 5 Description EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 EBNA1 (400 – 414) (405– 418) (409 – 422) (413– 429) (420 – 434) (425– 439) (430 – 451) (435– 451) (442– 458) (449 – 461) (452– 465) (456 – 469) (460 – 474) (465– 478) (469 – 482) (473– 487) (478 – 491) (482– 496) (487–503) (494 –508) (499 –510) (501–514) (505–518) (509 –522) (513–527) (519 –532) (523–536) (527–541) (532–544) (535–548) (539 –554) (545–559) (549 –563) (554 –566) (557–571) (562–576) (566 –580) (571–584) (575–588) (579 –593) (584 –597) (588 – 600) (591– 604) (595– 609) (600 – 614) (605– 619) (610 – 625) (616 – 629) (620 – 634) (625– 639) (630 – 641) Sequence PGRRPFFHPVGEADY FFHPVGEADYFEYH VGEADYFEYHQEGG DYFEYHQEGGPDGEPDV EGGPDGEPDVPPGAI GEPDVPPGAIEQGPA PPGAIEQGPADDPGEGPSTGPR EQGPADDPGEGPSTGPR PGEGPSTGPRGQGDGGR GPRGQGDGGRRKK GQGDGGRRKKGGWF GGRRKKGGWFGKHR KKGGWFGKHRGQGGS FGKHRGQGGSNPKF RGQGGSNPKFENIA GSNPKFENIAEGLRA FENIAEGLRALLAR AEGLRALLARSHVER ALLARSHVERTTDEGTW VERTTDEGTWVAGVF DEGTWVAGVFVY GTWVAGVFVYGGSK AGVFVYGGSKTSLY VYGGSKTSLYNLRR SKTSLYNLRRGTALA NLRRGTALAIPQCR GTALAIPQCRLTPL AIPQCRLTPLSRLPF RLTPLSRLPFGMA PLSRLPFGMAPGPG LPFGMAPGPGPQPGPL PGPGPQPGPLRESIV PQPGPLRESIVCYFM LRESIVCYFMVFL SIVCYFMVFLQTHIF FMVFLQTHIFAEVLK LQTHIFAEVLKDAIK FAEVLKDAIKDLVM LKDAIKDLVMTKPA IKDLVMTKPAPTCNI MTKPAPTCNIRVTV APTCNIRVTVCSF CNIRVTVCSFDDGV VTVCSFDDGVDLPPW FDDGVDLPPWFPPMV DLPPWFPPMVEGAAA FPPMVVEGAAAEGDDG EGAAAEGDDGDDGDE EGDDGDDGDEGGDGD DDGDEGGDGDEGEEG GGDGDEGEEGQE domain of EBNA1 (aa 400 – 641) was chosen. The MHC class I-restricted T cell epitopes were selected based on their previous identification as immunodominant CD8⫹ T cell epitopes (27), whereas EBNA1 was chosen as a dominant EBV-encoded CD4⫹ T cell Ag in healthy virus carriers (Table III) (27–29). MHC class I-restricted HCMV pp65-derived peptides were used as control Ags (Table II) (24, 26, 30). The mixture of MHC class I-restricted T cell epitopes constitutes the EBV- and HCMV-derived portion of the control peptide pool, which is used as positive controls in immunomonitoring studies of patients infected with HIV and contains CD8⫹ T cell epitopes recognized by most individuals (24). PMBCs were analyzed for intracellular cytokine production after 6 h of stimulation with peptide Ags or SEB as positive control. As shown in Fig. 2, RA patients demonstrated substantial expansions of CD8⫹ T cells specific for both EBV-encoded immunodominant The Journal of Immunology 995 A w/o 105 0.19 SEB 105 0.088 HCMVpp65 105 1.34 0.23 EBV 105 0.2 EBNA1pool1-5 0.091 105 0.23 104 104 104 104 104 103 103 103 103 103 102 102 102 102 0 0 0 102 103 104 105 105 0.18 0 0 102 103 104 105 105 0.36 0.21 104 105 0.18 105 0.3 103 104 105 0 102 0.19 105 0.32 104 104 104 104 103 103 103 103 103 102 102 102 102 0 0 102 103 104 105 0 0 102 103 104 105 103 104 105 104 105 0.23 0.25 102 0 0 0 102 103 EBNA1pool5 104 0 0.27 0 0 102 EBNA1pool4 EBNA1pool3 105 0.21 103 0.15 102 0 0 102 EBNA1pool2 EBNA1pool1 IFN-γ 1.3 0 102 103 104 105 0 102 103 104 105 CD8 B EBNA1 EBV CD4+ T cells IFN-γ producing T cells CD8+ T cells * 0.6 0.2 FLU-HA HCMVpp65 CD8+ T cells * 0.8 CD8+ T cells 3 SEB 0.2 CD4+ T cells CD8+ T cells CD4+ T cells 8 25 0.5 20 0.6 0.4 0.1 0.3 6 2 0.1 15 0.4 4 1 10 0.2 0.2 0.0 0.0 0.1 2 5 0 0.0 0.0 HD RA HD RA 0 0 HD RA HD RA HD RA HD RA HD RA FIGURE 2. Increased Frequency of EBV-specific CD8⫹ immediate effector T cells in RA. A, Ex vivo flow cytometry-based intracellular IFN-␥ staining assay to determine the frequency of EBV- and HCMV-specific T cells in RA and HD. Depicted is the analysis of CD3⫹ T cells from a representative RA patient with a strong CD8⫹ T cell response to EBV-encoded Ags. MHC class I-restricted HCMV pp65-derived peptides were used as control Ags (Table II). MHC class I-restricted T cell epitopes derived from three latent (EBNA3A, EBNA3B, EBNA3C) and three lytic (BZLF1, BRLF1, BMLF1) Ags (designated as EBV) were selected based on their previous identification as immunodominant CD8⫹ T cell epitopes (Table II). The C-terminal domain of EBNA1 (aa 400 – 641), toward which most healthy virus carriers develop a CD4⫹ T cell response, was chosen as a dominant EBV-encoded CD4⫹ T cell Ag, and a total of 51 overlapping peptides were distributed into five different pools (Table III). PMBCs were analyzed for intracellular cytokine production after 6 h of stimulation with peptide Ags or SEB as positive control. B, Patients with RA showed substantial expansions of CD8⫹ T cells specific for both EBV-encoded immunodominant MHC class I-restricted Ags (mean frequency in HD vs RA: 0.11% vs 0.28% of all circulating CD8⫹ T cells; p ⫽ 0.0029) and EBNA1 (mean frequency in HD vs RA: 0.03% vs 0.23% of all circulating CD8⫹ T cells; p ⫽ 0.03), indicating that IFN-␥-producing, EBV Ag-specific, effector CD8⫹ T cells are expanded in RA. The frequency of EBNA1-specific CD4⫹ T cells among all CD4⫹ lymphocytes (mean frequency in HD vs RA: 0.03% vs 0.05%) and HCMV pp65-specific CD8⫹ T cells among all CD8⫹ lymphocytes (mean frequency in HD vs RA: 0.72% vs 0.54%) did not significantly differ between patients and controls. Additionally, frequencies of CD4⫹ T cells specific for Flu-HA, chosen for its reported promiscuous MHC class II binding and its immunodominance in humans, did not differ between 14 healthy donors and 15 RA patients who were tested for Flu-HA recognition (mean frequency in HD vs RA: 0.04% vs 0.06%). Following SEB stimulation, patients and controls showed similar frequencies of IFN-␥-producing CD8⫹ T cells (mean frequency in HD vs RA: 7.1% vs 5.2%) and CD4⫹ T cells (mean frequency in HD vs RA: 1.9% vs 2.7%). MHC class I-restricted Ags (mean frequency in HD vs RA: 0.11% vs 0.28% of all circulating CD8⫹ T cells; p ⫽ 0.0029) and EBNA1 (mean frequency in HD vs RA: 0.03% vs 0.23% of all circulating CD8⫹ T cells; p ⫽ 0.03), indicating that IFN-␥-producing, EBV Ag-specific, effector CD8⫹ T cells are expanded in RA. Notably, the frequency of EBNA1-specific CD8⫹ T cells was at the detection limit of the ex vivo cytokine staining assay in healthy virus carriers (26, 30 –33), whereas these cells were clearly detectable in patients with RA. The frequency of EBNA1-specific CD4⫹ T cells among all CD4⫹ lymphocytes (mean frequency in HD vs RA: 0.03% vs 0.05%) and HCMV pp65-specific CD8⫹ T cells among all CD8⫹ lymphocytes (mean frequency in HD vs RA: 0.72% vs 0.54%) did not significantly differ between patients and controls. Additionally, frequencies of CD4⫹ T cells specific for an influenza hemagglutinin peptide (Flu-HA, aa 306 –318), chosen for its reported promiscuous MHC class II binding and its immunodominance in humans (34), did not differ between 14 healthy donors and 15 RA patients, who were tested for Flu-HA recognition (mean frequency in HD vs RA: 0.04% vs 0.06%). Following SEB stimulation, patients and controls showed similar frequencies of IFN-␥-producing CD8⫹ T cells (mean frequency in HD vs RA: 7.1% vs 5.2%) and CD4⫹ T cells (mean frequency in HD vs RA: 1.9% vs 2.7%). These findings appeared to be independent of the patients’ treatment status, since both untreated (n ⫽ 11/25) and treated (n ⫽ 14/25) patients as well as patients receiving anti-TNF therapy (n ⫽ 6) showed significantly higher frequencies of EBV Ag-specific CD8⫹ T cells compared with healthy controls. In contrast, frequencies of CD4⫹ T cells specific for EBNA1, CD8⫹ T cell responses to HCMV pp65, and CD4⫹ as well as CD8⫹ T cell responses to SEB were similar between untreated and treated patients vs controls (data not shown). Collectively, these data indicate that the frequency of circulating CD8⫹ T cells, targeting both lytic and latent EBV-encoded Ags, is specifically increased in patients with RA. Effector and central memory compartmentalization of EBV-specific CD8⫹ T cells in RA To identify which CD8⫹ T cell subsets contribute to the increased response in RA, we determined proliferative responses to the respective viral Ags in 25 RA patients and 20 healthy controls using a 996 EBV IN RA FIGURE 3. Increased proliferative capacity of lytic and latent EBV Ag-specific CD8⫹ T cells in RA. Employing a flow cytometry-based CFSE dilution assay, we detected that patients with RA showed substantially higher proliferative responses to EBVencoded immunodominant CD8⫹ T cell epitopes, but not to HCMV pp65 (p ⫽ 0.004). EBNA1-specifc CD8⫹ T cell proliferation tended also to be higher in RA, but it was only detectable in six patients and three healthy virus carriers and did not reach statistical significance. EBNA1-specific CD4⫹ T cell proliferation was similar in RA patients and in healthy virus carriers. multiparameter flow cytometry-based CFSE dilution assay. In line with our finding on ex vivo IFN-␥ production, patients with RA showed substantially higher proliferative responses to EBV-encoded immunodominant CD8⫹ T cell epitopes ( p ⫽ 0.004), but not to HCMV pp65 (Fig. 3). EBNA1-specific CD8⫹ T cell proliferation tended also to be higher in RA, but it was only detectable in six A SEB CD8 No Antigen patients and three healthy virus carriers, thus not reaching statistical significance. We further characterized the phenotype of CFSE-diluted EBVspecific CD8⫹ T cells using markers indicative for central and effector memory compartments (CD45RO, CD62L) as well as for the costimulatory molecules CD28 and CD27 (30). As expected, HCMVpp65 EBV EBNA1 0.91 17.7 0.71 2.49 0.65 0.55 21.6 0.36 1.58 0.74 CFSE 11.1 8.05 2.4 CD28 0.086 CD27 11.3 CD62L 0.84 CD45RO CD8+ T cells: 6.94 3.94 CFSE B SEB CD8 No Antigen HCMVpp65 EBV EBNA1 0.75 32.6 1.25 0.87 1.67 0.6 14.2 0.61 0.33 0.7 CFSE 3.66 3.48 0.95 3.98 CD28 1.85 CD27 1 2.89 CD62L CD45RO CD8+ T cells: 0.41 CFSE ⫹ FIGURE 4. Expanded EBV-specific CD8 T cells in RA predominantly originate from the CD45RO⫹CD62L⫺ effector memory T cell pool. The phenotype of CFSElow EBV-specific CD8⫹ T cells was determined using markers indicative for central and effector memory compartments (CD45RO, CD62L) as well as for differentiation and costimulation (CD27, CD28). A, Nearly all EBV-specific T cells originated from the memory pool (CD45RO⫹). Most expanded CD8⫹ T cells specific for immunodominant MHC class I-restricted epitopes lacked CD62L expression identifying them as effector memory T cells. B, Proliferating CD8⫹ T cells specific for EBNA1 consisted of both CD62L⫹ and CD62L⫺ memory T cells. As expected, most CD8⫹ T cells specific for EBV Ags were CD27⫹CD28⫹, and we did not detect any statistically significant difference in the frequency of CD27 or CD28 expression by EBV-specific CD4⫹ and CD8⫹ memory T cells between patients and healthy volunteers. The Journal of Immunology aa 1 61 121 181 241 301 361 421 481 541 601 B 3.0 Intensity of spots (AU) aa 1 61 121 181 241 301 361 421 481 541 601 RA 2.5 2.0 1.5 1.0 0.5 0.0 0 0.0 HD Intensity of spots (AU) A 997 50 100 150 200 0.5 1.0 1.5 2.0 2.5 3.0 C msdegpgtgpgnglgekgdtsgpegsggsgpqrrggdnhgrgrgrgrgrgggrpgapggs gsgprhrdgvrrpqkrpscigckgthggtgagagaggagaggagagggagagggaggagg aggagagggagagggaggaggagagggagagggaggagagggaggaggagagggagaggg aggagagggaggaggagagggagaggaggaggagaggagagggaggaggagaggagagga gaggagaggaggagaggaggagaggaggagagggaggagaggaggagaggaggagagga ggagaggaggagagggagaggagaggggrgrggsggrgrggsggrgrggsggrrgrgrer arggsrerargrgrgrgekrprspssqssssgspprrpppgrrpffhpvgeadyfeyhqe ggpdgepdvppgaieqgpaddpgegpstgprgqgdggrrkkggwfgkhrgqggsnpkfen iaeglrallarshverttdegtwvagvfvyggsktslynlrrgtalaipqcrltplsrlp fgmapgpgpqpgplresivcyfmvflqthifaevlkdaikdlvmtkpaptcnirvtvcsf ddgvdlppwfppmvegaaaegddgddgdeggdgdegeegqe N-terminal GA-repeat C-terminal D HD RA EBNA1-IgG1 1500 * 1000 500 0 HD RA EBNA1-IgG2 EBNA1-IgG4 1500 1500 1000 1000 500 500 0 HD RA 0 HD RA FIGURE 5. Broadened specificity and IgG1 polarization of EBNA1-specific IgG responses in RA. A, Epitopes recognized by EBNA1-specific IgG were identified using a membrane carrying spots of 211 covalently linked overlapping dodecamer peptides that cover the entire sequence of EBNA1 (aa 1– 641). Each spot contains a linear synthetic peptide of 12-aa length bound to a continuous cellulose membrane. Representative examples from one RA patient and one healthy donor (HD) are shown in A. The relative spot intensities correlate with the amount of bound serum Abs. B, Mean relative spot intensities for 12 HD (lower panel) and 12 RA (upper panel) patients. IgG Abs from healthy donors recognized predominantely the glycine/alanine-rich repeat (GA) domain of EBNA1 (aa 88 –323). In contrast, IgG Abs form RA patients recognized a much broader array of epitopes, including epitopes in the arginineenriched flanking regions of the GA-domain and in the C-terminal domain of EBNA1. The differentially recognized spots are outlined in black in B, and the corresponding primary protein sequence of EBNA1 is underlined in C. D, RA patients showed selectively increased titers of EBNA1 (aa 458 – 641)specific IgG1 (p ⫽ 0.02) but not IgG2 or IgG4. EBNA1-specific IgG3 Abs could not be detected in HD or RA patients (data not shown). nearly all EBV-specific CD8⫹ T cells originated from the CD45RO⫹ memory compartment. The CD8⫹ T cells specific for EBNA1 consisted of CD62L⫹ and CD62L⫺ memory T cells (Fig. 4B) and thus did not differ in this respect from EBNA1-specific CD4⫹ T cells, in which both CD62L⫹ central memory and CD62L⫺ effector memory T cell subsets contributed approximately equally to EBNA1-specific CD4⫹ T cell proliferation in patients (data not shown) and healthy controls (30). The phenotypes described above were consistently found in all donors showing CD4⫹ and/or CD8⫹ T cell proliferative responses to EBV-encoded Ags, with no statistically significant difference found between RA patients and healthy virus carriers. Latent EBV Ag-specific CD4⫹ and CD8⫹ memory T cells accumulate within a CD27⫹CD28⫹ differentiation compartment during primary infection and remain enriched within this compartment throughout the persistent phase of infection (35, 36). CD8⫹ T cells specific for lytic cycle Ags accumulate within both CD27⫹CD28⫹ and CD27⫹CD28⫺ compartments, indicating a difference in differentiation states and/or costimulatory require- ments (37). Stimulation with immunodominant CD8⫹ T cell epitopes resulted in expansion of a minor CD27⫹CD28⫺ population, which also lacked CD62L expression, indicating further differentiated effector memory T cells (38) (Fig. 4A). Most proliferating EBNA1-specific CD8⫹ T cells in our cohort of RA patients and healthy donors originated from the CD27⫹CD28⫹ compartment (Fig. 4B). We did not detect any statistically significant difference in the frequency of CD27 or CD28 expression by EBVspecific CD4⫹ and CD8⫹ T cells between patients and healthy volunteers (data not shown). These data do not support the concept of insufficient T cell responses to EBV in RA. The preferential expansion and increased frequency of effector memory and IFN-␥ producing CD8⫹ T cells specific for EBV proteins expressed during viral replication, however, suggests an increased availability of these Ags due to higher viral replication in patients with RA. Cytokine profiling of EBV-specific T cell immunity in RA To determine whether patients with RA show qualitatively altered EBV-specific T cell cytokine profiles compared with healthy virus 998 1.0 Frequency of CD8+ T cells specific for pooled viral antigens Viral load 15000 (EBV copy number per 106 PBMC) FIGURE 6. Increased EBV loads correlate with higher frequencies of EBV-specific CD8⫹ T cells in RA. A, EBV viral loads are 7.3-fold higher in RA patients compared with healthy virus carriers (p ⫽ 0.02; unpaired t test with Welch’s correction). EBV DNA was quantified from PBMC by quantitative real-time PCR in relation to bcl-2 expression. All samples were tested at least in duplicate, and the mean values are shown. Bars and error bars represent means and SEM, respectively. B, RA patients with high EBV copy numbers show higher frequencies of IFN-␥-producing EBV-specific CD8⫹ T cells specific for MHC class I-restricted, pooled lytic, and latent EBV Ags (Spearman r ⫽ 0.53; p ⫽ 0.02). EBV IN RA 10000 5000 0 HD carriers, we analyzed supernatants of EBV-specific T cell cultures obtained at day 6 after primary proliferation for the composition of cytokines indicative of Th1 (IFN-␥), Th2 (IL-13), and Th17 (IL17) polarization as well as for IL-2 and IL-10 production. Of these, only IFN-␥ and IL-2 were detectable at low levels in both RA- and HD-derived cell cultures stimulated with MHC class I-restricted EBV Ags (mean concentrations for IFN-␥: 41 pg/ml (HD) vs 323 pg/ml (RA); mean concentrations for IL-2: 58 pg/ml (HD) vs 86 pg/ml (RA) as measured in 14 representative positive T cell cultures), and production of IFN-␥ was moderately increased in RAderived positive cultures stimulated with immunodominant CD8⫹ T cell epitopes ( p ⫽ 0.03). These data are consistent with the observation that Th1 polarization and IFN-␥ production predominate in EBV-specific T cell immunity and do not argue for a qualitatively altered T cell response to EBV in patients with RA. Broadened specificity and IgG1-polarization of EBNA1-specific IgG responses in RA To further assess the relative activity of EBV-specifc Th1 cells in vivo, we recombinantly expressed the immunogenic C terminus of EBNA1 (aa 458 – 641) in an eukaryotic expression system and analyzed EBNA1-targeting IgG isotype-specific responses in 25 patients and 20 healthy EBV carriers (21). IFN-␥ can skew human Ab responses toward the IgG1 opsonizing and complement-fixing Ig subclass and IL-4 toward the allergy-related IgG4 and IgE subclasses (21). As depicted in Fig. 5D, patients with RA showed significantly increased titers of EBNA1-specific IgG1 ( p ⫽ 0.02), but not IgG2 or IgG4. EBNA1-specific IgG3 Abs could not be detected in HD or RA patients (data not shown). IgG1 was the most frequently detected isotype in all individuals tested, possibly reflecting the Th1 polarization of EBNA1-specific T cell immunity. IgG4 responses to EBNA1 were detected in a minor subgroup of patients and controls, with no statistically significant differences found between both cohorts. We next determined target epitopes of EBNA1-specific IgG in 12 patients and 12 controls by using membranes, on which 211 covalently linked and overlapping dodecamer peptides, covering the entire sequence of EBNA1 (aa 1– 641), had been spotted (22, 23). As shown in Fig. 5, the glycine/alaninerich repeat (GA) domain of EBNA1 (aa 88 –323) was predominantly recognized by IgG Abs from healthy virus carriers. In contrast, IgG Abs from RA patients recognized a much broader array of epitopes. Differentially recognized epitopes were primarily lo- RA Spearmen r = 0.53 0.8 p = 0.02 0.6 0.4 0.2 0.0 101 102 103 104 105 Viral Load cated in the arginine-enriched flanking regions of the GA domain (EBNA1 aa 33– 89 and EBNA1 aa 324 – 402) and in the C-terminal domain of EBNA1 (EBNA1 aa 421–527) (Fig. 5B). None of these epitopes was exclusively recognized by RA patients or by healthy virus carriers. Membranes incubated with control sera from EBVseronegative donors did not show any positive spots (data not shown). These data support the concept that patients with RA show increased as well as broadened EBV-specific immune responses. EBV copy numbers in circulating blood cells are 7-fold increased in RA We next quantified levels of cell-bound viral genomes in circulating blood cells in patients and controls and compared frequencies of EBV-specific T cells with viral loads. To this end, we determined EBV DNA copy numbers in PBMCs by real-time PCR using bcl-2 DNA controls to determine copy numbers per genome in 19 patients and 13 healthy EBV carriers (26). EBV DNA was detectable in 13 of 19 (68%) RA patients and in 6 of 13 (46%) healthy donors from whom PBMCs were accessible for viral load quantification. RA patients showed 7.3-fold increased levels of cell-associated EBV DNA copies (mean 1,397 for HD vs 10,146 for RA per 106 PBMC, respectively) (Fig. 6). We found that RA patients with high EBV copy numbers showed higher frequencies of IFN-␥-producing EBV-specific CD8⫹ T cells specific for MHC class I-restricted, pooled lytic, and latent EBV Ags (Spearman r ⫽ 0.53; p ⫽ 0.02) (Fig. 6, right panel). Comparisons of viral loads and CD4⫹ T cell frequencies did not show any statistically significant correlations. There was no significant correlation between clinical disease activity as assessed by the disease activity score using 28 joint counts (DAS28) and EBV copy numbers. Furthermore, proliferating T cell frequencies to EBV-encoded Ags did not correlate with EBV copy numbers in RA patients and healthy virus carriers. Discussion Our study demonstrates that RA patients have elevated CD8⫹ T cell and B cell responses to pooled lytic and latent EBV Ags that are involved in both B cell transformation and productive viral replication. We did not find evidence for a defective T cell control of EBV infection in RA. In contrast, higher levels of cell-associated viral genomes in circulating blood cells correlated with increased frequencies of EBV-specific and IFN-␥-producing CD8⫹ The Journal of Immunology T cells, suggesting that increased viral replication drives enhanced EBV-specific immune responses in RA. EBV manipulates the human B cell compartment to achieve persistence in memory B cells and is strongly regulated by and responsive to the biology of its main host cell. It is thought that EBV initially infects extrafollicular naive B cells in tonsils after transmission by saliva exchange (39). By driving B cells into activation and proliferation, upon which they home to germinal centers and then differentiate with the help of EBV Ags into memory B cells, the virus gains access to a long-lived host cell reservoir and persists in the absence of EBV protein expression with the exception of EBNA1 during homeostatic B cell division (40). Ag stimulation and/or receipt of a plasma cell differentiation signal drive occasional reactivations into the viral lytic cycle (41). It has previously been proposed that B cell dysfunction in autoimmune diseases associated with prominent autoantibody production alters regulatory mechanisms of EBV persistence, since patients with systemic lupus erythematosus show aberrant expression of viral latent and lytic genes in the blood, as well as abnormally high frequencies of circulating EBV-infected cells associated with disease flares (42). Autoantigen-specific B cells are normally neutralized or controlled by several tolerance checkpoints during B cell development (43– 46). Patients with RA exhibit defects in central B cell tolerance mechanisms, resulting in higher frequencies of circulating autoreactive B cells (47) and rheumatoid factor, which consists of autoantibodies against the constant region of IgG Abs and can be detected in ⬃80% of RA patients (48). Rheumatoid factor has shown to induce EBV replication in B cells via BCR stimulation in vitro (49), and it is therefore conceivable that higher viral loads in blood cells result from frequent B cell autoantigen recognition in RA instead of being a consequence of impaired T cell-mediated immune responses to EBV. The hypothesis that autoreactivity partly contributes to increased levels of EBV replication by triggering EBV release from autoreactive EBV-infected B cells fits well with the finding that lytic EBV Ag-specific T cell responses are increased in RA. CD4⫹ and CD8⫹ T cells against lytic EBV Ags have previously been isolated from inflamed joints of RA patients (50, 51), indicating that EBV-specific T cells are not only elevated in peripheral blood, but that they also infiltrate inflamed joints in RA. In agreement with these previous studies, we demonstrate that most EBV-specific CD8⫹ T cells belong to the effector memory compartment and lack homing markers to secondary lymphoid tissues like CD62L (38), and they therefore might preferentially home to sites of autoimmune inflammation. Organized lymphoid structures that resemble secondary lymphoid organs are frequently found in synovial tissues from RA patients (52). Analyses of the rearranged Ig V genes of B cells that were isolated from biopsies of these tertiary lymphoid structures in patients with RA have shown that B cells undergo Ag-driven clonal expansion and somatic hypermutation at these ectopic follicles (53, 54). Similar structures are found in the CNS of patients with multiple sclerosis (55), another autoimmune disease associated with altered immune responses to EBV (26), and it has recently been reported that ⬎40% of brain-infiltrating B cells and plasma cells are infected with EBV and show expression of primarily latent viral Ags spatially associated with expansions of infiltrating CD8⫹ T cells (56). Instead of latent Ags, expression of lytic EBV Ags has been described in the synovial tissue of RA patients (57) and could enhance inflammation via local restimulation of T cells directed against these Ags. Therefore, even though elevated EBV-specific immune cell responses might represent an epiphenomenon in response to increased Ag load in circulating blood cells in RA, they could nevertheless augment T cell-medi- 999 ated tissue damage and contribute to a local proinflammatory environment by recognizing EBV gene products in inflamed joints. An implication of this line of thought is that deregulated EBVspecific immune responses and increased viral titers in RA can be normalized by clinically effective therapeutic B cell depletion (58). It will therefore be of interest to longitudinally study EBV-specific T and B cell responses in RA patients during B cell-depleting rituximab treatment and to evaluate the validity of EBV-associated immune parameters as potential biomarkers for treatment responsiveness in RA (59). In conclusion, we have demonstrated perturbations of EBV infection in patients with RA. The altered immune recognition of EBV in RA is not restricted to one specific Ag but involves a mixture of both lytic and latent viral gene products expressed during viral replication. Expanded CD8⫹ T cell responses to these Ags positively correlate with increased viral loads in circulating blood cells. This suggests that RA-associated immune dysfunctions drive enhanced EBV replication in B cells and thereby stimulate EBV-specific T cell responses. Future studies will need to address whether specific B cell abnormalities in RA correlate with changes in the regulation of EBV infection observed in these patients. Our data indicate that investigating the biology of EBV infection in the context of autoimmunity has the potential to provide new insights into mechanisms of EBV regulation and the pathogenesis of autoimmune diseases. Acknowledgments We gratefully acknowledge Drs. J. Frey and H. Jödicke for their help with the recruitment of the healthy donors. We thank all of our patients for their continual cooperation. Disclosures The authors have no financial conflicts of interest. References 1. Firestein, G. S. 2003. Evolving concepts of rheumatoid arthritis. Nature 423: 356 –361. 2. Muller-Ladner, U., T. Pap, R. E. Gay, M. Neidhart, and S. Gay. 2005. Mechanisms of disease: the molecular and cellular basis of joint destruction in rheumatoid arthritis. Nat. Clin. Pract. Rheumatol. 1: 102–110. 3. Klareskog, L., L. Padyukov, J. Ronnelid, and L. Alfredsson. 2006. Genes, environment and immunity in the development of rheumatoid arthritis. Curr. Opin. Immunol. 18: 650 – 655. 4. Kamradt, T., R. Göggel, and K. Erb. 2005. Induction, exacerbation and inhibition of allergic and autoimmune diseases by infection. Trends Immunol. 26: 260 –267. 5. Slaughter, L., D. A. Carson, F. C. Jensen, T. L. Holbrook, and J. H. Vaughan. 1978. In vitro effects of Epstein-Barr virus on peripheral blood mononuclear cells from patients with rheumatoid arthritis and normal subjects. J. Exp. Med. 148: 1429 –1434. 6. Tosato, G., A. D. Steinberg, and R. M. Blaese. 1981. Defective EBV-specific suppressor T-cell function in rheumatoid arthritis. N. Engl. J. Med. 305: 1238 –1243. 7. Scotet, E., M. A. Peyrat, X. Saulquin, C. Retiere, C. Couedel, F. Davodeau, N. Dulphy, A. Toubert, J. D. Bignon, A. Lim, et al. 1999. Frequent enrichment for CD8 T cells reactive against common herpes viruses in chronic inflammatory lesions: towards a reassessment of the physiopathological significance of T cell clonal expansions found in autoimmune inflammatory processes. Eur. J. Immunol. 29: 973–985. 8. Lünemann, J. D., T. Kamradt, R. Martin, and C. Münz. 2007. Epstein-Barr virus: environmental trigger of multiple sclerosis? J. Virol. 81: 6777– 6784. 9. Toussirot, E., and J. Roudier. 2007. Pathophysiological links between rheumatoid arthritis and the Epstein-Barr virus: an update. Joint Bone Spine 74: 418 – 426. 10. Callan, M. F. C., L. Tan, N. Annels, G. S. Ogg, J. D. K. Wilson, C. A. O’Callagahan, N. Steven, A. J. McMichael, and A. B. Rickinson. 1998. Direct visualization of antigen-specific CD8⫹ T cells during the primary immune response to Epstein-Barr virus in vivo. J. Exp. Med. 187: 1395–1402. 11. Alspaugh, M. A., G. Henle, E. T. Lennette, and W. Henle. 1981. Elevated levels of antibodies to Epstein-Barr virus antigens in sera and synovial fluids of patients with rheumatoid arthritis. J. Clin. Invest. 67: 1134 –1140. 12. Yokochi, T., A. Yanagawa, Y. Kimura, and Y. Mizushima. 1989. High titer of antibody to the Epstein-Barr virus membrane antigen in sera from patients with rheumatoid arthritis and systemic lupus erythematosus. J. Rheumatol. 16: 1029 –1032. 1000 13. Inoue, N., S. Harada, N. Miyasaka, A. Oya, and K. Yanagi. 1991. Analysis of antibody titers to Epstein-Barr virus nuclear antigens in sera of patients with Sjogren’s syndrome and with rheumatoid arthritis. J. Infect. Dis. 164: 22–28. 14. Klatt, T., Q. Ouyang, T. Flad, I. Koetter, H. J. Buhring, H. Kalbacher, G. Pawelec, and C. A. Muller. 2005. Expansion of peripheral CD8⫹CD28⫺ T cells in response to Epstein-Barr virus in patients with rheumatoid arthritis. J. Rheumatol. 32: 239 –251. 15. Toussirot, E., D. Wendling, P. Tiberghien, J. Luka, and J. Roudier. 2000. Decreased T cell precursor frequencies to Epstein-Barr virus glycoprotein Gp110 in peripheral blood correlate with disease activity and severity in patients with rheumatoid arthritis. Ann. Rheum. Dis. 59: 533–538. 16. La Cava, A., J. L. Nelson, W. E. Ollier, A. MacGregor, E. C. Keystone, J. C. Thorne, J. F. Scavulli, C. C. Berry, D. A. Carson, and S. Albani. 1997. Genetic bias in immune responses to a cassette shared by different microorganisms in patients with rheumatoid arthritis. J. Clin. Invest. 100: 658 – 663. 17. Tosato, G., A. D. Steinberg, R. Yarchoan, C. A. Heilman, S. E. Pike, V. De Seau, and R. M. Blaese. 1984. Abnormally elevated frequency of Epstein-Barr virusinfected B cells in the blood of patients with rheumatoid arthritis. J. Clin. Invest. 73: 1789 –1795. 18. Balandraud, N., J. B. Meynard, I. Auger, H. Sovran, B. Mugnier, D. Reviron, J. Roudier, and C. Roudier. 2003. Epstein-Barr virus load in the peripheral blood of patients with rheumatoid arthritis: accurate quantification using real-time polymerase chain reaction. Arthritis Rheum. 48: 1223–1228. 19. Arnett, F. C., S. M. Edworthy, D. A. Bloch, D. J. McShane, J. F. Fries, N. S. Cooper, L. A. Healey, S. R. Kaplan, M. H. Liang, H. S. Luthra, et al. 1988. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 31: 315–324. 20. Stucki, G., M. H. Liang, S. Stucki, P. Bruhlmann, and B. A. Michel. 1995. A self-administered rheumatoid arthritis disease activity index (RADAI) for epidemiologic research: psychometric properties and correlation with parameters of disease activity. Arthritis Rheum. 38: 795–798. 21. Bickham, K., C. Münz, M. L. Tsang, M. Larsson, J. F. Fonteneau, N. Bhardwaj, and R. Steinman. 2001. EBNA1-specific CD4⫹ T cells in healthy carriers of Epstein-Barr virus are primarily Th1 in function. J. Clin. Invest. 107: 121–130. 22. Grogan, J. L., A. Kramer, A. Nogai, L. Dong, M. Ohde, J. Schneider-Mergener, and T. Kamradt. 1999. Cross-reactivity of myelin basic protein-specific T cells with multiple microbial peptides: experimental autoimmune encephalomyelitis induction in TCR transgenic mice. J. Immunol. 163: 3764 –3770. 23. Kamradt, T., and R. Volkmer-Engert. 2004. Cross-reactivity of T lymphocytes in infection and autoimmunity. Mol. Divers. 8: 271–280. 24. Currier, J. R., E. G. Kuta, E. Turk, L. B. Earhart, L. Loomis-Price, S. Janetzki, G. Ferrari, D. L. Birx, and J. H. Cox. 2002. A panel of MHC class I restricted viral peptides for use as a quality control for vaccine trial ELISPOT assays. J. Immunol. Methods 260: 157–172. 25. Dhodapkar, M. V., R. M. Steinman, J. Krasovsky, C. Münz, and N. Bhardwaj. 2001. Antigen-specific inhibition of effector T cell function in humans after injection of immature dendritic cells. J. Exp. Med. 193: 233–238. 26. Lünemann, J. D., N. Edwards, P. A. Muraro, S. Hayashi, J. I. Cohen, C. Münz, and R. Martin. 2006. Increased frequency and broadened specificity of latent EBV nuclear antigen-1-specific T cells in multiple sclerosis. Brain 129: 1493–1506. 27. Hislop, A. D., G. S. Taylor, D. Sauce, and A. B. Rickinson. 2007. Cellular responses to viral infection in humans: lessons from Epstein-Barr virus. Annu. Rev. Immunol. 25: 587– 617. 28. Münz, C., K. L. Bickham, M. Subklewe, M. L. Tsang, A. Chahroudi, M. G. Kurilla, D. Zhang, M. O’Donnell, and R. M. Steinman. 2000. Human CD4⫹ T lymphocytes consistently respond to the latent Epstein-Barr virus nuclear antigen EBNA1. J. Exp. Med. 191: 1649 –1660. 29. Münz, C. 2004. Epstein-Barr virus nuclear antigen 1: from immunologically invisible to a promising T cell target. J. Exp. Med. 199: 1301–1304. 30. Heller, K. N., J. Upshaw, B. Seyoum, H. Zebroski, and C. Münz. 2007. Distinct memory CD4⫹ T-cell subsets mediate immune recognition of Epstein Barr virus nuclear antigen 1 in healthy virus carriers. Blood 109: 1138 –1146. 31. Lee, S. P., J. M. Brooks, H. Al-Jarrah, W. A. Thomas, T. A. Haigh, G. S. Taylor, S. Humme, A. Schepers, W. Hammerschmidt, J. L. Yates, et al. 2004. CD8 T cell recognition of endogenously expressed Epstein-Barr virus nuclear antigen 1. J. Exp. Med. 199: 1409 –1420. 32. Voo, K. S., T. Fu, H. Y. Wang, J. Tellam, H. E. Heslop, M. K. Brenner, C. M. Rooney, and R. F. Wang. 2004. Evidence for the presentation of major histocompatibility complex class I-restricted Epstein-Barr virus nuclear antigen 1 peptides to CD8⫹ T lymphocytes. J. Exp. Med. 199: 459 – 470. 33. Tellam, J., G. Connolly, K. J. Green, J. J. Miles, D. J. Moss, S. R. Burrows, and R. Khanna. 2004. Endogenous presentation of CD8⫹ T cell epitopes from Epstein-Barr virus-encoded nuclear antigen 1. J. Exp. Med. 199: 1421–1431. 34. Gelder, C. M., J. R. Lamb, and B. A. Askonas. 1996. Human CD4⫹ T-cell recognition of influenza A virus hemagglutinin after subunit vaccination. J. Virol. 70: 4787– 4790. 35. Amyes, E., C. Hatton, D. Montamat-Sicotte, N. Gudgeon, A. B. Rickinson, A. J. McMichael, and M. F. Callan. 2003. Characterization of the CD4⫹ T cell EBV IN RA 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. response to Epstein-Barr virus during primary and persistent infection. J. Exp. Med. 198: 903–911. Appay, V., P. R. Dunbar, M. Callan, P. Klenerman, G. M. Gillespie, L. Papagno, G. S. Ogg, A. King, F. Lechner, C. A. Spina, et al. 2002. Memory CD8⫹ T cells vary in differentiation phenotype in different persistent virus infections. Nat. Med. 8: 379 –385. Hislop, A. D., N. H. Gudgeon, M. F. Callan, C. Fazou, H. Hasegawa, M. Salmon, and A. B. Rickinson. 2001. EBV-specific CD8⫹ T cell memory: relationships between epitope specificity, cell phenotype, and immediate effector function. J. Immunol. 167: 2019 –2029. Sallusto, F., J. Geginat, and A. Lanzavecchia. 2004. Central memory and effector memory T cell subsets: function, generation, and maintenance. Annu. Rev. Immunol. 22: 745–763. Thorley-Lawson, D. A. 2001. Epstein-Barr virus: exploiting the immune system. Nat. Rev. Immunol. 1: 75– 82. Hochberg, D., J. M. Middeldorp, M. Catalina, J. L. Sullivan, K. Luzuriaga, and D. A. Thorley-Lawson. 2004. Demonstration of the Burkitt’s lymphoma EpsteinBarr virus phenotype in dividing latently infected memory cells in vivo. Proc. Natl. Acad. Sci. USA 101: 239 –244. Laichalk, L. L., and D. A. Thorley-Lawson. 2005. Terminal differentiation into plasma cells initiates the replicative cycle of Epstein-Barr virus in vivo. J. Virol. 79: 1296 –1307. Gross, A. J., D. Hochberg, W. M. Rand, and D. A. Thorley-Lawson. 2005. EBV and systemic lupus erythematosus: a new perspective. J. Immunol. 174: 6599 – 6607. Chen, C., E. L. Prak, and M. Weigert. 1997. Editing disease-associated autoantibodies. Immunity 6: 97–105. Tiller, T., M. Tsuiji, S. Yurasov, K. Velinzon, M. C. Nussenzweig, and H. Wardemann. 2007. Autoreactivity in human IgG⫹ memory B cells. Immunity 26: 205–213. Yurasov, S., H. Wardemann, J. Hammersen, M. Tsuiji, E. Meffre, V. Pascual, and M. C. Nussenzweig. 2005. Defective B cell tolerance checkpoints in systemic lupus erythematosus. J. Exp. Med. 201: 703–711. Cohn, M., N. A. Mitchison, W. E. Paul, A. M. Silverstein, D. W. Talmage, and M. Weigert. 2007. Reflections on the clonal-selection theory. Nat. Rev. Immunol. 7: 823– 830. Samuels, J., Y. S. Ng, C. Coupillaud, D. Paget, and E. Meffre. 2005. Impaired early B cell tolerance in patients with rheumatoid arthritis. J. Exp. Med. 201: 1659 –1667. Scofield, R. H. 2004. Autoantibodies as predictors of disease. Lancet 363: 1544 –1546. Yang, L., M. Hakoda, K. Iwabuchi, T. Takeda, T. Koike, N. Kamatani, and K. Takada. 2004. Rheumatoid factors induce signaling from B cells, leading to Epstein-Barr virus and B-cell activation. J. Virol. 78: 9918 –9923. Scotet, E., J. David-Ameline, M. A. Peyrat, A. Moreau-Aubry, D. Pinczon, A. Lim, J. Even, G. Semana, J. M. Berthelot, R. Breathnach, et al. 1996. T cell response to Epstein-Barr virus transactivators in chronic rheumatoid arthritis. J. Exp. Med. 184: 1791–1800. Landais, E., X. Saulquin, E. Scotet, L. Trautmann, M. A. Peyrat, J. L. Yates, W. W. Kwok, M. Bonneville, and E. Houssaint. 2004. Direct killing of EpsteinBarr virus (EBV)-infected B cells by CD4 T cells directed against the EBV lytic protein BHRF1. Blood 103: 1408 –1416. Aloisi, F., and R. Pujol-Borrell. 2006. Lymphoid neogenesis in chronic inflammatory diseases. Nat. Rev. Immunol. 6: 205–217. Schroder, A. E., A. Greiner, C. Seyfert, and C. Berek. 1996. Differentiation of B cells in the nonlymphoid tissue of the synovial membrane of patients with rheumatoid arthritis. Proc. Natl. Acad. Sci. USA 93: 221–225. Randen, I., O. J. Mellbye, O. Forre, and J. B. Natvig. 1995. The identification of germinal centres and follicular dendritic cell networks in rheumatoid synovial tissue. Scand. J. Immunol. 41: 481– 486. Magliozzi, R., O. Howell, A. Vora, B. Serafini, R. Nicholas, M. Puopolo, R. Reynolds, and F. Aloisi. 2007. Meningeal B-cell follicles in secondary progressive multiple sclerosis associate with early onset of disease and severe cortical pathology. Brain 130: 1089 –1104. Serafini, B., B. Rosicarelli, D. Franciotta, R. Magliozzi, R. Reynolds, P. Cinque, L. Andreoni, P. Trivedi, M. Salvetti, A. Faggioni, and F. Aloisi. 2007. Dysregulated Epstein-Barr virus infection in the multiple sclerosis brain. J. Exp. Med. 204: 2899 –2912. Takeda, T., Y. Mizugaki, L. Matsubara, S. Imai, T. Koike, and K. Takada. 2000. Lytic Epstein-Barr virus infection in the synovial tissue of patients with rheumatoid arthritis. Arthritis Rheum. 43: 1218 –1225. Edwards, J. C., and G. Cambridge. 2006. B-cell targeting in rheumatoid arthritis and other autoimmune diseases. Nat. Rev. Immunol. 6: 394 – 403. Teng, Y. K., E. W. Levarht, M. Hashemi, I. M. Bajema, R. E. Toes, T. W. Huizinga, and J. M. van Laar. 2007. Immunohistochemical analysis as a means to predict responsiveness to rituximab treatment. Arthritis Rheum. 56: 3909 –3918.