Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
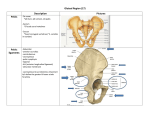
Alleviating Piriformis Syndrome 4 Contact Hours Learning Objectives At the end of this workshop you will: • Be able to list the relevant soft-tissue structures. Instructor: Bob McAtee, RMT, CSCS, C-PT Pro-Active Massage Therapy Colorado Springs, CO 719-475-1172 www.stretchman.com Defining Piriformis Syndrome • Piriformis syndrome, first described in the literature in 1928, is the name given to a complex of symptoms arising from compression of the sciatic nerve and/or associated blood vessels by the piriformis muscle. Sciatica or Piriformis Syndrome? • In PS, pain generally originates at or below the sciatic notch of the sacrum (neuritis). • In sciatica, the pain originates at the lumbar spine, because the sciatic nerve is being entrapped at the spinal level (radiculopathy). • Be able to demonstrate proper palpation techniques. • Be able to perform seated, prone, and side-lying assessment techniques. • Be able to demonstrate the three-part treatment protocol. • Leave the seminar confident and capable of integrating these techniques into your repertoire. Typical Symptoms • The most common symptoms of piriformis syndrome are pain and paresthesia in the buttock and down the back of the thigh. • Commonly felt when sitting, climbing stairs (or hills), squatting, running, cycling. Differential Diagnosis • Trochanteric Bursitis • Lumbar Degenerative Disc • Lumbar Facet Dysfunction • Lumbar Spondylosis or Spondylolisthesis 1 Elements of Piriformis Syndrome • Three components: nerve and vascular entrapment, SI joint dysfunction, and trigger points in the muscle. • Entrapment most often occurs at the sciatic notch. In some cases, the piriformis is too large, and leaves little room for the sciatic nerve and associated blood vessels. • Chronic hypertonicity of the piriformis can be sufficient to fill the foramen and compress the nerve. S-I Joint/Piriformis Because of its origin on the anterior sacrum, piriformis can produce a rotary shearing force on the SI joint which would tend to displace the top of the sacrum anteriorly. • This may force the PSIS anteriorly when compared to the opposite side. Sacrum Variations These sacrum are curved differently because the five vertebral bones that form them are differently shaped. This leads to different natural spinal curves and different ranges of motion. Sciatic Nerve Variations From Beaton, L.E. and B.J. Anson. The relation of the sciatic nerve and its subdivisions to the piriformis muscle. Anat. Rec. 70:1-5, 1938 S-I Joint/Piriformis • Manipulation of the SI without resolving piriformis hypertonicity gives only temporary relief. • Attempting to relieve piriformis tightness without addressing the SI displacement is also a temporary fix. Perpetuating Factors • Symptoms may be aggravated by: • Prolonged sitting • Sitting with the affected leg crossed over the opposite knee • Overstretching (not too often, but to aggressively). • Activity, such as running uphill or downhill, cycling in low gears, ballet and modern dance, or repetitive motions that overload the piriformis in its role as a stabilizer of the hip (eccentric stress). 2 No Diagnosis • As massage therapists, we are not legally qualified to diagnose or prescribe. • However, it is within our scope of practice to evaluate soft-tissue to determine if we can offer appropriate treatment or if the client needs to be referred to another professional. • For this seminar, we will be using an abbreviated form of assessment that focuses on the functional integrity of the musculotendinous tissues. Acetabulum Variations: Rotation • Front view of two pelvises: You can see the hip sockets of the left specimen but not the right. This is because the sockets are oriented in different directions. • Side view:Same specimens, side-view. Movements of the femur that are easy for one might be impossible for the other because the femur would compress against the edges of the hip socket (acetabulum). Normal Rotation ROM of the Hip Internal rotation: 35°- 45° External rotation: 45° It’s best to compare affected and unaffected sides to try and establish “normal” for each client. Visual Assessment • With client supine and relaxed: • Compare lateral rotation of the legs. • Excessive lateral rotation (>450) indicates piriformis shortening on that side. Femur Variations: Rotation • This view illustrates how femurs all have different degrees of spiral or twist to their shafts. Assessment: Pace Abduction Test This is a standard test for piriformis syndrome • With the client seated, knees flexed and hanging over the edge of the table, place your hands on the lateral knees and ask the client to push against your resistance. • Pain, faltering or weakness is positive for piriformis involvement. • This test is better than resisted lateral rotation because it eliminates the other five lateral rotators. 3 Sidelying Assessment •Sidelying, with the hip flexed to 90°: –Resisted horizontal abduction: –may put stress on the sciatic nerve, as the muscle contracts. –Passive horizontal adduction: –stretches the piriformis and may compress the sciatic nerve. Palpation: Piriformis • The piriformis lies deep to the gluteus maximus, which must remain relaxed during palpation. Palpating Piriformis • Palpate the piriformis at the level of its insertion into the greater trochanter. • Deep tenderness inferior to piriformis is probably coming from the gemelli, obturator internus, or quadratus femoris. • Palpation along the length and across the grain of the muscle may reveal tenderness, taut bands, trigger points, and “nervy” pain. Additional Assessment • Assessment of the piriformis can also include: • Prone, with the knee flexed to 90°: – Passive medial rotation, stretches the piriformis and may compress the sciatic nerve. – Passive lateral rotation, shortens and bunches the piriformis at the sciatic notch. – Resisted lateral rotation, may put stress on the sciatic nerve as the muscle contracts. Palpation: Bony Landmarks • To accurately locate the piriformis, identify these bony landmarks: • Superior aspect of the greater trochanter (the insertion) and • The top and bottom of the sacrum and its lateral border. Avoid Sciatic Nerve Palpation The most likely places to palpate the sciatic nerve: • at the greater sciatic foramen • at a point halfway between the ischial tuberosity and the greater trochanter as the nerve passes into the leg. 4 Pain on Palpation Treatment Techniques • Help the client distinguish between muscle pain, and nerve pain. • Our goal is to practice some hands-on therapeutic interventions for piriformis syndrome. • Nerve pain is usually described as: shooting, electrical, hot, numbing, pins and needles, etc. • Soft-tissue work designed to relieve hypertonicity of the gluteal muscles and all of the lateral rotators of the hip will be the most effective treatment. • If palpation elicits nerve pain, move your contact slightly to get away from the sciatic nerve and check to see if the quality of pain changes. Transverse Friction • Transverse friction, popularized by British Orthopedic physician, Dr. James Cyriax. • Transverse friction helps to release nerves entrapped in these tissues. • Can be applied very specifically or more generally across an entire structure. • The key to performing transverse friction well is to palpate the desired structure and then work across the grain of the tissue. • Apply the stroke using a thumb or finger, as if glued to the skin. Transverse Friction: Piriformis • Adding these options to your current repertoire of skills will allow you more flexibility in designing client sessions and increase your likelihood of success in dealing with this condition. Transverse Friction: Piriformis • Because piriformis syndrome is primarily a nerve compression problem, treatment must be aimed at relieving the pressure on the nerve. • Light friction is appropriate as it helps warm the surrounding tissue and stimulate blood flow. • Light friction work along the sacral border and at the insertion point on the greater trochanter is especially effective when the piriformis has been softened up with other techniques. Applying Friction: Piriformis • Mild friction is applied across the grain of the tissue, using thumb, fingers, or knuckles to rub against the lateral border of the sacrum and the superior and posterior trochanter. • Be certain that the friction does not cause any numbness or tingling, since this indicates that you’re frictioning right on the sciatic nerve. Light friction along sacral border. Light friction at the attachments on the greater trochanter. 5 Pin and Stretch Technique • Pin and stretch techniques have become popular in recent years through the work of Michael Leahy, D.C., Stuart Taws, Whitney Lowe, and others. • The basic protocol has the practitioner applying pressure to selected tissues while actively or passively moving the tissues from the shortened position to the lengthened position. • The exact application of the technique varies, depending on which “expert” is teaching it. The rationale for this technique is based on several hypotheses: Pin and Stretch: Piriformis • Client prone, stand at the affected side and ask her to flex her knee to 90 degrees, externally rotate the thigh to bring the lower leg across the midline. • Use your distal hand to lightly grasp the client’s foot and ankle, your proximal hand will apply pressure to the piriformis during the application of this technique. • A loose fist is used for general contact, the thumb is used for Beginning position, more specific contact. loose fist contact. Isolytic Contractions • Discussed at length in “Muscle Energy Techniques” by Leon Chaitow N.D., D.O. • An isotonic eccentric contraction occurs when a muscle is lengthening against resistance. For instance, after performing a biceps curl (a concentric contraction), the biceps is contracting eccentrically as you lower the weight. • Isolytic contractions (specialized isotonic eccentric contractions) are thought to break down adhesions or fibrotic tissue that may have formed within and between layers of tissues. Pin and Stretch: Hypotheses • Maintaining constant contact on the tissue while lengthening it draws the scar tissue/adhesion beneath the contact and helps to release it. • Pressure in the presence of motion helps to reset the autonomic nervous system so the tissue functions more normally. • Working on all the tissues that move the joint during each session will give the best results. Pin and Stretch: Piriformis II • With the leg in the starting position just described, apply pressure to the piriformis with a loose fist and maintain that pressure while you passively rotate the thigh internally, that is, pull the foot and ankle toward you as far as possible. • Release the pressure on the piriformis, return the leg to the starting position, reapply pressure in a different place on the piriformis and repeat. • Systematically work the whole piriformis, then the rest of the lateral rotators of the hip. After the first round using a loose fist is completed, repeat using a flat thumb, for more specific contact. Video clip Maintain moderate pressure as you draw the leg toward you, stretching the piriformis under pressure. Isolytic Contractions II • Isolytic contractions make use of therapeutic levels of resistance to help improve muscle pliability and function. This technique should be pain-free at all times, but may be uncomfortable. • Hypothesis: • Isolytic contractions cause “controlled trauma” to fibrotic tissues. This is followed by a healing process in which the fibrotic tissue is replaced with healthier tissue. 6 Isolytic Contractions: Protocol •The client should be positioned for maximum comfort. • The muscles to be treated should be fully shortened, then the client is asked to resist, but allow, the practitioner’s attempt to lengthen the muscles. •The isolytic contraction lasts 3-5 seconds. In the first round, the client should be working at 15- 20% of maximum and pain-free. •In subsequent rounds (3-4), the client works harder, even up to maximal effort, as long as the therapist can overcome the effort, and the client remains pain-free. Isolytic Contractions: Piriformis • Client prone, stand at the affected side and ask the client to flex his knee to 90 degrees, externally rotate the thigh to bring the leg across the midline as far as possible. • Use your distal hand to lightly grasp the client’s foot and ankle, your proximal hand stabilizes the pelvis. • Client lightly resists as you slowly pull the leg toward you, internally rotating the thigh as far as possible. • In the beginning, the client’s resistance is minimal, then with each subsequent isolytic contraction, the client resists more strongly. video clip Self-Care Piriformis Sequence • Assessment • Warm-up Massage • Pain-free stretching. • Foam Roller. • As symptoms decrease, begin adding pain-free exercise, especially eccentric work for the lateral rotators. • Light Transverse Friction • Pin and Stretch • Isolytic Contractions • “Make Nice” • Re-Assess Further Reading Myofascial Pain and Dysfunction: The Trigger Point Manual Volume 2: Lower Extremities Travell, Janet & Simons, David Williams & Wilkins, Baltimore 1992 Illustrated Manual of Orthopaedic Medicine Cyriax, James & Patricia Butterworths 1985 Muscle Energy Techniques, 2nd edition Chaitow, Leon Churchill Livingstone, Edinburgh 2001 Facilitated Stretching, 3rd edition McAtee, Robert & Charland, Jeff Human Kinetics, Champaign 2007 7