Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
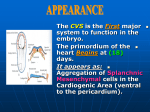
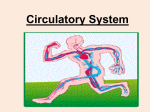
54 Case studies | August 2013 - Issue 1 Raghib syndrome: Echocardiographic features Ying Zhao MD, Ph D, Yi-hua He MD, Ph D and Wen-xu Liu MD Department of Ultrasound, Beijing Anzhen Hospital, Capital Medical University, Beijing, China Introduction A 25-year-old female was referred to our hospital with a 3 year history of palpitation and cyanosis. The chest X-ray was suggestive of pulmonary artery and right heart dilatation, and the ECG showed right ventricular hypertrophy. A transthoracic echocardiogram showed absent coronary sinus (CS) on the parasternal long axis view (Fig1A). The roof of coronary sinus was absent and a secundum type atrial septal defect (ASD) was also noticed on the apical four chamber view with left-to-right shunt from left atrium (LA) to right atrium (RA) through the absent coronary sinus, on color Doppler (Figs1B1C). The persistent left superior vena cava (PLSVC) was demonstrated on the suprastenal view. A right heart contrast echocardiography showed the micro-bubbles first appearing in the LA appendage, confirming the PLSVC draining into LA (Fig1D). Thus, the diagnosis was Raghib syndrome with secundum ASD, and the patient was referred for surgical repair. The surgical procedure showed completely unroofed CS and the PLSVC drained into LA between left appendage and left upper pulmonary vein. Rerouting the PLSVC into RA was successfully achieved by reroofing of the CS and reconstructing the atrial septum. A post-operative transthoracic echocardiogram showed the patch between the atrial septum and CS, no residual shunt between LA and RA and PLSVC draining into the RA (Figs2A-D). Fig1 Pre-operation echocardiogram Discussion A No CS was found from parasternal long axis view B The roof of CS was absent and the secundum type ASD was seen from apical four-chamber view (arrow) C Left-to-right shunt from LA to RA through the absent CS on color Doppler imaging (aoorw) D The right heart contrast echocardiography showed the bubble contrast first appeared in the LA confirming that the PLSVC drained into LA. (CS=coronary sinus; ASD= atrial septal defect; LA=left atrium; RA=right atrium; PLSVC= persistent left superior vena cava) Raghib syndrome is a special type of ASD which is known as coronary sinus spetal defect (CCSD), first described by Raghib 1. CCSD accounts for less than 1% of ASD and 0.1% of all congenital heart diseases (CHDs). CCSD is classified as three types according to completely or partially absent CS wall (Type I: complete; Type II: unroofed mid-portion and Type III: unroofed terminal portion) 2. Each type of CCSD is subsequently divided into 2 subtypes according to the presence of PLSVC: a) with PLSVC and b) without PLSVC. Type Ia is also called Raghib syndrome which includes absent CS, coronary sinus ASD and PLSVC draining into the LA between the appendage and left upper pulmonary vein 3 . The right superior vena cave is usually thin or completely absent. In inexperienced hands the Raghib syndrome could easily be missed with simple ASD, but detailed transthoracic echocardiographic examination with all modalities, color Doppler and bubble contrast should assist in achieving the complete diagnosis. The correct diagnosis should also guide towards optimum surgical planning which involves reroofing of the CS as well as rerouting the PLSVC rather than simple ASD patching 4. Fig2 Post-operation echocardiogram Correspondence to: Professor Yi-hua He, MD. Department of Ultrasound, Beijing Anzhen Hospital, Capital Medical University, Beijing, China Email: [email protected] Fax: + 0086 010-84005638 A The patch between the atrial septum and the coronary sinus level was noticed. B The left-to right shunt between atria was disappeared on color Doppler. C and D Two-dimentional and Color Doppler echocardiography showed the PLSVC flow drained into RA. (PLSVC= persistenr left superior vena cava, RA=right atrium) August 2013 - Issue 1 | Case studies References 1. Raghib G, Ruttenberg HD, Anderson RC, Amplatz K, Adams P, Jr., Edwards JE. Termination of Left Superior Vena Cava in Left Atrium, Atrial Septal Defect, and Absence of Coronary Sinus; a Developmental Complex. Circulation. 1965;31:906-18. 2. Ootaki Y, Yamaguchi M, Yoshimura N, Oka S, Yoshida M, Hasegawa T. Unroofed coronary sinus syndrome: diagnosis, classification, and surgical treatment. J Thorac Cardiovasc Surg. 2003;126:1655-6. 3. Xie MX, Yang YL, Cheng TO, Wang XF, Li K, Ren PP, et al. Coronary sinus septal defect (unroofed coronary sinus): Echocardiographic diagnosis and surgical treatment. Int J Cardiol. 2012 (Epub of print). 4. Takach TJ, Cortelli M, Lonquist JL, Cooley DA. Correction of anomalous systemic venous drainage: transposition of left SVC to left PA. Ann Thorac Surg. 1997;63:228-30. 55