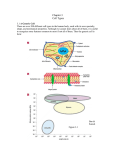
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Mezei_RBC_2017 Mezei_RBC_2017 PATHOPHYSIOLOGY OF RED BLOOD CELLS Zsófia Mezei, MD., 2017. 3./ Hemoglobinopathies a./qualitative alterations: differences in aminoacid composition Gel or crystal formation tendency of hemoglobin sickle cell anemias/drepanocytosis/ HgbS ((226gluval) hemoglobin C disease Hgb C ((226glulis) Unstable hemoglobin: Hereditary Heinz-body anemia Hemoglobin E Hemoglobin easily oxidisable to methemoglobin Methemoglobinemias b./ quantitative: disordered synthesis of complete hemoglobin chains -thalassemias: Thalassemia minor Thalassemia intermedia Thalassemia major/Cooley’s anaemia -thalassemias: Silent carrier Thalassemic characteristics Hemoglobin H (β4) Hemoglobin Barts / hydrops fetalis (γ4) II./ EXTRACORPUSCULAR HEMOLYTIC ANEMIAS: 1./ Immune hemolytic anemias a./ isoimmunisation/alloimmunisation: b./ autoimmune hemolytic anemiák (AIHA): Warm autoimmune hemolytic anemias: Drug-induced AIHA: Type 1: Hapten mechanism Type 2: Immune complex mechanism Type 3: Protein binding to RBC surface Type 4: Autoantibody induction and binding Cold autoimmune hemolytic anemias - primary - secondary Bithermic autoimmune hemolytic anemias - paroxysmal cold hemoglobinuria 2./ Non-immune hemolytic anemias ANEMIAS DEFINITION: GENERAL SIGNS AND SYMPTOMS: Caused by hypoxia and its compensating mechanisms: CLASSIFICATION: A./ INEFFECTIVE ERYTHROPOIESIS/DECREASED RED BLOOD CELL PRODUCTION I./ Normochromic-normocytic anemias: Damaged bone marrow, EPO or cytokine deficiency 1./ APLASTIC OR HYPOPLASTIC ANEMIAS 2./ MYELOPHTHISIS 3./ HYPOPROLIFERATIVE ANEMIAS 4./ PURE RED CELL APLASIA II./ Macrocytic hyperchromic / megaloblastic anemias: Cbl, IF or folate deficiency 1./ PERNICIOUS ANEMIA 2./ OTHER MEGALOBLASTIC ANEMIAS III./ Microcytic, hypo(micro)chromic anemias Disturbed iron metabolism and hem or globin synthesis 1./ IRON DEFICIENCY ANEMIAS 2./ IRON TRANSPORT DEFICIENCY ANEMIAS 3./ IRON UTILIZATION AND REUTILIZATION ANEMIAS a./ SIDEROBLASTIC ANEMIAS Hereditary: DALA synthase disorder Uroporphyrinogen syntase disorder Impaired ferrochelatase Acquired: b./ HEMOGLOBINOPATHIES 4./ ANEMIAS ASSOCIATED WITH CHRONIC DISEASES B./ HEMOLYTIC ANEMIAS / ANEMIAS WITH EXCESSIVE HEMOLYSIS I./ INTRACORPUSCULAR HEMOLYTIC ANEMIAS: 1./ RBC membrane defects Hereditary: a./ Hereditary spherocytosis b./ Hereditary elliptocytosis c./ Hereditaty pyropoikilocytosis d./ Stomatocytosis or hydrocytosis e./ Abetalipoproteinemia (acanthocytosis) Acquired: Paroxysmal nocturnal hemoglobinuria (PNH) 2./ RBC enzyme deficiencies Pentose phosphate pathway -glucose-6-phosphate dehydrogenase Glycolytic pathway (Embden-Meyerhof pathway) - pyruvate kinase Nucleotide metabolism - pyrimidine 5’ nucleotidase 1 C./ ANEMIAS CAUSED BY/FOLLOWING BLOOD LOSS 1./Anemia following to acute blood loss 2./Anemia following to chronic blood loss D./ ABNORMAL DISTRIBUTION OF BLOOD 2 Mezei_RBC_2017 Mezei_RBC_2017 NORMAL VALUES ANEMIAS - 4.5-5.3 x 1012/L = 4.5-5.3 million/L - 4.1-5.1 x 1012/L = 4.1-5.1 million/L HEMATOCRIT / Htk: - 0.37-0.49 L/L - 0.36-0.46 L/L HEMOGLOBIN / Hb: - 8.1-11.2 mmol/L (13.0-18.0 g/dL) - 7.4-9.9 mmol/L (12.0-16.0 g/dL) IRON / Fe: - 5.4-28.7 mol/L TOTAL IRON BINDING CAPACITY /TIBC: - 40.8-76.7 mol/L FERRITIN: Men - 30-300 g/L Women - 10-200 g/L FOLATE: - 7.0-39.7 nmol/L B12: 184 pmol/L RETICOLOCYTE COUNT: 5-15 among 1000 RBCs MEAN CORPOSCULAR HEMOGLOBIN (MCH): - 25-35 pg/cell MEAN CORPOSCULAR HEMOGLOBIN CONCENTRATION (MCHC): - 310-370 g/L MEAN CORPOSCULAR VOLUME (MCV) - 78-102 fL RBC COUNT: Men Women Men Women Men Women 3 4 Mezei_RBC_2017 Mezei_RBC_2017 ERYTHROPOIESIS ERYTHRON: The total mass of circulating RBCs, their precursors and the tisues (bone marrow) that produce them. BONE MARROW: ERYTHROID CELLS: Proerythroblast (E1) Basophilic erythroblast (E2) Polychromatic erythroblast (E3) Polychromatic normoblast (E4) Oxyphilic normoblast (E5) Reticulocyte (contains remnants of nuclei only; stained supravitally) RATIO OF ERYTHROPOIESIS AND GRANULOPOESIS: 1:3 REGULATION IF RBC FORMATION: Erythropoietin (EPO): produed by kidneys; its physiological stimulus is O2 deficiency Cytokines/ growth factors CYCLE OF RBC FORMATION: Proerythroblasts turn to reticulocytes in 5 days /as an effect of EPO in 2 days/ Reticulocytes turn to erythrocytes in 1-2 days Lifespan of RBCs 120 days SUBSTANCES REQUIRED FOR RBC FORMATION: Iron, B6, B12, folate and erythropoietin ERYTHROID CELLS FOUND IN CIRCULATION PHYSIOLOGICALLY: Reticulocyte Erythrocyte- without nucleus 5 6 Mezei_RBC_2017 Mezei_RBC_2017 7 8 Mezei_RBC_2017 Mezei_RBC_2017 MORPHOLOGICAL DIFFERENCES OF RBCs: distorted and shrinked RBC with multiple spiny cytoplasmic projections pyruvate kinase deficiency ANISOCYTE: RBC with different size but normal shape in all anemias ANULOCYTE: Annular(ring)-shaped RBC with decreased MCH hypochromic anemia BASOPHILIC STIPPLING: in increased abnormal erythropoiesis lead poisoning thalassemia DACRYOCYTE: tear-shaped RBC osteomyelofibrosis ELLIPTOCYTE: egg-shaped RBC hereditary elliptocytosis FRAGMENTOCYTE/SCHISTOCYTE: split / RBC fragment HUS, TTP, heart valve implant HEINZ BODY: denatured hemoglobin G-6-PD deficiency methemoglobinemia HOWELL-JOLLY BODY: nuclear remnants asplenia MACROCYTE: large RBC but normal in size hyperchromic anemia MEGALOCYTE: large and egg-shaped RBC hyperchromic anemia MICROCYTE: small RBC but normal in size hypochromic anemia NORMOCYTE: RBC with diameter 7-8 m; doughnut-shaped with light center POIKILOCYTOSIS: RBCs showing abnormal variations in shape in severe anemias SICKLE CELL: lunular RBC (sicle shaped) due to abnormal Hgb sickle cell anemia SPHEROCYTE: spheric form small RBC lacking central pallor spherocytosis without light center TARGET CELL: RBCs with bullseye appearance thalassemias ACANTHOCYTE: 9 10 Mezei_RBC_2017 Mezei_RBC_2017 ANEMIAS CLASSIFICATION: DEFINITION: Anemia is a condition where the oxygen-carrying capacity of RBCs is impaired. This might be induced by: - decreased absolute RBC count - reduced hemoglobin content, corresponding to age and sex - abnormal hemoglobin A./ I./ Normochromic-normocytic anemias: GENERAL SIGNS AND SYMPTOMS: Caused by hypoxia and its compensating mechanisms: Nervous system: headache, tinnitus, vertigo, syncope, insomnia, concentration difficulty and impaired vision Urinary system: microscopic hematuria, mild proteinuria, salt and water retention and elevated erythropoietin synthesis Circulatory system: tachycardia and angina Respiratory system: hyperventilation Discoloration of skin and visible mucous membranes: Depending on type of anemia: - white: iron deficiency anemia - yellow: hemolytic anemia - gray: tumor anemia Skin appendages: - hair: split ends and hair loss - nail: INEFFECTIVE ERYTHROPOIESIS/CONDITIONS WITH DECREASED RED BLOOD CELL PRODUCTION cracked, koilonychias (spoon nails) 11 Definition: Reduced RBC count and oxygen carrying capacity of RBCs without morphologic and staining abnormalities Normocytic: normal Mean corpuscular volume / MCV Normochromic: normal normal Mean corpuscular hemoglobin / MCH Mean corpuscular hemoglobin concentration/MCHC Types: 1./ APLASTIC OR HYPOPLASTIC ANEMIAS Definition: Anemia that results from a loss of hematopoietic stem cell population and decrease of early blood cell precursor count EPO level is normal or increased Aplastic anemia is part of pancytopenia caused by hypoplasia of bone marrow. Causes 1./ unknown – 50-65 % of cases are idiopathic 2./ known a./ hereditary: chromosomal abnormlaity b./ acquired: radiation chemicals - benzene drugs: side effect: dose-dependent manner idiosyncratic effect - unexpected - dose-independent autoimmune mechanisms infections: hepatitis, HIV, Epstein-Barr virus hypersplenia Clinical signs and symptoms: 1./peripheral blood smear: a./ anemia: normocytic, normochromic (due to ↓ RBC production of bone marrow) ↓ reticulocyte count therapy (Fe, folate, B12) resistant general signs and symptoms of anemia b./ neutropenia: leukopenia (↓ leukocyte count) - infections and sepsis c./ thrombocytopenia (↓ PLT count) - hemorrhages 2./ empty bone marrow (bone marrow poor in cells) site of hematopoiesis is replaced by lipids 12 Mezei_RBC_2017 Mezei_RBC_2017 2./ MYELOPHTHISIS Definition: Infiltration and replacement of normal hematopoietic cells by ’non-hematopoietic’ cells EPO level is normal or increased Cause: Infiltration of bone marrow by: a./ connective tissue b./ lipid c./ tumor cells Clnical signs and symptoms: General signs and symptoms of anemia Signs and symptoms of underlying disease Hepatosplenomegaly (extramedullar hematopoiesis/due to myeloid metaplasia) Peripheral blood smear: RBC: normocytic anemia (but ocasionally size and morphologic differences occur, which shortens lifespan of RBCs and in this case reticulocytosis occurs) in case of extramedullar RBC formation nucleated red blood cells might appear in the circulation WBC: normal, ↓ or PLT: the count is often low, giant, bizarre shape cells might occur 3./ HYPOPROLIFERATIVE ANEMIAS Definition: absent or deficient EPO or diminished response to EPO and/or cytokines Cause: Renal diseases: amyloidosis, diabetes nephropathy and uremia Decreased metabolism: hypothyroidism and hypopituitarism Conditions with protein loss Clinical signs and symptoms: peripheral blood smear: normocytic, normochromic RBCs reticulocytopenia general signs and symptoms of anemia signs and symptoms of underlying disease 4./ PURE RED CELL APLASIA Definition: Selective destruction of erythroid precursors EPO level is normal or increased Cause: viral infection, immune processes, drugs and toxins Clinical signs and symptoms: usually mild, depending on degree of underlying disease and anemia variable cellularity of bone marrow 13 14 Mezei_RBC_2017 Mezei_RBC_2017 II./ Macrocytic hyperchromic or megaloblastic anemias: Definition: Reduced RBC count and oxygen carrying capacity. Large ( MCV) and strong staining (MCH, MCHC) Cells are found in circulation and bone marrow as well Cause: Vitamin B12 deficiency or inadequate utilization Folate deficiency or inadequate utilization VITAMIN B12: PHYSIOLOGY Cobalamin (Cbl) is essential, found in animal products only Way of absorption: Cbl from food, bound to protein, is dissociated from food protein by gastric hydrochloric acid and pepsin Cbl binds to R protein found in saliva and gastric juice and transported to duodenum, where B12 is dissociated from R protein by pancreatic digestive enzymes and binds to intrinsic factor (IF) produced by gastric parietal cells The complex is absorbed via attachment to special receptors located in the ileum Cbl in circulation: bound to transcobalamin I (blood) storage bound to transcobalamin II transported with blood to receptors of consuming and storage organs bound to transcobalamin III reach liver, bile and intestine and defecated DEFICIENCY OR INADEQUATE UTILIZATION OF VITAMIN B12 : A./ Decreased B12 uptake: vegetarians B./ Vitamin B12 malabsorption: 1./ Disorders of IF metabolism: a./Decrease of IF synthesis: Hereditary: - inability to synthetise IF or - IF is functionally inadequate Acquired: - gastrectomy or - injury of gastric parietal cells cell mediated autoimmune process or caused by auto antibodies produced against microsomal fraction of gastric mucosal cells consequence: atrophic gastritis histamine refractory achylia gastrica (HCl production cannot be stimulated by histamine) - ↑ risk for stomach cancer b./impaired B12 binding capacity of IF- due to blocking Ab c./impaired binding of IF-B12 complex to ileal receptors because this is inhibited by autoAb against the complex 2./ pancreatic gland disorders 3./ disorders of ileum: inflammation, surgiacl resection 4./ increased B12 consumption: vermis and bacteria consume B12 5./ Drugs: p-amynosalicylic acid, colchicine, neomycin C./ Transcobalamin II deficiency protein synthesis – liver diseases protein loss - nephrosis D./ Increased need: pregnancy, following to blood loss Aim: Technique: SCHILLING TEST This test is used to determine whether Se B12 deficiency is caused by: malabsorption or IF deficiency Schilling I. - B12 storages of the patinet has to be filled by parenterally administered B12 (1000 g) - Then (after 1 hour and within 6 hours following to administration) radioactive B12 is given orally to the patient - 24-hour urine collection - Amount of voided isotope is determined from the 24-hour collected urine: normally ≥ 9 % ; if the result < 5 % decreased B12 absorption is determined when renal function is normal Schilling II. - B12 storages of the patinet has to be filled by parenterally administered B12 (1000 g) - Then (1-6 h following to administration) radioactive B12 +IF is given orally to the patient - 24-hour urine collection - The amount of voided isotope is determined in rate (in percentage) of transported activity If amount of voided B12 isotope normalizedIF deficiency is the cause If the voided B12 isotope remains abnormal, malabsorption is the cause 15 16 Mezei_RBC_2017 Mezei_RBC_2017 FOLATE PHYSIOLOGY OF FOLATE Synthetised in plants and damaged by cooking Transports C1 portions (methyl and formyl group) and has an importan role in synthesis of homocysteine methyonine DNA DEFICIENCY OR UTILIZTAION DISORDER RFOLATE A./ Insufficient uptake: alcoholists, adolsecents and children B./ Malabsorption: in inflammatory bowel diseases drugs (phenytoine, barbiturate, ethanol) C./ Disorders of metabolism: dihydrofolate reductase inhibitors (methotrexate, trimethoprim), alcohol, enzyme defects D./ Cytotoxic substances: interfere with DNA ynthesis (purine, pyrimidine or folate antagonists, antimetabolites, alkyling agents) E./ Increased need: pregnancy, children Tumors hematopoiesis Types: 1./ Pernicious anemia /Biermer’s anemia/ macrocytic anemia caused by autoimmune processes 2./ Pernicious like anemia / other macrocytic anemia caused by B12 and folate deficiency Pathomechanism: Methylcobalamin (MeCbl) deficiency Cause impaired DNA synthesis, thus -maturation of nucleus is slow and cell cycle is prolonged (lifespan of cells increase) RNS synthesis continues, thus - cytoplasma increases; i.e. megaloblastic hematopoiesis occurs - RBC precursors are megaloblastic - RBCs are vulnerable - cell lysis→ Se ncBi and urea Affect all (currently dividing) cell lines, thus leukopenia, large WBC with hypersegmented nucleus (over-matureated) and thrombocytopenia might occur as well Impaired methionine synthesis -decreased methionine synthase activity -decreased methionine level might be responsible for nervous sytem symptoms Adenosylcobalamin (AdoCbl) deficiency Disordered myelin synthesis and repair occurs. Accumulated propionyl-CoA damages myelin sheath This cause degenaretive processes in: Cerebral white matter Peripheral nerves Posterior and lateral horn of spinal cord Optic nerves 17 18 Mezei_RBC_2017 Mezei_RBC_2017 Clinical signs and symptoms: Peripheral blood smear: RBC: macrocytic hyperchromic - large size MCV 100 fl - strong staining MCH35pg/sejt, MCHC370g/l ovalocytosis – egg-shaped cells anisocytosis – exceedingly variable RBC diameters widened Price-Jones curve and shifted to the right Poikilocytosis – variable RBC shape osmotic resistance of RBCs – hemolysis reticulocyte count WBC: hypersegmented (showing more than 5 nuclear lobes) Leukopenia PLT: thrombocytopenia Bone marrow: (MPO=myeloperoxidase) Hypercellular bone marrow Megaloblastic erythropoiesis Erythroid hyperplasia (high RBC precursor count) myeloid/erythroid (norm. WBC/RBC: 3:1) ratio Gastrointestinal signs Hunter’s glossitis: red and painful toung with atrophic papillae Histamine refractory achylia gastrica – perdispose to gastric cc Narvous system: Presented in vitamin B12 deficiency only (folate deficiency cause nervous system injury in fetus only): Polyneuropathy Disorders of peripheral sensing: Disturbed: - touching sensation - heat sensation, Memory disorder Depression Funicular myelosis, degenaration of myelin sheath: 1./ Posterior fascuculi of spinal cord - spinal ataxia - cause wide-based gait 2./ Corticospinal tract spastic paresis and corticospinal signs 19 20 Mezei_RBC_2017 Mezei_RBC_2017 III./ Microcytic, hypo(micro)chromic anemias Definition: Reduced RBC count and oxygen carrying capacity Small/MCV and poorly staining/MCH, MCHC RBCs are presented in circulation Types: 1./ IRON DEFICIENCY ANEMIA Definition: ineffective erythropoiesis caused by iron deficiency IRON Need: PHYSIOLOGY 1 mg/day (adult men) Absorption: Absorbed in duodenum and in proximal jejunum. Heme iron is absorbed in a better way than nonheme iron. Absorption of non-heme iron is assisted by: gastric hydrocholic acid, ascorbic acid Iron is absorbed via acative transport. If transferrin saturated, iron absorption ceases and the non-absorbed unrequired iron leaves the body via the faces. Apoferritin synthetised in mucosal cells takes up iron. From ferritin iron gets to the carrier plasma protein transferrin. Transferrin is a beta-globulin synthethised by the liver. Iron distribution: Only small amount of ferritin is found in serum. There is a close relation between Se ferritin and iron storage of the body. Low Se ferritin - A sign of iron deficiency in all cases High Se ferritin concentration is not always caused by the increased iron storages. Inflammation can induce high ferritin level as well, because ferritin is an acute phase protein. Hemosiderin is a degraded storage form of ferritn, difficult to use for hematopoiesis. Primarily iron is stored in mononuclear phagocytic cells (machrophages) of spleen, liver and bone marrow. Iron released during cell lysis is reused in hematopoiesis. Iron reuse covers 97% of daily iron need. 21 22 Mezei_RBC_2017 Mezei_RBC_2017 CAUSES OF IRON DEFICIENCY: Usually caused my multiple factors simultaneously Insufficient intake: not enoug or not the adequate form (ferri or ferro) Malabsorption (impaired absorption): 1./ Decreased hydrochloric acid production 2./ Increased bowel motility 3./ Transport disorders Hereditary Acquaired Increased loss: occult hemorrhage (GI hemorrhage, menstrual) chronic intravascular hemolysis: iron deficiency occur due to hemoglobinuria and hemosiderinuria Increased need pregnancy, growth Development of iron deficiency anemia: Stage 1/ Pre-latent: Decreased iron storage Normal: Se Hb and iron Decreased: Se ferritin < 20 ng/mL Increased: transferrin concentration (↑ TIBC/total iron binding capacity refers to this) Stage 2/ Latent: Empty iron storage Cannot guarantee iron neded to erythroid bone marrow Decreased: Se iron Increased: Se transferrin Se ferritin receptor concentration increases >8.5 mg/L Stage 3/ Manifest: Microcytic hypochromic anemia 23 24 Mezei_RBC_2017 Mezei_RBC_2017 Clinical signs and symptoms: General signs and symptoms of anemia Koilonychia: concave, cracked and dry nails Angular cheilosis: fissure and ulcer of labial comissure Plummer-Vinson syndrome: iron deficiency anemia dysphagia glossitis Peripheral blood smear: RBC microcytic: small diameter of RBC ( MCV) anisocytosis: varable RBC diameters widened Price-Jones curve and shifted to the left hypochromic: poorly staining RBCs (MCH, MCHC) planocytes: thin RBCs anulocytes: ring-shaped RBCs decreased reticulocyte count Bone marrow: Serum: Numerous young RBCs (normoblasts) iron ferritin (↓ RBC ferritin as well) TIBC (total iron binding capacity) transferrin saturation 2./ IRON-TRANSPORT DEFICIENCY ANEMIAS Koilonychia Definition: Iron from storages cannot reach site of erythropoiesis. Glossitis Cause: transferrin deficeinecy: - synthesis (e.g. liver diseases) - loss (e.g. nephrosis) defective transferrin molecule Angular cheilosis Dysphagia 25 26 Mezei_RBC_2017 Mezei_RBC_2017 3./ IRON UTILIZATION AND REUTILIZATION ANEMIAS Definition: Inadequate or abnormal intracellular iron utilization for hemoglobin synthesis, in spite of the fact that amount of iron is sufficient or increased in mitochondria of erythroid precuror cells. Types: a./ SIDEROBLASTIC ANEMIAS Definition: Impaired formation of hem porfirin structure Thus iron cannot be built into the structure of heme. Cause: Hereditary: Disorders of enzymes required for heme prophyrin synthesis: DALA synthase defect uroporphyrinogen synthase defect ferrochelatase defect Acquired: Vitamin B6 deficiency (DALA cofactor) Intoxication: - lead, inhibits heme synthesis - antituberculotics and alcohol disturb pyridoxine metabolism or formation of active pyridoxine-5-phoshate from pyridoxine - chloramphenicol and chemotherapeutic agents Associated with neoplastic and inflammatory diseases (cc, leukemia and RA) Clinical signs and symptoms: Peripheral blood smear: RBC: microcytic, Price-Jones curve widened, shifted to the left Siderocytes: iron granules in RBC cytoplasm elevated: Se iron, ferritin, Transferrin saturation decreased: TIBC (total iron binding capacity) Bone marrow: hypercellular ringed sideroblasts The ring is fromed by mitochondrial iron deposits, as there is the initial and last step of heme synthesis intramedullary death of RBCs b./ HEMOGLOBINOPATHIES thalassemias (see hemolytic anemias) microcytic, hypochromic anemia but elevated Se iron and ferritin decreased Se transferrin (i.e. there is a large quantity of iron storages) 27 Bone marrow 28 Mezei_RBC_2017 Mezei_RBC_2017 4./ ANEMIAS ASSOCIATED WITH CHRONIC DISEASES Cause: acute and chronic inflammation (virus, bacteria, parasites, fungi) tumor (hematological, solid tu) autoimmune diseases (RA, SLE and vasculitis) chronic renal disease and nephritis Pathomechanism: a./ Impaired iron metabolism (defective iron reutilization): Cytokines are released from activated T-cells and monocytes by pathogens: INF, TNF, IL-1, IL-6, IL-10 Cytokines iron uptake and store of RES cells, due to: of ferritin synthesis thus iron storage of RES erythrophagocytosis DMT1 expression of macrophages, and thus iron uptake of a macrophages transferrin-mediated uptake of iron by macrophages ferropontin expression of macrophages and thus iron export of macrophages hepcidin expression and thus iron export of macrophages and duodenal iron absorption b./ Impaired erythropoies because cytokines - inhibit proliferation and differentiation of RBC precurors - EPO production and acativity - EPO receptor expression in progenitor cells - ROS activity, direct cytotoxic to progenitor cells and EPO producing cells Clinical signs and symptoms: symptoms of underlying diseases (infection, inflammation, tu) Moderate microcytic anemia Se iron decreased Se ferritin and RBC ferritin normal Anemia associated with chronic diseases Iron Transferrin Transferrin saturation Ferritin Solubile transferrin receptor - normal normal - normal Cytokine level Iron deficiency anemia normal 29 30 Mezei_RBC_2017 Mezei_RBC_2017 C./ HEMOLYTIC ANEMIAS / ANEMIAS WITH EXCESSIVE HEMOLYSIS SITE OF HEMOLYSIS: DEFINITION:: Decreased RBC count and oxygen carrying capacity despite effective erythropoiesis, as lifespan of RBCs are decreased HEMOLYISIS:: Iron, LDH1, Potassium and Hgb released from RBCs: Iron bound to apotransferrin - Se iron LDH1 - Se LDH1 Potassium - Se K Hgb bound to haptoglobin - ↓ Se haptoglobin One part of free hemoglobin that remained in plasma is excreted by kidneys - hemoglobinuria Other part is transformed to hematin and bound to hemopexin (only after haptoglobin is saturated) - Se hemopexin Carried to RES by hemopexin In RES biliverdin and then bilirubin is formed and gets to plasma - Se ncBi. Nonconjugated Bi (ncBi) is carried by albumin to the liver, where that is conjugated (cBi) by glucuronate and becomes water soluble cBi reaches the bowels, where Ubg is formed; one part of Ubg is reabsorbed in the circulation One part of Ubg that reached circulation gets back to liver and other part is voided - urinary Ubg The unabsorbed Ubg is transformed to stercobilin in bowels, this determines color of faces - pleiochromic faces 31 RED BLOOD CELL MEMBRANE 32 Mezei_RBC_2017 Mezei_RBC_2017 CAUSES AND TYPES OF HEMOLYTIC ANEMIAS I. INTRACORPUSCULAR HEMOLYTIC ANEMIAS: 1./ RBC membrane defects # HEREDITARY a./ Hereditary spherocytosis Definition: hereditary RBC membrane defect Cause: abnormal RBC cytoskeleton caused by a genetic disorder autosomal recessive: ↓ binding ability of spectrin to 4.1protein and actin autosomal dominant: unstable ankyrin that leads to ↓ incorporation of spectrin to membrane Pathomechanism: Cytoskeletal defect cause: ion permeability of RBC membrane, thus ic. Na+ and water that leads to development of spherocyte (ball-shaped RBC) Deformed RBCs are - filtered by spleen and - lifespan of RBCs ↓ because continuous shape changes use up much energy Clinical signs and symptoms: Most of the patients suffer from a lifelong but moderate normochromic anemia Cahnges in hemoglobin level RBC: Spherocyte (ball-shaped), these red cells lack central pallor Their osmotic resistance 33 Normal osmotic resistance Decreased ozmotic resistance Signs of hemolysis with intermittent and variable jaundice and splenomegaly Gall stones Congenital disorders: polydactylia, gothic palate b./ Hereditary elliptocytosis Definition: >20 % of circulating RBC are elliptocytes Forms/Types: - general form: numerous elliptocytes with mild hemolysis - spherotic form: spherocytes and elliptocytes with moderate anemia - stomatocytic form: accompanied with RBC antigen alteration that is protective against malaria Pathomechanism: - abnormal spectrin chain leads to impaired spectrin dimer-dimer interaction - in spherocytic form amount of 4.1 protein is decreased - impaired ankyrin-anion transporter bound Clinical signs and symptoms: asymptomatic or well compensated normal osmotic resistance 34 Mezei_RBC_2017 Mezei_RBC_2017 c./ Hereditary pyropoikilocytosis: Definition: thermosensitive RBCs Pathomechanism: impaired spectrin dimer-dimer interaction caused by abnormal spectrin chain Clinical signs and symptms: RBC: fragments, microspherocytes Hairy cells, decreased MCV Mild hemolytic anemia e./ Acanthocytosis Abetalipoproteinemia Cause: Genetic disorder, recessive apo B-48 and 100 deficiency Pathomechanism impaired transport of TG to blood Clinical signs and symptoms: Decreased lipid absorption: Steatorrhoea Decreased Se chylomicron (postprandial lipidaemia cannot be detected) Se total lipid Se VLDL (not produced) Acanthocytes in peripheral blood smear: dark and shrinked RBCs with collapsed and irregular cavity and wide spike projections this is accompanied with relatively high sphingomyelin content of RBC membrane; this makes the cell rigid severe hemolytic anemia ataxic neuropathy retinitis pigmentosa mental retardation d./ Stomatocytosis o hydrocytosis Pathomechanism: Exact structural defect is unknown. Increased membrane permeability to Na ions and K ions as well Na+ carries water, cells become swollen and susceptible to osmotic and mechanic lysis Clinical signs and symptoms: Erythroid hyperplasia and thus mild anemia. RBC: stomatocytes: fish mouth-like pallor in the middle of cells uniconcave cells, increased MCV, hemolysis 35 36 Mezei_RBC_2017 Mezei_RBC_2017 II. INTRACORPUSCULAR HEMOLYTIC ANEMIAS: 1./ RBC membrane defect # HEREDITARY # ACQUIRED Paroxysmal nocturnal hemoglobinuria (PNH): Definition: Acquired clonal disorder of hemopoietic stem cell Cause: X-linked somatic mutation of phosphatidylinositol glycan–A (PIG-A) gene in hematopoietic stem cells Pathomechanism: First step: X-linked somatic mutation of phosphatidylinositol glycan– A (PIG-A) gene in stem cells and thus glycosylphosphatidyl inositol (GPI) anchor protein becomes impaired on hemopoietic stem cell surface Second step: Immunological selection of hemopoietic stem cells with deficient GPI anchor The selection is initiated by suppressive cytokines (i.e.transforming growth factor β - TGF-β) that diminish hematopoiesis. These abnormal cells survive and proliferate Increased proliferation increase the chance of further genetic mutations Third step: Abnormal GPI anchor appear in phenotype (in all circulating cells) RBCs are more sensitive to lytic effect of complement because abnormal GPI anchor cannot bind: complement regulatory proteins: - DAF (CD55 /decay-accelerating factor/) that accelerate C3 convertase degradation - MIRL (CD59 /membrane inhibitor of reactive lysis) that prevent C9 polymerisation and sinking into membrane This protein is found on PLTs as well. Activated complement might cause platelet aggregation and hypercoagulabilty; i.e. thrombosis. Increased cell lysis might cause an elevation in Se TF level, which might cause increased platelet aggregation and hypercoagulability 37 38 Mezei_RBC_2017 Mezei_RBC_2017 Clinical signs and symptoms: chronic intravascular hemolyis with acute attacks (causes: infection, stress, drugs, sleeping, ↓ pH) hemoglobinuria, hemosiderinuria, splenomegaly venous thrombosis: - in intraabdominal veins: (in portal and mesenterial veins and in hepatic vein) that cause splanomegaly and abdominal pain - Thrombi in cerebral veins might cause death of the patient Prognosis: aregenerative crisis infection embolisation uremia death within 10 years from set up of diagnosis Peripheral blood smear: Normocytic normochromic anemia granulocytopenia thrombocytopenia Bone marrow: hypercellular in early phase hypocellular in a later phase PCV/Packed Cell Volume/HCT/Hematocrit 39 2./ RBC enzyme deficiencies # CONGENITAL Pentose phosphate pathway glucose-6-phosphate dehydrogenase (G6PD)=Fabism Cause: G6PD gene on chromosome X Patients: male and homozygous female Altering signs and symptoms: heterozygous female (resistance against malaria) Pathomechanism: G-6-PD deficiency G6PD catalyzes NADP+NADPH+ formation NADPH is a cofactor of glutathione reductase ↓ amount of reduced glutathione glutathione is protective against oxidative stress ↓ RBC protection against oxidativesterss Oxidative stress might be induced by: drugs: antimalarial sulphonamides sulphones analgetics nitrofurans vitamin K derivatives Fava bean: Contains reductive compounds (isouracil and divicin), hydrogen peroxide is formed by them The following parts might be oxidized: Heme iron: Methemoglobin is formed, inadequate for O2 transport Globin: Heinz-bodies are formed, these are products from oxidative degeneration of Hgb, which are bound to the membrane RBCs that contain Heinz-bodies are rigid and detected and destructed by RES - ↑ cation permeability of membrane, thus cause hydrated and deformed RBCs Membrane proteins: e.g. spectrin, this leads to decreased RBC deformation Lipids: cause acute iv. haemolysis 40 Mezei_RBC_2017 Mezei_RBC_2017 Clinical signs and symptoms: Induce: oxidants high body temperature Acute viral and bacterial infection Diabetic acidosis General signs and symptoms of hemolytic anemia: Hemolysis (jaundice) Enhanced erythropoiesis (Reticulocytosis) Anemia RBC: Heinz-bodies Bite cells (caused by removal of Heinzbodies by spleen) Complication: hemoglobinuria Acute renal failure Acute hemolysis in G6PD deficiency „bite” cell or keratocyte (arrow) two „blister cells” (arrow), polychromatic macrocytes and irregularly contracted cell (arrowhead) 41 42 Mezei_RBC_2017 Mezei_RBC_2017 Glycolytic pathway (Embden-Meyerhof pathway) Pyruvate kinase (PK) Cause: AR enzyme deficiency Pathomechanism: Physiological role of PK: pyruvate synthesis with ATP formation, which ir required for - K+-Na+ pump Ca++ pump of RBC membrane - maintenance of deformation Signs and symptoms: Hemolysis - in homozygous only - in heterozygous not Splenomegaly RBC: normocytic Akantocytes (contracted spiky RBCs) Aplastic crisis might occur (e.g. in parvovirus infection) Nucleotide metabolism Pyrimidine 5’ nucleotidase Cause: AR, Manifest in homozygous-hemolytic anemia Pathomechanism: Due to enzyme deficiency: There is no RNA degradation of reticulocytes, 5x increase of RBC nucleotide pool: ↑ pyrimidine and ↓ adenosine nucleotide undegraded ribosomes accumulate and aggragate Signs and symptoms: hemolysis, basophilic stippling in mature RBCs, splenomegaly Pyruvate kinase deficiency after splenectomy 43 44 Mezei_RBC_2017 Mezei_RBC_2017 PHYSIOLOGY OF GLOBIN SYNTHESIS: Chromosome 16 (α, ζ) and 11 (β, δ, ε, γ) are responsible for synthesis of globin chains. Formation site and type of globin chain changes periodically. 3./ Hemoglobinopathies a./qualitative alterations: Differences in aminoacid structure A./ Gel or crystal formation tendency of hemoglobin 1./ SICKLE CELL ANEMIAS / DREPANOCYTOSIS Cause: Point mutation of chromosome 11 Hgb S is formed: Hgb S ((226gluval), site of glutamate is occupied by valin in chain Heterozygous - RBCs 50% Hgb S Homozygous - RBCs 70–98% Hgb S (other F) Pathomechanism: Hemoglobin consists of 4 globin chains. Cromosome 16 is responsible for formation of 2 alpha chains and chromosome 11 is responsible for formation of other 2 beta chains. Solubility of oxy-Hgb S is normal Solubility of reduced-Hgb S is decreased, thus these precipitate When size of the aggregate reaches a critical level, explosive gel formation starts, because the aggregate acts as a core and tube-like fibers are formed by adhesion of core and reducedHgbS-teramers. This cause formation of sickle cells, i.e. menisocytosis gel fromation is: enhanced by: - hypoxia - pH ↓ stability of reduced-HgbS - 2,3-DPG stability of reduced-HgbS -increased redued-HgbS cc ( 16 g/dl) - mechanical effects; e.g. shearing stress - RBC dehydration ( MCHC) - deceleration of speed (because a given time is required for gel formation) suppressed by: - increase in amount of HgbF - increase in amount of HgbA 45 46 Mezei_RBC_2017 Mezei_RBC_2017 Signs and symptom: Chr. hemolysis Blood Characteristics of sickle cells: Principal Mechanisms responsible for potassium and water loss in sickle red cells Defect in membrane salt and water transport: 1./ Na+-K+-ATPase is activated 2./ K+-Cl- cotransporter is activated 3./ Gárdos-type K+ channel is activated RBC is dehydrated of MCHC is increasing the polymerisation that cause irreversible sickling (sickle form remains after reoxygenisation) Spontaneous Heinz-body formation Membrane protein (glycophorin and ankyrin) precipitation IgG, IgA, IgM and complemts factors are attached to them Macrophages are activated RES detects (and filters) affected RBCs iv. hemolysis occurs that might cause anemia - anemia Heinz-bodies Howell-Jolly-bodies (nuclear chromatin remnants in cytoplasm, spleen is unable to filter them) Sickle cell in Na-metabisulphite preparation Jaundice Bone marrow: - erythroid hyperplasia Symptoms due to vascular occlusion Splenic vein thrombosis -hyposplenia Pain -muscle, bone, abdominal Ulcus cruris Liver: Congestive hepatopathy -caused by heart failure Hepatitis -caused by frequent transfusions Hepatic lesions -caused by hepatic sinusoidal occlusion -caused by overburdened Kupffer cells Sudden hepatomegaly -caused by sequestration Cholelitiasis Respiratory: Pulmonal embolisation Lung infarction Urogenital: urine concentration ability Hematuria Papillary necrosis decreased GFR RTA Priapism and impotence Ophthalmic: Retinopathy Hyaloid hemorrhage Neurologic: Thrombosis Ischemic cerebral events Acute attacks Acute life-theratening events Hemolytic crisis Elicited by: -infection, cold, Hgb level, ↓ pH Signs:-pain, portal and renal vessel occlusion Aplastic crisis Elicited by -Parvovirus infection Signs -rapidly decreasing Hgb, Htk, Reticulocyte 47 48 Mezei_RBC_2017 Mezei_RBC_2017 2./ HEMOGLOBIN-C DISEASE Cause: Gene defect caused by point mutation, Hgb C ((226glulis) is produced glu = glutamate, lys = lysine Glutamate is replaced with lysine in -chain Pathomechanism: HgbC- interacts with K+-Cl- transporter - its activity remain in mature RBCs - K+ is lost by RBC and RBC is dehydrated, MCHC is increased oxyHgbC is aggregated and crystallized but dissolved during deoxygenisation and do not cause occlusion Signs: RBC membrane becomes rigid by HgbC: Fragmentocytes, Microspherocytes, Target cells might be formed (80 % of RBCs) Homozygous: mild hemolysis, compensated splenomegaly -moderate Heterozygous: asymptomatic Hemoglobin C crystals are hexagonally shaped rods that occur in the red cell cytoplasm of patients with homozygous hemoglobin C. These crystals may also be extracellular 49 50 Mezei_RBC_2017 Mezei_RBC_2017 B./ Unstable hemoglobin 1./ HEREDITARY HEINZ-BODY ANEMIAS Definition: Aminoacid change caused by a point mutation that results in unstable hemoglobin molecule. There are numerous individual variants Pathomechanism:Effects of aminoacid change: Heme group of hemoglobin molecule is lost, - Configuration of heme binding site is changed, - Bounds between and chains are weaken or - Structure of subunit is weaken Consequences: In oxydative stress Hgb molecule is broken up and precipitates Heinz-bodies are formed They are precipitated, denaturated hemoglobin due to oxidative injury. They are usually eccentrically placed and attach to the membrane. (They are may be seen in G6PD, α thalassemia, unstable hemoglobins and in splenectomised patients also.) RBC membrane becomes defected RES detects/filters Hemolysis Signs: Chr. and partially compensated hemolysis Splenomegaly 51 2./ HEMOGLOBIN E Definition: ponit mutation, gene defect, unstable Hgb molecule is formed, Glutamate is replaced by lysisn in position 26 of Hgb 2 226GluLys Pathomechanism: Mutation occurs in 1-1 bound and thus the oxydative stress makes the molecule unstable Signs: Heterozygous: Normal Hgb, Microcytosis, No splenomegaly Electrophoresis: 70% Hgb A, 25% E, 5% A2 or F Homozygous: Mild anemia, Low MCV, microcytosis, Traget cell, No reticulocytosis, chr. hemolysis Electrophoresis: Hgb E only C./ Hemoglobin easily oxidisable to methemoglobin METHEMOGLOBINEMIAS: Definition: Methemoglobin is an oxidation product of hemoglobin that contains ferri iron Ferri ion containing heme of methemoglobin is unable to bind oxygen. Ferro heme in hemoglobin tetramer is unable to carry oxygen either, because its oxygen binding capacity is increased and cannot deliver oxygen (oxygen dissociation curve is shifted to the left). Normally rate of methemoglobin is 0.5 %, which is reduced by NADH-cytochrom-b5 reductase Types: Hereditary: a./ Hemoglobinopathy -Haemoglobin M Pathomechanism: Genetically defected and chains. Histidine, which has a role in formation of iron binding, is replaced by tyrosine. Stable bound is formed between heme iron and aminoacid side chain, thus inability of oxygen binding and resistance cytochrome-b5 reductase. Signs: cyanosis minimal hemolysis when compensated might be symptomatic due to: - polycythemia and - increased 2,3 DPG level b./ Cytochrome-b5 reductase deficiency or defect Aquired - oxidants: Causes: Exogenous: nitrite, nitrate pollution Endogenous: bacteria (enteritis, sepsis) Signs:Children: nervous system defects Occur when there is 40 % methemoglobin 50 %: cyanosis, hypoxia; 70-80 %: life-threatening 52 Mezei_RBC_2017 Mezei_RBC_2017 b./quantitative alterations: disorders of entire globin chain synthesis THALASSEMIAS Definition A genetic defect that cause imbalance between synthesis of the globin chains Pathomechanism: The unpaired chains are accumulated in erythropoietic stem cells and are toxic causing ineffective erythropoiesis. Types: THALASSEMIA Definition: Genetic defect of globin chain synthesis is located in chromosome 11 Cause: Defected perparation of mRNS-transcript in nucleus - Early termination of translation - Gene deletion Pathomechanism: In adults chain can be replaced by and chain Thus in -thalassemia the amount of: Hgb A2 ( 22) and Hgb F ( 22) increase Excessive unpaired chains aggregate and precipitate that leads to: decreased ATP synthesis potassium leakage decreased sialic acid content of membrane IgGs against blood group antigens are produced and macrophages bind them - rigid and deformed RBCs Ca++ transport defect occur, thus ic Ca++ level incerases chain aggregates are bound to membrane cytoskeleton and cause: apoptosis of erythropoietic stem cells in bone marrow and rigidity and instability of RBCs, K+-Cl- cotransporter becomes defected, thus RBCs become dehydrated 53 Clinical menifestations: 1./ -thalassaemia minor: heterozygous mild anemia, or anemia is not presented peripheral blood: RBC –microcytic, hypochromic, basophilic stippling splenomegaly (rare) 2./ -thalassemia intermedia: various genetic background moderately severe definite anemia hepatosplenomegaly 3./ -thalassemia major (Cooley’s anemia): homozygoous severe hemolytic anemia jaundice, hepatosplenomegaly impaired growth increased susceptibility to infections peripheral blood smear: nucleated RBCs basophilic stippling (rRNS aggregates) chain aggregates 54 Mezei_RBC_2017 Mezei_RBC_2017 THALASSEMIA Definition: Genetic defect of globin chain synthesis is located in chromosome 16 Cause: gene translocation, point mutation Clinical manifestations: 1./ Silent carrier syndrome:Genotype: / One α gene is absent 2./ Thalassememic nature: 2 genes are absent either homozygous or heterozygous Homozygous -thalassemia: genotype: -/- Heterozygous -thalassemia: genotype: --/ Normal HgbA2 level anemia is presented or not, hypochromic, microcytic RBCs 3./ Hemoglobin-H disease 3 genes are absent; genotype: --/- / Hgb H (ß4) is formed Hgb H is unstable and precipitates in vivo: compensated hemolysis occur splenomegaly RBC microcytic hypochromic target cells Heinz-bodies (precipitated Hgb H) 55 56 Mezei_RBC_2017 Mezei_RBC_2017 4./ Hemoglobin Barts or hydrops fetalis: chain is not produced at all; genotype: (--/--) chain cannot be raplaced by other chains 4 (Hemoglobin Barts) Characteristics: -high oxygen affinity -unstable -aggregate in oxidative stress - aggregates might bind to RBC membrane: - severe hemolysis - ineffective erythropoiesis (small degree) Might cause overhydration of RBCs Might lead to intrauterin death 57 II. EXTRACORPUSCULAR HEMOLYTIC ANEMIAS: Cause of hemolysis is located outside RBCs 1./ Immune hemolytic anemias a./ isoimmunisation/alloimmunisation: - transfusion of incompatible blood ABO (incomplete Ab / IgM) - Rh incompatibility: (complete Ab / IgG) hemolytic disease of neonates (morbus haemolyticus neonatorum) Rh (-) mother produces antibodies against Rh (+) RBCs of fetus. When maternal and fetal circulation contact, maternal antibodies harm fetal RBCs KERNICTERUS Pathomechanism: Lipid soluble ncBi penetrates to central nervous system because blood-brain-barrier is immature. In CNS ncBi is deposited to basal ganglions that are rich in lipids. This leads to neurological defects. Clinical signs: apathy, hypotoniciy, encephalopathy, rigidiy, chorea, hardness of hearing 58 Mezei_RBC_2017 Mezei_RBC_2017 b./ autoimmune hemolytic anemias /AIHA/: Definition: autoantibodies are produced against self RBCs Types: Detection: Coombs test A./ WARM AUTOIMMUNE HEMOLYTIC ANEMIAS: Direct Coombs test: Used for detection of RBCs covered by IgG. The test is positive if Coombs serum that contain anti-IgG and anticomplement cause agglutination of RBCs. Indirect Coombs test: Used for detection of free antibodies in serum. The test is positive if normal RBCs (not covered by antibodies), which are given to the examined serum, agglutinate in the presence of Coombs serum. Causes: Primary/Idiopathic/genetic susceptibility Secondary: associated to other diseases (SLE, RA, CLL, infection/ CMV, HIV) Drugs Pathomechanism: At body temperature IgGs are bound to RBCs These marked RBCs are detected by spleen and destroyed via phagocytosis. (extravascular hemolysis) Signs: RBC: Spherocyte RBCs are covered by IgG and C3 Direct antiglobulin test is positive 59 60 Mezei_RBC_2017 Mezei_RBC_2017 Drug induced autoimmune hemolytic anemias: Type 1: Hapten-mediated mechanism: Cause: im. high dose of penicillin or tetracyclin Mechanism: Type 2 allergic reaction The drug binds to RBC membrane as a hapten, thus becomes a complete antigen and IgG is produced against them, which binds to complete Ag RES filter/detect them RBC hemolysis Type 2 Immuncomplex-mediated mechanism „innocent bystander”: Cause: Kinidine, p-aminosalicylate, phenacetin, NSAID Mechanism Type 3 allergic reaction Drugs, as hapten, bind to plasma proteins and become complete antigen. IgM is produced against this antigen that binds to the antigen. Immuncomplexes are formed that nonspecifically cover RBCs, PLTs and glomerular endothelium and thus deposits are formed. IgM activates complement (C) and cause RBC hemolysis Type 3 Attachment of proteins to RBC surface Cause: Cephalothin Mechanism: non-immunologic process: Cause nonsepcific connection of different proteins (IgG, IgM, complement, tissue factor, albumin) to cell surface Rarely cause hemolysis Type 4 Autoantibody induction and attachemnt: Cause: Methyldopa, levadopa, procainamide, ibuprofen, diclofenac in high doses and prolonged administration Mechanism: Autoimmune disease due to defect of immune system T-supresor cell is inhibited by drugs and B-cell is activated, and IgG against Rh is produced 61 B./ COLD AUTOIMMUNE HEMOLYTIC ANEMIAS: Causes: Priary: unknown Secondary: acute: infections -mycoplasma pneumonia -infectious mononucleosis chronic: lymphoproliferative diseases Waldenström’s macroglobulinemia Autoimmune diseases Pathomechanism: -Primary cold autoimmune hemolysis: Attacks of painful acrocyanosis Cause: in cold (30 oC) RBC agglutination is caused by IgM in peripheral circulation IgM Ab titer is less than 1:1000 - Secondary cold autoimmune hemolysis: Occur when intravascular temperature is 20-25 oC Signs of hemolysis that is caused by monoclonal IgM Ab titer is higher than 1 : 1000 Signs: acrocyanosis, Raynaud’s phenomenon 62 Mezei_RBC_2017 Mezei_RBC_2017 C./ BITHERMIC IGG TYPE AIHA: - Paroxysmal cold hemoglobinuria: Cause: the most common AIHA in childhood - primary: unknown - secondary: syphilis, mumps, mononucleosis, Pathomechaanism: 20 oC: IgG and RBC attachment, IgG complement binding capacity of RBCs 37oC: IgG antibodies dissociate from RBCs complement is activated RBC hemolysis occur Signs of AIHA: Extravascular hemolysis: Lyisis of RBCs that are filtered by liver and spleen, thus (especially when chronic) hepatosplenomegaly occur Intravascular hemolysis: Rare, usually after acute infection Signs of increased bone marrow and peripheral RBC formation In decompensated hemolysis general signs of anemia are seen as well 2./ Non-immune haemolytic anemias Cause: Physical: a./ Mechanical or traumatic RBC injury large vessels: vessle graft, synthetic valves, march hemoglobinuria microcirculation: in microangiopathy (DIC, TTP, HUS) fibrin fibers cause RBC damage b./Heat: combustion Chemical: a./ Chemicals: copper, lead, distilled water b./ Biologic agents: snake, spider and bee bites, malaria Signs: Abnromal RBC shapes: occurence of schystocyte and acantocyte, etc RBC AGGLUTINATION 63 64 Mezei_RBC_2017 Mezei_RBC_2017 PROGRESS OF HEMOLYTIC ANEMIAS: 1./ Chronic a./ compensated hemolysis and - RBC formation (tenfold than normal) are seen, this compensate increased hemolysis and thus - there is no signs of anemia b./ decompensated, hemolysis and - RBC formation (erythropoiesis) are seen but this cannot compensate the amount of hemolysis and thus - signs of anemia are presented as well 2./ Acute (hemolytic crisis) a./ spontaneous b./ acute exacerbation of chronic hemolysis SIGNS OG HEMOLYTIC ANEMIAS GENERAL SIGNS Signs of increased RBC lysis: Blood: elevated Se nc indirect Bi Se free hemoglobin Se iron Se transferrin saturation Se K (released form disintegrated RBCs) Se LDH1 isoenzyme (also released from cells) decreased Se (free) haptoglobin level (in iv. hemolysis) Se hemopexin (only when Se haptoglobin level is unmeasurable) Se TIBC Feces: dark Urine: Ubg incerased Hemoglobinuria, and as a result proteinuria might occur (small Mw enables filtration via glmeruli; hemoglobinuiria occur only when extent reach the tubular maximum) Signs of increased RBC formation: Blood: reticulocytosis (sign of accelerated RBC formation) Bone marrow: erythroid hyperplasia CLINICAL SIGNS OF ACUTE HEMOLYTIC CRISIS - shivering, high body tempareture, sweating - dyspnea, tachypnea - drop of blood pressure - pruritus, urticaria, flush - headache - nausea, vomitus - hemoglobinuria COMPLICATIONS OF HEMOLYTIC ANEMIAS 1./ Chronic hemolytic anemias jaundice splenomegaly pigment gallstones 2./ Acute hemolytic anemias shock acute renal failure DIC 65 C./ ANEMIAS CAUSED BY/FOLLOWING BLOOD LOSS 1./Anemia following acute (recent) blood loss: Cause: sudden and severe blood loss Signs: Signs caused by hypoxia and hypovolemia: weakness, fatigue, sweating, thirst, pallor, dyspnea, coma and stupor Tachycardia, hypotension and hyperventilation Phases: a./ Shortly after blood loss: Hypovolemia causes catecholamine release and thus cause RBC mobilization form storages, thus RBC count remains normal b./ In some hours (approx. 3 hours): Hypovolemia cause: RAAS activation and ADH release Htk decreases Normocytic-normochromic anemia develops c./ In 1 day: Hypoxia erythropoietin (EPO) synthesis EPO cause increased RBC formation increased reticulocyte count Total normalization of RBC count and Hgb level requires 6-8 weeks Rate of regenartion depends on: severity of bleeding/hemorrhage and amount of stored iron 2./ Anemia following chronic (persistent) blood loss: Cause: occult (slight, unnoticed but long lasting) hemorrhages: in gastrointestinal system: ulcer, tu, hemorrhoids and salycilate urogenital system: menstruation hemorrhages: telangiectasis, thrombocyte count and functional disorder Signs: Signs of iron deficiency anemia D./ ABNORMAL DISTRIBUTION OF BLOOD Cause: hypersplenia syndrome portal hypertension myeloproliferative diseases storage disorders infectious diseases Pathomechanism: Increased RBC storage in enlarged spleen Signs: Pancytopenia, or only one cell line is affectd Hyperplastic bone marrow 66 Mezei_RBC_2017 Mezei_RBC_2017 67 68