Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
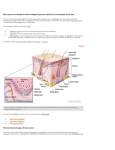
If its dry wet it, if its wet dry it Ummm Not always! Alastair Dickson, Jess Gilmour & Tonya de Bique >Ğƚ͛ƐƚĂůŬĂďŽƵƚƐŬŝŶĐĂŶĐĞƌ http://youtu.be/qnp-‐4AGeXs8 The skin Epidermis ± Flat squamous cells Basal cells ± Round cells in epidermis ± Below squamous cells Melanocytes ± Scattered amongst basal cells ± Reside deepest part of epidermis Dermis ± Below epidermis ± Multiple types cells + structures ± Include glands, blood + lymph vessels ± Sweat + sebum reach skin surface through pores Types of cancer cells Pre-‐cancerous lesions ± Aktinic keratoses Benign growths ± Non-‐invasive ± Typically rĞŵŽǀĞĚнĚŽŶ͛ƚƌĞƚƵƌŶ ± viz moles Malignant ± Maybe threat to life ± Often can be removed but can grow back Common types of skin cancer Basal cell skin cancer (BCC) Squamous cell skin cancer (SCC) Melanoma Frustrated grandparent Loves the outdoors. Does lots of hiking. Fed-‐up with his dry, wrinkly skin. Now grandchildren questioning why ŚĞ͛ƐŐŽƚŚŽƌŶƐ͍ Is this normal? Is it cancerous? tŚĂƚ͛ƐLJŽƵƌƚŚŽƵŐŚƚƐ͍ tŚĂƚ͛ƐLJŽƵƌƉůĂŶ͍ Any suggestions for skin care/prevention? Aktinic keratoses ͞dŚŝĐŬĞŶĞĚ͕ƐĐĂůLJŐƌŽǁƚŚĐĂƵƐĞĚďLJƐƵŶůŝŐŚƚ͟ Occur on sun exposed areas of skin ± Esp back hands, face namely nose, cheeks, upper lip, temple + forehead Multiple flat or thickened, scaly or warty, skin coloured or reddened lesions. ± Can develop into a cutaneous horn ± Cells show characteristic UV-‐induced gene mutations Risk factors include sun exposure, tanning booths. Be suspicious if see signs sun damaged skin ± Dry, discoloured, wrinkled skin Most lesions do not progress to malignancy but increased risk of SCC Ulcerous dog bite Retired farmer, from highlands of Scotland Annoyed with his ulcer. Wants it freezing off. Blames his terrier for biting him after had been chasing rats. What are your thoughts? What hx would you take. Describe the lesion DDx? Plan? BCC Also known as Rodent ulcer Typically looks like small inflamed crater with a raised edge Starts basal layers of skin Typically occurs in sun-‐exposed areas of skin ± Commonest place is face Commonest type skin Ca in caucasians ± More common closer to equator, high altitudes Age ± 5 times more likely in people aged than in 50-‐55 year old Rarely metastasises A bad case of dermatitis Retired cleaner Lots of dermatitis in past. Worried cos this seems different. Worse than before and now getting joint pain. What do you think/your concerns? Is it dermatitis/something else? What questions are relevant here? Describe the lesion? ± Any worrying features? What examination would you do? tŚĂƚ͛ƐLJŽƵƌƉůĂŶ͍ What are you going to tell the patient? What are their likely top questions/concerns? SCC Affects squamous cells Appearance: ± Typically starts as small crusted or scaly area of skin with red or pink base. ± May grow into lump looking like a wart. ± May ulcerate or bleed intermittently-‐ i.e. It ĚŽĞƐŶ͛ƚĂƉƉĞĂƌƚŽŚĞĂů͘ ± Left untreated will grow + damage nearby structures possibly eroding them completely Most common type skin Ca in dark skinned persons Dark skinned persons affects non-‐sun exposed skin ± Legs or feet Caucasians typically affects sun exposed skin ± Head, face, ears + neck Sometimes metastasises ŽǁĞŶ͛ƐŝƐĞĂƐĞ Early form of SCC Also known as precancerous dermatitis or precancerous dermatosis Risk factors include prolonged exposure to arsenic + HPV16, HPV2 ± Query if factory worker, esp chemicals industry Occurs on sun-‐exposed areas of skin Older white men esp prone Appearance reddish, scaly or thickened patch of skin Requires treatment to prevent it growing deeper into skin ± ± Topical 5-‐fluorouracil cream Imiquimod 5% cream on lower limbs Unsightly freckle New GP Your next pt is 24 yr old lady w fair complexion + ŵƵůƚŝƉůĞ͚ĨƌĞĐŬůĞƐ͛͘ She is concerned about 1 of the freckles on her thigh which has become unsightly over past 9 months. No discomfort. What type of hx would you take? Describe the lesion What examination(s) would you do? What are your concerns? What is the patient likely to be worried about? What would you do next? Melanoma Occurs in melanocytes Can occur on any skin surface ± Men: typically head, neck, between shoulders + hips ± Women: typically lower legs, between shoulders + hips Rare in people with dark skin ± Different range of distribution in such persons ± Typically under finger or toe nails, palms of hand or soles of feet Commonly metastasises ± Typically fatal if does o ?post excision screening f/u worthwhile for re-‐occurence ± New drugs available/forthcoming, variable estimates on effectiveness Symptoms of melanoma: ABCDE Asymmetry Irregular border ± Edges often ragged, notched or blurred ± Pigment diffusion into surrounding skin Uneven colour ± Shades of black, brown + tan ± May also see other shades: white, gray, red, pink or blue Diameter ± Change in size, typically larger (but not always) ± ĞƐƵƐƉŝĐŝŽƵƐŝĨĚŝĂŵĞƚĞƌшϲŵŵ;ϭͬϰ͞Ϳ ± But can be tiny Evolving ± Changing/changed over recent weeks/months Melanoma-‐ Other More advanced ± Texture may change Skin surface may breakdown ± ± ± ± Scrapped look Hard or lumpy Oozing or bleeding surface Itchy, tender or painful Rationing + referrals Worried/concerned ± 2 week NHS referral rule Need 2nd opinion, no suspicion malignancy ± In-‐house GPwSI ± Refer dermatology Cosmetic removal ± Private referral ± Primary or secondary care ± Multiple providers Diagnosis Initially via biopsy 4 types of biopsy ± shave biopsy No stitches required ± Punch biopsy Circle of tissue removed from abnormal area ± Incisional biopsy Surgical removal of part of lump or suspicious area removed ± Excisional biopsy Entire growth + margin of surrounding tissue surgically excised Most commonly used when suspicion of melanoma Staging of BCC & SCC Stage 0 ± Carcinoma in situ ± Involves only top layer of skin Stage I ± 'ƌŽǁƚŚчϮĐŵĚŝĂŵĞƚĞƌ;ůĂƌŐĞĂƐƉĞĂŶƵƚͿ Stage II ± 'ƌŽǁƚŚшϮĐŵĚŝĂŵĞƚĞƌ Stage III ± Cancer has invaded below the skin to cartilage, muscle or bone ± Or cancer has spread to adjacent lymph nodes ± No other spread Stage IV ± Metastatic spread ± More commonly SCC Staging of melanoma Stage 0 ± Only involves the top layer of skin ± Melanoma in situ Stage I ± dƵŵŽƵƌŝƐчϭŵŵƚŚŝĐŬнƐŬŝŶƐƵƌĨĂĐĞĂƉƉĞĂƌƐďƌŽŬĞŶĚŽǁŶ ± Tumour is 1-‐2mm thick but skin surface appears intact Stage II ± Tumour 1-‐2mm thick + surface appears broken down ± Thickness > 2mm (+ surface may appear broken down) Stage III ± 1 or more adjacent lymph nodes involved ± Invasion of adjacent structures Stage IV ± Metastasis has occurred WĂƚŝĞŶƚƐ͛ĨĞĂƌƐΘĞdžƉĞĐƚĂƚŝŽŶƐ What are patients worried about? How do you elicit their fears + concerns? How do you calm them? How do you make sense of it all? With increasing rationing, esp of dermatology, what back-‐ƵƉƉůĂŶƐĚŽǁĞŚĂǀĞŝĨǁĞĐĂŶ͛ƚƌĞĨĞƌ͍ Prognosis All 3 types are curable if identified + treated early. Non-‐melanoma skin cancers ± 95% cure rate Melanomas ± Low if metastasized ± Current estimates w existing Tx 10-‐20% at 2 years [Robert et. al.; Ipilimumab plus dacarbazine for previously untreated metastatic melanoma; NEJM; 30/6/11; 364: 2517-‐26] Prevention Important patients know what to check for + how http://youtu.be/TKyiWt4MH7o Important patients know how to protect themselves against further sun damage ± How do we do this? References http://dermnetnz.org/ www.dermis.net www.patient.co.uk Guidelines for the management of basal cell carcinoma, British Association of Dermatologists (2008) Multiprofessional Guidelines for the Management of the Patient with Primary Cutaneous Squamous Cell Carcinoma, British Association of Dermatologists (2002) The prevention, diagnosis, referral and management of melanoma of the skin, Royal College of Physicians and British Association of Dermatologists (September 2007) NICE Clinical Guideline; Skin tumours including melanoma. February 2006 and update 2011