Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
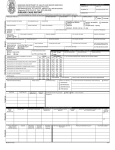
DRAFT Novel Coronavirus CASE Form CONFIDENTIAL v0.5 April 2013 Page 1 of 4 Possible case: please complete page 1&2 Confirmed case: please complete pages 1-4 Outcome details: please complete page 4 ALL CASES Date of Notification to Public Health Department: PATIENT INFORMATION Case ID Sex: F Surname M Unk Forename Date of Birth: Age (years): Address HSE Area CCA Phone number Country of birth Email address Occupation GP Name GP Address GP email GP Phone GP Fax CLINICAL DETAILS Imported Case type: Sporadic Secondary If imported, probable country of infection Date of diagnosis: Date of onset of 1st symptoms: Symptoms Cough Runny nose Headache Shortness of breath History of fever ≥ 380C (previous 14 days) Sneezing Sore throat Fever ≥ 380C Other symptom, please specify Yes No Unknown Chest x-ray evidence of pneumonia Yes No Unknown Suspicion parenchymal disease based on clinical evidence of pneumonia Did the case develop ARDS? Yes No Unknown Hospitalised due to nCov infection Yes Date of hospital admission No Unknown ARDS onset date Name of hospital Date of hospital discharge Was case mechanically ventilated? Yes Date mechanical ventilation started Duration of mechanically ventilation (days) No Was the case admitted to ICU Date of admission to ICU Yes No Did the case develop renal failure? Yes No Unknown Did case undergo ECMO? ECMO abroad ECMO country Yes No Unknown Yes No Unknown Outcome: Recovered Unknown Date mechanical ventilation finished Unknown Date of discharge from ICU Recovering Duration of ECMO (days) Deceased Unknown LABORATORY DETAILS Were specimens sent for respiratory viral screen? Yes Influenza A Results of respiratory viral screen result (tick all positive result that apply) Influenza B If other respiratory viral screen result, please specify: No Unknown Adenovirus RSV HMPV PIV1 PIV2 PIV3 DRAFT Novel Coronovirus CASE Form v0.5 April 2013 Page 2 of 4 Possible case: please complete page 1&2 Confirmed case: please complete pages 1-4 Outcome details: please complete page 4 ALL CASES EXPOSURE DETAILS Yes No Unk Did this possible case have contact with a confirmed case of Novel Coronovirus 10 days prior to onset? If yes, please give name of contact Did this possible case travel outside Ireland 10 days prior to onset? Yes Country (visited by CASE) Departure date Airport of arrival No Did this possible case travel within Ireland 10 days prior to onset? Town (visited by CASE) No Yes Unknown Arrival date Flight number Unknown Departure date Arrival date Yes No Unk Did this possible case have contact with someone who travelled to the Middle East (ME) 10 days prior to onset? If yes, what is the case’s relationship with traveller returned from ME? Country (visited by CONTACT) Departure date Arrival date Flight number Did the case have contact with any of the following during the 10 days prior to onset? Yes No Unk Yes No Unk Cow Goat Camel Sheep If contact with other animal, please specify: Location where animal contact occurred Yes No Unk Yes No Unk Other animal Bat Civet OCCUPATIONAL EXPOSURE DETAILS Is the case a Health Care Worker (HCW)? Yes No Unknown HCW job title No Unknown Direct patient contact? (e.g. hands on clinical contact) Yes HCW caring for patients with SARI in ICU? Yes No Unknown Type of patients cared for i.e. ICU, outpatients etc Does the case work in a laboratory handling specimens suspected to contain nCoV? Name & address of Health Care Facility/ laboratory where employed CLUSTER DETAILS Part of cluster? Yes CIDR outbreak ID Details of cluster location/setting Comments No Unknown Number symptomatic in cluster Yes No Unknown DRAFT Novel Coronovirus CASE Form v0.5 April 2013 Page 3 of 4 Possible case: please complete page 1&2 Confirmed case: please complete pages 1-4 Outcome details: please complete page 4 ALL CASES CLINICAL DETAILS - EXTENDED (Confirmed cases only) Symptoms (continued): Diarrhoea Arthralgia Vomiting Myalgia Altered consciousness Other please specify Anorexia Nausea Fatigue Rash Nose bleed Headache Seizures Conjunctivitis Maximum temp (oC) Complications: Cardiac arrest Chest X-ray evidence of pneumonia Hypotension requiring vasopressors Underlying medical conditions: please tick all that apply Chronic heart disease Chronic neurological disease Chronic kidney disease Chronic liver disease Diabetes BMI Chronic respiratory disease (excl. asthma requiring medication) Other co-morbidity, please specify: Was the case pregnant? Yes If yes, what is the current trimester? 1st No Unknown 2nd 3rd Does the case currently smoke? No Unknown Yes Transplant recipient (organ/marrow) HIV/ Other immunesuppressive illness Malignancy Asthma requiring medication Pregnancy outcome Estimated delivery date Yes No Unk Case vaccinated with pneumococcal vaccine? Case vaccinated with current seasonal influenza vaccine? Antiviral treatment prescribed? Ribavarin Start date Ribavarin finish date Yes Visited GP? 1st GP visit date No Visited ED? Yes 1st ED visit date No Ribavirin only Pneumococcal vaccine date Influenza vaccine date Other antiviral Unknown 2nd GP visit date Case admitted to hospital? 3rd GP visit date Unknown 2nd ED visit date Yes Name of 1st admitting hospital 1st discharge diagnosis 1st Hospital admission source: Name of 2nd admitting hospital 2nd discharge diagnosis 2nd Hospital admission source: Name of 3rd admitting hospital 3rd discharge diagnosis 3rd Hospital admission source: Antiviral combination Other antivirals start date Other antivirals finish date No 3rd ED visit date Unknown Community Date of 1st admission Date of 1st discharge Other ward in same hospital Other hospital Community Date of 2nd admission Date of 2nd discharge Other ward in same hospital Other hospital Community Date of 3rd admission Date of 3rd discharge Other ward in same hospital Other hospital DRAFT Novel Coronovirus CASE Form v0.5 April 2013 Page 4 of 4 Possible case: please complete page 1&2 Confirmed case: please complete pages 1-4 Outcome details: please complete page 4 ALL CASES LABORATORY RESULTS (Confirmed cases only) Laboratory name Specimen collected date Laboratory result date Specimen type BAL Specimen ID NCoV test result NPA Pos Neg equivocal Plasma Nose swab Sputum Finger prick Serum Throat swab Oral fluid Tissue Was baseline serology taken on case? Date baseline serology taken Yes No Faeces Unknown Date baseline serology sent to NVRL OUTCOME DETAILS - All Case classification: Outcome Confirmed Still ill Possible Recovering Denotified Recovered Deceased Was a post-mortem examination performed? Unknown Underlying/primary Contributary/secondary Yes No No contribution to death Awaiting Coroners report Unknown Cause of death as per medical certificate of death Result of coroners report (where applicable) SECONDARY BACTERIAL INFECTIONS Did case have secondary bacterial infection Yes If yes, please specify positive result: H. influenzae S. pneumoniae Other organism, please specify: No Unknown S. aureus MRSA E. coli Other organism POST-EXPOSURE SEROLOGY (21 days after 1st exposure) Was post-exposure serology (21 days after exposure) taken on case? Date post-exposure serology taken Yes No Unknown Date post-exposure serology sent to NVRL REPORTER DETAILS Reporter name Reporter phone Reporter HSE Date of case interview Unknown If deceased, date of death: Date of symptom resolution in the case If deceased, was nCoV contributing factor: Lost to follow up Reporter position Reporter email Reporter fax Date case notified to HPSC Unknown Pending