Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
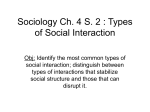
ARTICLE Changes in anterior chamber depth during accommodation: a pilot study Antonio J. Del Águila-Carrasco, MSc; Alberto Domínguez-Vicent, MSc; Daniel Monsálvez-Romín, OD; Cari Pérez-Vives, MSc; Vicent Sanchis, MSc PURPOSE: To study anterior chamber depth (ACD) behaviour in different positions, with different degrees of accommodation. SETTING: Academic department associated to a regional hospital. METHODS: ACD data were acquired from 20 young, healthy subjects under 8 different vergences, from +2 dioptres (D) to –5 D using a Pentacam HR device. Measurements were taken for the central zone of the ACD and for 4 more positions, each in a different direction (superior, inferior, nasal and temporal), 2 mm from the centre. RESULTS: Changes in each position of the ACD resulting from accommodation were small and generally insignificant (P > 0.05). The statistically deepest ACD value for all vergences was found at the central position. The superior-nasal and temporal-inferior pairs did not show statistically significant differences (P > 0.05) for all vergences. In addition, temporal and inferior chamber depths were statistically significantly deeper (P < 0.05) than superior and nasal chamber depths. CONCLUSIONS: While the central position presents the deepest ACD, the superiornasal pair presents the narrowest ACD. No significant changes in ACD occur after 5 D of accommodation. J Emmetropia 2013; 4: 87-91 Submitted: 02/26/2013 Revised: 03/11/2013 Accepted: 03/13/2013 Optometry Research Group (GIO), Department of Optics. University of Valencia. Spain. Acknowledgements: This research was supported in part by Research Grant #SAF2009-13342-E# awarded by the Ministry of Science and Innovation (Ministerio de Ciencia e Innovación), by a Atracció de Talent research scholarship (Universidad de Valencia) awarded to Alberto Domínguez Vicent, by a collaboration scholarship (Ministerio de Educación, Ciencia y Deporte) awarded to Daniel Molsálvez Romín and by a VALi+D research scholarship (Generalitat Valenciana) awarded to Cari Pérez-Vives. Financial disclosure: The authors have no proprietary interest in any of the products or devices mentioned in this article. Corresponding author: Antonio J. Del Águila-Carrasco Department of Optics – University of Valencia c/Dr. Moliner, 50 – 46100 – Burjassot – Spain e-mail: [email protected] © 2013 SECOIR Sociedad Española de Cirugía Ocular Implanto-Refractiva Many papers have been published on the changes of different anatomical structures of the eye during accommodation, such as anterior chamber depth (ACD)1-4,6-14,16-28, anterior chamber angle (ACA)16, or pupil diameter3,5,8,26,27. In these studies, it was observed that the values of these anatomical structures decrease after increasing the vergence of the fixation target (Figure 1 shows an example of changes in ACD as a function of accommodation). The issue with these studies is that all the ACD measurements were taken only in the central zone, without measuring changes in peripheral ACD during accommodation. It would be interesting to determine these changes, with the aim of developing new models of intraocular lenses (IOLs) and improving on current models. These new IOLs should protect the intraocular anatomical structures, such as corneal endothelium, iris or crystalline lens, from possible disorders or disturbances caused by the contact of the lens with ISSN: 2171-4703 87 88 CHANGES IN ACD DURING ACCOMODATION any of these structures after surgery. Additionally, since accommodation could lead to changes in various anatomical structures, it is important to study changes in ACD at different levels of accommodation, and also in different positions, not only the central zone. The more that is known about the modifications that occur in the eye while accommodating or when it is relaxed, the better designed the IOLs will be. Consequently, it will be easier to differentiate those subjects who are candidates for IOL implantation from those who do not have an appropriate ACD value in any determined zone. The aim of the present study was to analyse changes in central and peripheral ACD during accommodation. To the authors’ best knowledge, this is the first report that evaluates these ocular changes during accommodation. PATIENTS AND METHODS Subjects Twenty right eyes from twenty individuals, 9 male and 11 female, aged from 20 to 30 years (23.20 ± 1.68 years) were included in this study. Spherical refractive errors ranged between –0.50 to +0.50 dioptres (D), the mean spherical refractive error being 0.23 ± 0.28 D. They had clear intraocular media and no known ocular disease. All patients were informed about the details of this study, and written informed consent was obtained after verbal and written explanation of the nature and possible consequences of the study, in accordance with the Declaration of Helsinki. No Institutional Review Board approval was required for this Figure 1. Changes in anterior chamber depth during accommodation in different positions of the anterior chamber. study. Subjects with best-corrected visual acuity of less than 20/40, ocular or systemic disease, ocular surgery history, intraocular pressure higher than 21 mmHg and presence of retinal or optic disk disease, were excluded from taking part in this study. Pentacam HR The Pentacam HR instrument uses a rotating Scheimpflug camera for the non-invasive measurement of the anterior segment (Figure 2). This camera calculates a three-dimensional model of the anterior segment. The system has two different three-dimensional modes: a regular three-dimensional scan that takes 50 images in 2 seconds, and a special three-dimensional high-resolution corneal mode, in which the camera takes 50 images in 1 second. The Pentacam automatically captures images once correct alignment in the x, y, and z directions is attained. After image capture, the instrument analyses the 50 Scheimpflug images of the anterior eye to reconstruct the anterior segment, thus providing information about corneal curvature (front and back surfaces), corneal elevation (front and back corneal surfaces), pachymetry maps and ACD information. The instrument generates a quality setting reading for each measurement, providing information on the reliability of each 3D scan. Studies show that the Pentacam has excellent repeatability and first-rate interobserver reproducibility for measuring ACD15. Moreover, the Pentacam HR has a red LED that can be used as a fixation target and moved in 0.5 D steps from +2 D to –5 D. Before each measurement, the subject was instructed to maintain the fixation target in focus during the measurement. Figure 2. Pentacam HR device connected to a computer. JOURNAL OF EMMETROPIA - VOL 4, APRIL-JUNE CHANGES IN ACD DURING ACCOMODATION Experimental procedure The Pentacam HR was used to automatically measure central and peripheral ACD for far vision and for different positions of the fixation target. The central ACD was defined as the distance between the corneal endothelium and the anterior surface of the crystalline lens. The peripheral ACD was measured at 2 mm from the centre of the cornea in nasal, temporal, superior and inferior directions. For these four positions, the ACD was measured as the distance between the corneal endothelium and the iris. The resolution of these measurements was 0.01 mm in both cases. ACD was measured 3 times per eye, and the average value was retained for all distances evaluated, ranging from +2 D to –5 D in steps of 1 D. Before starting the measurements, the volunteer had to fixate the target for 2 seconds to allow an appropriate accommodation response. During the measurements, the patient was requested to not blink, to avoid affecting the measurement. This procedure was performed during a single session. The ACD was expressed in millimetres. All measurements were carried out by the same specialist, who did not know the objective of this study and had experience using the Pentacam HR. 89 study was to compare results under different conditions (accommodative stimulus and anatomical localisation), the study design is factorial, so a repeated measures ANOVA was used and the assumption of normality was ensured by means of the Shapiro-Wilk test. A post-hoc multiple comparison test using the Holm Sidak method was performed when ANOVA revealed differences. Statistical significance was set at P = 0.05. RESULTS Figure 3 shows the variation in ACD during accommodation in the five different positions (central position, and 2 mm in a nasal, temporal, inferior and superior direction) where measurements were taken. A small reduction in ACD occurred as accommodation increased in all cases, but this reduction was not statistically significant at any position of the anterior chamber (P > 0.05). The results show that central position gives the statistically deepest ACD for all vergences, while the superior-nasal and temporal-inferior pairs were not statistically significantly different (P = 0.056 and P = 0.225, respectively). Nevertheless, temporal and inferior chamber depths were statistically significantly greater (P < 0.05) than superior and nasal chamber depths. Statistical analysis After data collection, anterior chamber depth measurements were exported from the instrument for further analysis. Statistical analysis was performed using SigmaPlot for Windows Version 11 (Systat Software, GmbH; Erkrath, Germany). Since the main goal of the DISCUSSION The aim of this study was to evaluate the behaviour of the ACD in different positions at different levels of accommodation. The use of the Pentacam HR device allowed us to perform the measurements in a Figure 3. Comparison of the anterior chamber depth from a subject with relaxed accommodation (above), and the ACD from the same subject when the level of accommodation is set at –5 D (below). Note the slight decrease in the ACD when the level of accommodation increases. JOURNAL OF EMMETROPIA - VOL 4, APRIL-JUNE 90 CHANGES IN ACD DURING ACCOMODATION non-invasive way. Figure 3 shows the decrease in ACD when accommodation is increased. This happens at the five positions analysed. However, these changes were small and no statistically significant differences were found for the positions evaluated. This indicates that there is practically no modification of the ACD during accommodation. Our results are similar to those obtained previously10,11,17,22,24,27, in which the mean ACD change after accommodation was about 0.1 mm. However, these results contradict those of Du et al.7, where the mean ACD change was 0.17 mm. This difference may be because the cited report studied changes in ACD after pharmacological accommodation. In Figure 3, ACD appears to vary considerably for each position of measurement within the same degree of accommodation (same fixation object vergence). For the same level of accommodation, our results revealed statistically significant differences between the ACD for all positions, except for the inferior and temporal positions (no differences), and superior and nasal positions (no differences either), indicating that the anterior chamber shows variations in depth that are not negligible. It is important to take this into consideration before IOL implantation (angle-supported anterior chamber lenses, iris-fixated lenses, etc.), or for checking already implanted IOLs for possible post-surgery problems. It is extremely important that the intraocular lens does not make contact with any anatomical structure of the eye, in order to prevent disturbances or disorders in the corneal endothelium, the iris, the crystalline, or in the anterior chamber itself. For this reason, it is essential to know as much as possible about the anterior chamber. ACD measurements in different positions before surgery are useful for preventing these disturbances, and also for designing new IOLs or improving those that are currently available. It is fair to mention the limitations of this study, such as the number of eyes measured, the fact that we only used one device to measure ACD and also that a small age range was included. In summary, although there are practically no changes in ACD during accommodation, this parameter changes appreciably depending on the position where the measurement has been taken. This is an important factor in the design and implantation of IOLs. REFERENCES 1. 2. Alderson A, Davies LN, Mallen EA, Sheppard AL. A method for profiling biometric changes during disaccommodation. Optom Vis Sci. 2012; 89:E738-E748. BaikoffG, LutunE, Wei J, Ferraz C. Anterior chamber optical coherence tomography study of human natural accommodation in a 19-year-old albino. J Cataract Refract Surg. 2004; 30:696– 701. 3. Baikoff G, Lutum E, Ferraz C, Wei J. Static and dynamic analysis of the anterior segment with optical coherence tomography. J Cataract Refract Surg. 2004; 30:1843-1850. 4. Bolz M, Prinz A, Drexler W, Findl O. Linear relationship of refractive and biometric lenticular changes during accommodation in emmetropic and myopic eyes. Br J Ophthamol. 2007; 91:360-365. 5. Charman WN, Radhakrishnan. Accommodation, pupil diameter and myopia. Ophthal Physiol Opt. 2009; 29:7279. 6. Drexler W, Baumgartner AA, Findl O, Hitzenberger CK, Fercher AF. Biometric investigation of changes in the anterior eye segment during accommodation. Vision Res. 1997; 37:2789-2800. 7. Du C, Wang J, Wang X, Dong Y, Gu Y, Shen Y. Ultrasound biomicroscopy of anterior segment accommodative changes with posterior chamber phakic intraocular lens in high myopia. Ophthalmology. 2012;119:99-105. 8. Du C, Shen M, Li M, Zhu D, Wang MR, Wang J. Anterior segment biometry during accommodation imaged with ultralong scan depth optical coherence tomography. 2012; 119(12):2479-85. 9. Dubbelman M, van der Heijde GL, Weeber HA. Change in shape of the aging human crystalline lens with accommodation. Vision Res. 2005; 45:117-132. 10. Garner LF, Yap MK. Changes in ocular dimensions and refraction with accommodation. Ophthal Physiol Opt. 1997; 17:12-17. 11. KaluznyBJ. Anterior movement of the crystalline lens in the process of accommodation in children. Eur J Ophthalmol. 2007. 17:515-20. 12. Kasthurirangan S, Markwell EL, Atchison DA, Pope JM. MRI study of the changes in crystalline lens shape with accommodation and aging in human. J Vis. 2011; 11:19,113. Kirschkamp T, Dunne M, Barry JC. Phakometric measurement of ocular surface radii of curvature, axial separations and alignment in relaxed and accommodated human eyes. Ophthal Physiol. Opt. 2004; 24:65-73. 14. Koretz JF, Cook CA, Kaufman PL. Accommodation and presbyopia in the human eye. Changes in the anterior segment and crystalline lens with focus. Invest Ophthalmol Vis Sci. 1997; 38:569-578. 15. Lackner B, Schmidinger G, Skorpik C. Validity and repeatability of anterior chamber depth measurements with Pentacam and Orbscan. Optom Vis Sci. 2005; 82:858–861. 16. Marchini G, Pedrotti E, Modesti M, Visentin S, Tosi R. Anterior segment changes during accommodation in eyes with a monofocal intraocular lens: High-frequency ultrasound study. J Cataract Refract Surg. 2008; 34:949956. 17. MalyuginBE, Shpak AA, Pokrovskiy DF. Accommodative changes in anterior chamber depth in patients with high myopia. J Cataract Refract Surg. 2012; 38:1403-1407. 18. Ni Y, Liu XL, Wu MX, Lin Y, Sun YY, He C, Liu YZ. Objective evaluation of the changes in the crystalline lens during accommodation in young and presbyopic populations using Pentacam HR system. Int J Ophthalmol. 2011; 4:611615. 19. Ostrin L, Kasthurirangan S, Hall DW, Glasser A. Simultaneous measurement of refraction and A-scan biometry during accommodation in humans. Optom Vis Sci. 2006; 83:657-665. JOURNAL OF EMMETROPIA - VOL 4, APRIL-JUNE 91 CHANGES IN ACD DURING ACCOMODATION 20. Petternel V, Köppl CM, Ruhswurm ID, Findl O, Skorpik C, Drexler W. Effect of accommodation and pupil size on the movement of a posterior chamber lens in the phakic eye. Ophthalmology. 2004; 111:325-331. 21. Poinoosawmy D, Nagasubramanian S, Brown NA. Effect of pilocarpine on visual acuity and on the dimensions of the cornea and anterior chamber. Brit J Ophthal. 1976; 60:676679. 22. Read SA, Collins MJ, Woodman EC, Cheong SH. Axial Length Changes During Accommodationin Myopes and Emmetropes. Optom Vis Sci. 2010; 87:656–662. 23. Read SA, Buehren T, Collins MJ. Influence of accommodation on the anterior and posterior cornea. J Cataract Refract Surg. 2007; 33:1877–1885. 24. Ruggeri M, Uhlhorn SR, de Freitas C, Ho A, Manns F, Parel JM. Imaging and full-length biometry of the eye during accommodation using spectral domain OCT with an optical switch. Biomed Opt Express. 2012; 3:1506-20. 25. Tsorbatzoglou A, Németh G, Széll N, Biró Z, Berta A. Anterior segment changes with age and during accommodation measured with partial coherence interferometry. J Cataract Refract Surg. 2007; 33:1597-1601. 26. Yan PS, Lin HT, Wang QL, Zhang ZP. Anterior segment variations with age and accommodation demonstrated by slitlamp adapted optical coherence tomography. Ophthalmology. 2010; 117:2301-2307. 27. Yuan Y, Chen F, Shen M, Lu F, Wang J. Repeated measurements of the anterior segment during accommodation using long scan depth optical coherence tomography. Eye Contact Lens. 2012; 38:102-108. 28. Zhou C, Wang J, Jiao S. Dual channel dual focus optical coherence tomography for imaging accommodation of the eye. Opt Express. 2009; 17(11):8947–8955. JOURNAL OF EMMETROPIA - VOL 4, APRIL-JUNE First author: Antonio J. Del Águila-Carrasco Optometry Research Group (GIO), Department of Optics. University of Valencia. Spain.