Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
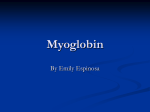
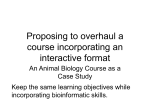
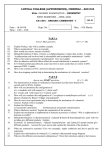
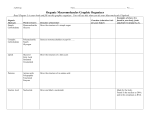
448 The Effect of Intracellular Oxygen Concentration on Lactate Release, Pyridine Nucleotide Reduction, and Respiration Rate in the Rat Cardiac Tissue Ryuichiro Araki, Mamoru Tamura, and Isao Yamazaki From the Biophysics Division, Research Institute of Applied Electricity, Sapporo Japan, Downloaded from http://circres.ahajournals.org/ by guest on August 1, 2017 SUMMARY. By measuring the absorbance change due to myoglobin oxygenation in hemoglobinfree isolated perfused rat hearts, we analyzed effects of perfusion pressure and heart rate upon the intracellular oxygen concentration. With Langendorff perfusion, the cardiac tissue was kept normoxic (above 50 ^M O2) at aortic pressure above 50 cm H2O, but became hypoxic (8 /XM O2) at 30 cm H2O. The increase in cardiac work, expressed as the product of peak systolic pressure and heart rate, increased oxygen consumption at aortic pressure of 50-200 cm H2O. The heart was kept normoxic under these conditions. Lactate release, oxygen consumption, and the oxidationreduction state of pyridine nucleotide were measured as a function of myoglobin oxygenation under various normoxic and anoxic conditions. Pyridine nucleotide fluorescence and lactate release started to increase as the intracellular oxygen concentration decreased to 6 and 10 ^M, respectively. Oxygen consumption was kept constant until the oxygen concentration decreased to 10 HM and slowed down below it. A close relationship between oxygen consumption and lactate release was observed. Infusions of epinephnne and norepinephrine under normoxic perfusion conditions increased cardiac work, oxygen consumption, and lactate release. More than 50% of myoglobin was then deoxygenated even under normoxic perfusion conditions. The increase in lactate release was ascribable to the increase in glycolytic flux caused by hypoxia. The change of pyridine nucleotide fluorescence by epinephrine was also explained by hypoxia in cardiac tissue. (Circ Res 53: 448-455, 1983) THE function of mammalian cardiac tissue is exquisitely sensitive to oxygen. Under hypoxic conditions, its mechanical performance declines rapidly, and the integrity of the tissue is compromised. This is due to the fact that myocardial energy production depends predominantly on the aerobic metabolism through /3-oxidation of fatty acid (Neely and Morgan, 1974). ATP synthesis through glycolysis in an anoxic state is insufficient to maintain cardiac performance at its normoxic level, although the glycolytic flux is significantly increased (Williamson, 1966a; Opie, 1976). Therefore, the intracellular oxygen concentration is crucial for normal function. The oxygen concentration in various tissue has been measured polarographically with a microelectrode (Broelsh et al., 1978; Silver, 1979). Optical methods have also been developed by several investigators (Longmuir and Knoop, 1976; Millikan, 1937; Chance, 1976; Jobsis, 1977; Opitz et al., 1978). For instance, emission of fluorescence at 470 run from excitation light at 340 nm can be used to detect changes in the content of reduced pyridine nucleotides. Chance and Schoener (1962) have studied correlations between the electrical activity of the cortex and the degree of pyridine nucleotide reduction caused by the transition from aerobiosis to anoxia. The dependence of the oxidation-reduction (redox) state of pyridine nucleotide on the oxygen concentration is calibrated with pigeon heart mitochondria by Sugano et al. (1974), who has reported that half-maximal reduction of pyridine nucleotide occurs at an oxygen concentration of 0.08 MM in state 3. Similarly, half-maximal reduction of cytochrome a + a3 occurs at oxygen concentrations of 0.3 /*M in state 3 and less than 0.07 ^M in state 4 (Oshino et al., 1974). These observations suggest the existence of a critical oxygen concentration, at which point respiration kinetics change from zero-order to firstorder with respect to the oxygen concentration (Longmuir, 1957; Jobsis, 1972). The concentration is below 1 mm Hg in mitochondria and above 10 mm Hg in several tissues (Chance, 1965; Wittenberg, 1970). The difference may be explained, in part, by the gradient of oxygen concentration between cytosolic and mitochondrial compartments (Tamura et al., 1978). Because of simplicity and convenience, the hemoglobin-free isolated heart perfused by the Langendorff technique has been used widely in the studies of myocardial energy metabolism. The fundamental characteristics of the preparation has been examined under various conditions (Williamson, 1964; Neely et al., 1967). The effects of various hormones and drugs on the energy metabolism have also been studied with this preparation, and the phosphorylation of some enzymes and membrane constituents Araki et a/./Myocardial Tissue Oxygenation is observed when catecholamine is added (Williamson, 1966b; Hiraoka et al., 1980). Since myoglobin is located in cytosolic space of the heart, its oxygenated degree reflects directly the oxygen concentration in the tissue (Tamura et al., 1978, 1983). We have measured the oxygenation state of myoglobin in the perfused rat heart by reflectance spectroscopy and determined the quantitative relation of the intracellular oxygen concentration with respiration rate, lactate release, and fluorescence of pyridine nucleotide under various experimental conditions. The detailed results are reported in this paper. Methods Downloaded from http://circres.ahajournals.org/ by guest on August 1, 2017 Hemoglobin-Free Isolated Perfused Heart Male albino rats of the Wistar strain (230-260 g body weight), fed on a commercial diet, were used. Rats were neither heparinized nor anesthetized throughout the experiments. Perfusion was carried out by a slightly modified method of Langendorff. The perfusion apparatus was essentially the same as that reported previously (Tamura et al., 1978). The aortic pressure was kept constant at 80 cm H2O unless otherwise noted. The perfusate contained 10 mM glucose and 2.5 ITIM calcium, equilibrated with a gas mixure of 95% O2 + 5% CO2 for normoxic, or 95% N2 + 5% CO2 for anoxic, conditions. The perfusate was not recycled in a flow-through system, and its temperature was maintained at 27°C. After equilibration for 15 minutes, hearts were subjected to the anoxic condition for about 1 minute by changing the oxygen-saturated perfusate to the nitrogen-saturated one. Changes in absorbance of myoglobin and fluorescence intensity of pyridine nucleotide for this normoxic-anoxic transition were full scale. Spectrophotometric Measurement of the Perfused Heart Dual-wavelength reflectance spectrophotometry was used to measure myoglobin oxygenation (Tamura et al., 1978, 1983). Light longer than 560 nm was guided onto the surface of left ventricle of perfused heart with a flexible light guide 1 cm in diameter. The light reflected from the heart was again guided into photomultipliers with a Yshaped light guide through a pair of interference filters. Measurement and reference wavelengths were 580 and 620 nm, and the difference in absorbance between the above two wavelengths was recorded. The oxidationreduction state of pyridine nucleotide was measured by slightly modified surface fluorometry, as described by Chance et al. (1965). The excitation light at 360 nm was guided into the left ventricle of perfused heart with a quartz light guide to excite reduced pyridine nucleotide in the tissue. The emitted light was guided into a photomulriplier for fluorescence measurement through a filter centered at 470 ± 20 nm. A part of the reflected light was guided into another photomultiplier, the output from which was used to subtract the artifact from the fluorescence signal with a difference amplifier. Heart Contractility and Cardiac Work The left ventricular pressure (LVP) was measured by using a microtip pressure transducer (model PC-350, Millar Instrument). A 22-gauge needle was inserted into the 449 left ventricle through the wall, and the pressure change was transmitted through a 1 -mm diameter vinyl tube filled with perfusate to a pressure transducer. The first derivative of left ventricular pressure change (dP/dt) was obtained electrically using a differentiating circuit with a time constant of 20 msec. Heart rate was measured with a frequency counter fed on the output of LVP or R wave of electrocardiogram (ECG). Cardiac work was expressed as the product of peak systolic pressure and heart rate (mm Hg/min) according to the method of Kobayashi and Neely (1979). Coronary Flow The flow rate was measured continuously with an electromagnetic flow meter (MFV-110, Nihon Koden) with a flow probe placed in the perfusion circuit. Oxygen Concentration in Effluent Perfusate, and Oxygen Consumption A Tygon tube with a diameter of 1 mm was inserted into the pulmonary artery, and a portion of the effluent perfusate was pumped through the electrode chamber at a constant rate of 1 ml/min. A Clark-type oxygen electrode was inserted into the chamber. The inflowing oxygen concentration was measured similarly with a 22-gauge needle inserted into the perfusion circuit. The rate of oxygen consumption was calculated as a product of flow rate and difference in the oxygen concentration between inflowing and effluent perfusates. Assay of Lactate in the Effluent Perfusate For determination of lactate release from the heart, the effluent perfusate from the pulmonary artery was collected in the test tube for 4 seconds at appropriate time intervals. The concentration of lactate was determined enzymatically (Gutman and Wahlefeld, 1974) and the inflowing perfusate was used as reference. Materials The enzymes for the lactate assay were purchased from Boehringer Mannheim Gmbh. Epinephrine hydrochloride and dopamine hydrochloride were obtained from Sigma and Nakarai Chemicals, respectively. All other chemicals were of analytical reagent grade. Results Effects of Perfusion Pressure and Heart Rate on the Heart Function Figure 1 shows the effect of perfusion pressure on absorbance of myoglobin and various parameters characterizing the cardiac performance. The absorbance change due to an aerobic-anaerobic transition was shown at the right of the figure for calibration. The change corresponded to the full scale for deoxygenation of myoglobin because no further change in absorbance was seen by electric stimulation, epinephrine infusion, or nitrogen flowing on the heart surface. When perfusion pressure was decreased from 80 to 30 cm H2O, the flow rate and left ventricular pressure decreased markedly. The oxygen concentration in the effluent perfusate decreased from 0.83 to 0.55 mM, and about 50% of 450 Circulation Research/Vol. 53, No. 4, October 1983 (B) (A) Calibration Perfusion Pressure (cmhbO) 60 |30|50| 80 1110 11301 150 11301110' O2 Concentration in Effluent Myoqlotrin I Oxygenation (580-620nm) Heart Rate Flow Rate .•D00 |0 snHg -1000 LVdP/dt L -v- V P —|5mmh- -H5mmH- Downloaded from http://circres.ahajournals.org/ by guest on August 1, 2017 FIGURE 1. Various cardiac performances modified externally. Rat heart was perfused with a Krebs-Ringer bicarbonate solution equilibrated with 95% 02 + 5% C02. Part A: perfusion pressure (shown in top column) was changed by changing the height between the aorta and reservoir. Part B: calibration traces were obtained from normoxicanoxic transition, in which the perfusate was switched to that equilibrated with 95% N2 + 5% CO2. total myoglobin was in the deoxygenated form at 30 cm H2O. Then, the intracellular oxygen concentration was estimated at 4 FIM. Increasing perfusion pressure up to 50 cm H2O caused increases in left ventricular pressure and flow rate, whereas the oxygen concentration in the effluent perfusate decreased to 0.22 mM. The original level of myoglobin oxygenation was nearly restored. Increasing the perfusion pressure stepwise up to 150 cm H2O were accompanied by parallel increases in left ventricular pressure, flow rate and the oxygen concentration in the effluent perfusate. Myoglobin oxygenation was saturated at 110 cm H2O of perfusion pressure. Heart rate remained almost constant during the experiment. The first derivative of left ventricular pressure (dP/dt) also increased with left ventricular pressure. WTien the perfusion pressure was increased from 80 to 200 cm H2O, lactate release from the heart increased from 0.15 ± 0.05 to 0.23 ± 0.02 ^mol/min per g wet weight, and the intensity of pyridine nucleotide fluorescence decreased slightly. Oxygen consumption increased from 2.5 ± 0 . 1 to 10.1 ± 0.3 Mmol/min per g wet weight with the increase in perfusion pressure from 50 to 200 cm H2O, which was linearly related to the cardiac work (cf. Fig. 5). This agreed with the result of Kobayashi and Neely (1979), who observed similar linearity upon a change in the aortic resistance. Since myoglobin was almost fully oxygenated under the conditions studied, it was evident that oxygen supply did not limit oxygen consumption. The linear dependence of oxygen consumption on cardiac work was also obtained when heart rate was raised from 90 to 210/min by pacing under 80 cm H2O of perfusion pressure (data not shown). Normoxic-Anoxic Transition When the oxygen-saturated perfusate was switched to the nitrogen-saturated one (Fig. 2A), the deoxygenation of myoglobin was completed within 1 minute. The reduction of pyridine nucleotide started when about 30% of total myoglobin was deoxygenated. The lactate concentration in the effluent perfusate increased markedly under the hypoxic conditions. After anaerobiosis was achieved, the nitrogen-saturated perfusate was switched to the oxygen-saturated one. The oxygenation of myoglobin responded first; then, the oxygen concentration in the effluent perfusate increased. Pyridine nucleotide started to oxidize when more than 10% of myoglobin was oxygenated, and reached the original level after myoglobin was completely oxygenated. Recovery of the lactate concentration in the effluent perfusate to the original level was later than the recovery of myoglobin oxygenation. In comparison with the experiment in Figure 2A, the oxygen concentration in the inflowing perfusate was changed at a 10 times slower rate, in Figure 2B, by continuously changing the oxygen:nitrogen ratio in the perfusate. The oxygen dependence of cardiac performances was the same in the two cases when the oxygen concentration was decreased, but was not when it was increased from anoxia. Reoxidation of pyridine nucleotide and recovery of lactate release were completed before the complete oxygenation of myoglobin. Figure 3A shows changes in lactate release, pyri- -H 5min KFIGURE 2. Changes in various performances of perfused heart due to normoxic-anoxic transition. Part A. the perfusate equilibrated with 95% 02 + 5% C02 was switched to that equilibrated with 95% N2 + 5% C02 by using an electric solenoid valve. The perfusate was changed within 5 seconds. Part B: the heart was perfused first with 95% 02 + 5% C02. The oxygen concentration of inflowing perfusate was decreased at a rate of 50 IIM O2/min by decreasing the Oj.N2 ratio of the gas mixture, and was again increased from an arrow at a rate of 100 p.u O2/min. Araki et a/./Myocardial Tissue Oxygenation 451 oxygen consumption were about 1, 3, and 2.6 /XM, respectively. The same results as in Figure 3 were given by transmission spectroscopy in which a thin light pipe was inserted into left ventricle and the light transmitted through the left ventricular wall was recorded (Tamura et al., 1978). Thus, it was concluded that there was no appreciable difference in the oxygenation state of the heart between endo- and epicardium under our perfusion conditions. 0 10 20 30 70 Downloaded from http://circres.ahajournals.org/ by guest on August 1, 2017 Intracellutar Chqgtn Concentration (JJM) FIGURE 3. Relationships of myoglobin oxygenation to pyridine nucleotide fluorescence, lactate release, and oxygen consumption during normoxic-anoxic transition. The conditions were as described in Figure 1 Open circles with a vertical line represent mean values of six hearts, and the lines represent ± SEM. Data were plotted against the percent oxygenation of myoglobin in part A and against the intracellular oxygen concentration in part B. In the top of part B, • represent respective data obtained from another series of experiments. dine nucleotide fluorescence, and oxygen consumption as a function of the oxygenation state of myoglobin. Lactate release started to increase when about 30% of myoglobin was deoxygenated, and reached a half maximum at 50% deoxygenation. The halfmaximal reduction of pyridine nucleotide was observed at 70% deoxygenation. Oxygen consumption changed inversely with lactate release. Identical curves were obtained by either increasing or decreasing the oxygen concentration in the inflowing perfusate at a rate below a certain limit. For instance, the curves started to change when the oxygen concentration was decreased at rates above 90 /iM/ and when it was increased at rates above 40 min. Therefore, we assumed that the steady state is maintained during the slow changes in the oxygen concentration, similar to the steady state which can be assumed in enzyme reactions. In Figure 3B, these results are replotted as a function of the intracellular oxygen concentration, with the use of an oxygen dissociation curve of myoglobin determined previously in the heart (Tamura et al., 1978). Pyridine nucleotide fluorescence and lactate release started to increase at oxygen concentrations lower than 6 and 10 tiu, respectively. Lactate release was 6-fold higher in anoxia (lower than 0.1 ^M oxygen) than in normoxia. Oxygen consumption started to fall at oxygen concentrations lower than 10 HM, and the rate remained constant above the concentration. The oxygen concentrations required for half-maximal pyridine nucleotide reduction, lactate release, and Effects of Epinephrine and Dopamine in Cardiac Function Figure 4A shows the effect of epinephrine infusion upon cardiac performance under normoxic perfusion conditions. The infusion increased both left ventricular pressure and heart rate. The cardiac work rose from 6300 to 19110 mm Hg/min and the rate of oxygen consumption from 3.2 ± 0.2 to 6.7 ± 0.3 jimol/min per g wet weight. The increase in oxygen consumption caused the decrease in the intracellular oxygen concentration, resulting in deoxygenation of myoglobin. Maximally, about 60% of myoglobin was deoxygenated, and then the oxygen concentration in cardiac tissue was estimated at 3 /IM. The maximum deoxygenation of myoglobin appeared after cardiac work or oxygen consumption reached a maximum. Lactate release started to increase when about 30% of myoblobin was deoxygenated. The lactate release depended closely on the oxygenated state of myoglobin. The maximal lactate release (0.5 ^mol/min per g wet weight) was placed at the maximal myoglobin deoxygenation. The results on norepinephrine infusion were similar to those on epinephrine (data not shown). The effect of dopamine infusion was shown in Figure 4B, where a dose of 100 Mg/ml was used to give similar values for cardiac work and oxygen (A) (A) Eprephnnt (cottjl FIGURE 4. Effects of epinephrine and dopamine infusions on cardiac performances under normoxic perfusion. Hearts were perfused with a Krebs-Ringer solution equilibrated with 95% O2 + 5% CO2 at an aortic perfusion pressure of 80 cm HiO. The infusions of drugs were continued for 30 seconds, as indicated by bars. Part A- epinephrine (1 lig/ml). Part B: dopamine (100 ng/ml). Circulation Research/Vol. 53, No. 4, October 1983 452 (A) (B) 0.6i 5 % .s-0.53 * \. 0.2 06 ifai.05 § | 03 T \ / I.01 A 0 10 20 30 50 Intracetlular Oxygen Concentration (pM) a3oi 0 5 10 15 20 25 30 P»* Systolic Presare « Heart Rate 3 (mmHg/min) » 10~ Downloaded from http://circres.ahajournals.org/ by guest on August 1, 2017 FIGURE 5. Relationships between cardiac performances modified by infusions of dopamme, epmephnne, and norepinephnne. The conditions were as described in Figure 4. Part A: oxygen consumption and lactate release were plotted against cardiac work. O, normoxic-anoxic transition (Figs 2 and 3); A, dopamine; O, epinephrine; • , norepinephnne (Fig. 4). Each vertical line represents ± sEMfor six tO, A) or eight (D, M) hearts. Part B: lactate release was plotted against the intracellular oxygen concentration. Each vertical line for epinephnne (O) and dopamme (O) represents ± SEMfor eight hearts. The data for norepinephrine (M) were the mean value for two hearts. Solid line was replotted from Figure 3B (middle). consumption, as compared with epinephrine infusion. Dopamine caused marked increases in left ventricular pressure, heart rate, and oxygen consumption (maximum; 7.1 ± 0.6 ^mol/min per g wet weight). Cardiac work rose from 7,000 to 16,800 (maximum) mm Hg/min, accompanying a parallel increase in oxygen consumption (cf. Fig. 5). Lactate release did not increase under this condition. The maximal deoxygenation of myoglobin was about 30% of that obtained with epinephrine. Flow rate was increased by dopamine but not by epinephrine. This might explain the difference in myoglobin oxygenation between the two cases. The relationships between cardiac work, oxygen consumption, and lactate release were summarized in Figure 5. Figure 5A shows that the increase in oxygen consumption depended linearly on the cardiac work when the change was caused either by dopamine or by an increase in perfusion pressure (Fig. 1). In contrast, the epinephrine- and norepinephrine-induced increases in oxygen consumption deviated from the straight line above 5.5 /imol/min per g wet weight. Lactate release was also plotted against cardiac work. When cardiac work was varied from 4,000 to 20,000 mm Hg/min by dopamine or perfusion pressure, lactate release increased slightly from 0.15 ± 0.05 to 0.23 ± 0.02 ^mol/min per g wet weight. At cardiac works above 12,000 mm Hg/ min, lactate release induced by either epinephrine or norepinephrine increased markedly and deviated from the plots obtained by changing perfusion pressure. Lactate release measured under various conditions was plotted against the intracellular oxygen concentration in Figure 5B. The plots obtained with epinephrine and dopamine all coincided with the curve obtained by normoxic-anoxic transition shown in Figure 3B (middle). Changing the dose of epinephrine from 0.01 to 2 ng/m\ did not change the curve shown in Figure 5 (data not shown). Fluorescence Changes of Pyridine Nucleotide Figure 6 shows the effect of increasing oxygen consumption on the redox state of pyridine nucleotide under normoxic and hypoxic conditions. Increasing heart rate from 90 to 110 in normoxia caused an increase in oxygen consumption from 2.5 to 3.1 ^mol/min per g wet weight (Fig. 6A). About 30% of myoglobin was then in the deoxygenated form. Pyridine nucleotide was oxidized and the reduced form was about 10% of that at transient anoxia. Under hypoxic conditions (Fig. 6B), however, the result was different. At an oxygen concen(A) (h Concentration n Effluent ~ Myoglotun Oxvqenation (580-620nm| oxidation of Pynkie Nucleoti 1360— WOnm) Flow Rate FIGURE 6. Effects of heart rate on the redox state of pyridine nucleotide under normoxic (part A) and hypoxic (part B) conditions. Heart was perfused with 95% O2 + 5% CO2 in part A and with 40% O2 + 55% Ni + 5% CO-i in part B. The heart rate rose spontaneously from 90 to no/min by electric pulse. Araki et a/./Myocardial Tissue Oxygenation 453 Downloaded from http://circres.ahajournals.org/ by guest on August 1, 2017 tration of 0.4 mM in the inflowing perfusate, 50% of myoglobin was deoxygenated. Increasing heart rate under this condition caused increases in oxygen consumption from 1.9 to 2.1 ^mol/min per g wet weight and in myoglobin deoxygenation from 50% to 65%, similarly as shown in Figure 6A. In contrast to the result in Figure 6A, however, pyridine nucleotide was further reduced when heart rate increased (Fig. 6B). Upon an increase in oxygen consumption, pyridine nucleotide was oxidized at oxygen concentrations above 10 ^M, but was reduced below it. Figure 7 shows redox changes of pyridine nucleotide induced by epinephrine (A) and dopamine (B). Experimental conditions were the same as those in Figure 4. The response of fluorescence intensity of pyridine nucleotide to an epinephrine dose was triphasic. The initial oxidation of pyridine nucleotide began with an increase in cardiac work or oxygen consumption. The switch from oxidation to reduction occurred when 40% of myoglobin was deoxygenated. The maximal reduction of pyridine nucleotide was seen later than maximal deoxygenation of myoglobin. Re-oxidation of pyridine nucleotide occurred and its redox state reached the initial level before myoglobin oxygenation and oxygen consumption returned to their initial levels. Thus, lactate release did not parallel the redox level of pyridine nucleotide. Infusion of dopamine, on the other hand, resulted in the oxidation of pyridine nucleotide by 10-15% of the normoxic-anoxic response. No reduction was seen in this case. Discussion Oxygenation State of Myoglobin in the Heart Under normal perfusion conditions at 27-30°C, more than 90% of myoglobin is oxygenated (Tamura et al., 1978) and the intracellular oxygen concentration is kept higher than 50 HM. This is consistent OjConcentraton «i Effluent ImM] Oxidation of | Pyndinc Nucltohdi (360—WOraa) [ 1min I Smin I I Sm FIGURE 7. Effects of infusions of epinephrine (part A) and dopamine (part B) on the redox state of pyridine nucleotide. The calibration for normoxic-anoxic changes in myoglobin oxygenation and pyndine nucleotide fluorescence is shown on the left. Epinephrine (1 iig/ml) and dopamine (100 ng/ml) were infused for 30 seconds. The other experimental conditions were as described in Figure 4. with the observation that absorbance of myoglobin does not change until the oxygen concentration in the inflowing perfusate is decreased to 0.7 rrtM (70% O2 saturation). At a perfusion temperature of 37°C, however, more than 30% of myoglobin was deoxygenated, even under normoxic perfusion conditions, where the heart beats spontaneously at a rate of 240-280/min. The intracellular oxygen concentration approaches 10 MM under these conditions. In order to avoid hypoxia under standard conditions, the present experiments have been carried out at 27°C. Therefore, the rates of oxygen consumption and lactate release are slow as compared with those reported previously (Williamson, 1966a, 1966b; Neely et al., 1967; Kobayashi and Neely, 1979). The oxygen concentration in the effluent perfusate (corresponding to the oxygen concentration at coronary sinus), cannot be used simply as an indicator for the tissue oxygenation state. As seen in Figure 1, the ratio of oxygen concentrations in the tissue and in the effluent perfusate is inverted between perfusion pressures of 30 and 50 cm H2O. Oxygen appears to be transferred from the circulating system into the intracellular space about 10-fold faster at 50 cm H2O than at 30 cm H2O. This phenomenon cannot be explained simply by an increase in the flow rate. Probably, the capillary bed might close at a perfusion pressure of 30 cm H2O. Although the oxygen concentration in the effluent perfusate decreases to about 0.2 mM upon infusion of either dopamine or epinephrine, the intracellular oxygen concentration is much higher in the former than in the latter (Fig. 6). This indicates that an increased flow rate by dopamine delivers oxygen into the tissue effectively. Thus, there seems no parallel between the flow rate, the oxygen concentration in the effluent perfusate, and the tissue oxygenation state. Infusion of adenosine to the perfused heart causes increases both in flow rate and oxygen concentration in the effluent, whereas myoglobin is deoxygenated. Dipyridamole gives similar results (Tamura et al., 1983). Effect of Oxygen Concentration on Respiration Rate, Lactate Production, and Pyridine Nucleotide Fluorescence The rate of oxygen consumption begins to decrease at an oxygen concentration of 10 HM, which may be called the critical oxygen concentration in the heart, although there is an argument with regard to this terminology (Wilson et al., 1973). This value is 10-fold higher than that obtained with isolated mitochondria (Longmuir, 1957; Jobsis, 1972). The difference can be accounted for by the oxygen concentration gradient between the cytosolic and mitochondrial spaces (Tamura et al., 1978). It is of interest to note that the deoxygenation of myoglobin commences at the critical oxygen concentration. This implies that myoglobin participates in regulating the oxygen concentration in the heart. Nishiki et al. (1979) have examined the interde- Circulation Research/Vol. 53, No. 4, October 1983 454 _ 0.5 a | 0.4 •S * 0.3-£j 0.2 |1 020 1 2 AOxygen Consumption (>m>oles/ming wet weight) FIGURE 8. Plots of the extra release of lactate against the deviation of oxygen consumption from the requirement for work. The deviation was caused by anoxia (O) and by infusions of epinephrine (O) and norepinephrine (U). The amounts of deviation correspond to the difference between the two lines shown in Figure 5A. Vertical and horizontal lines represent ± SEM. Downloaded from http://circres.ahajournals.org/ by guest on August 1, 2017 pendence of oxygen consumption and glycolytic flux in the aerobic steady state using Amytal as a respiratory inhibitor, and have shown that time courses of oxygen consumption and lactate production are mirror images of one another. The same relation between oxygen consumption and lactate release is seen in the normoxic to hypoxic transition (Fig. 3B). Figure 8 shows that the deviation from the expected values occurs proportionally with a value of about 5 for —A[O2]/A[lactate]. This relationship might be applied to blood-circulated heart or skeletal tissues, in which the lactate level of venous blood has been used as an indicator for hypoxia. The fluorescence intensity of pyridine nucleotide also reflects the intracellular oxygen concentration (Fig. 3). Since percent reduction of cytochrome a + a3 is proportional to the oxygenation state of myoglobin (Tamura et al., 1978), the percent reduction of pyridine nucieotide is plotted against percent reduction of cytochrome a + a3 in Figure 9. The curve for the heart resembles that in state 3 of isolated mitochondria (Sugano et al., 1974; Oshino et al., 1974). Chance (1959) and Jobsis et al. (1963), using perfused frog sartorius muscle, have observed that pyridine nucleotide oxidized during contraction is reduced back to the original level in the resting state. Such a stimulation-induced oxidation of pyridine nucleotide is seen in normoxia (Fig. 6A). In isolated mitochondria, an ADP-induced stimulation of respiration causes oxidation of pyridine nucleotide (Chance et al., 1964). In this connection, Chance (1964) demonstrated that increased stimulation caused first an oxidation and then the reduction of pyridine nucleotide on the frog sartorius muscle. The reduction of the pyridine nucleotide was explained by the local hypoxia, where oxygen demand exceeded the supply. In Figure 6B, however, when the heart was stimulated, the intracellular oxygen concentration decreased only slightly from 4 to 3.5 JTM, although deoxygenation of myoglobin was much more distinct. Therefore, a stimulation-induced reduction observed in Figure 6B cannot be explained clearly. Sugano et al. (1974) have reported that the plot of pyridine nucleotide reduction against the oxygen concentration is shifted toward the higher oxygen concentration when respiration is increased. For instance, its half reduction is observed at 0.08 ^M in state 3 and 0.02 JIM in state 4 of mitochondria. Thus, the stimulation-induced reduction (Fig. 6B) may be accounted for not only by the development of hypoxia, but also by a shift in the curve on the formation of ADP from ATP under hypoxic conditions. It seems likely that the change in fluorescence intensity comes mainly from the redox change of pyridine nucleotide in mitochondria. Epinephrine and Dopamine Infusions As shown in Figure 5A, on epinephrine infusion, the rate of oxygen consumption reaches a maximum (6 Mmol/min per g wet weight), even though the cardiac work increases further. The further increase in the cardiac work is accompanied by an increase in lactate release. The insufficiency of ATP production through oxidative phosphorylation may be compensated by an increase in glycolytic flux. As shown by Kobayashi and Neely (1979), and also in Figure 5A, glycolytic flux was increased when cardiac work was raised in the normoxic conditions. However, the epinephrine-induced increase of the flux could not be explained by the above, because at the same cardiac work, lactate release was more than 3-fold larger in the heart after epinephrineinfusion than that of increasing perfusion pressure or dopamine-infusion. Figure 5B shows that such an increase in the glycolytic flux is rather indicative of the hypoxic condition in cardiac tissue. The increased amount of lactate release is proprononal to the decreased amount of oxygen consumption, but a molar ratio Alactate:Aoxygen of about 0.2 (Fig. 8) is too small to supplement the lack of ATP production through glycolytic flux. The reason remains to be determined by further experiments. Chance et al. (1965) have reported complex re- 0 20 40 60 80 100 % Oxidation of Cyt a + FIGURE 9. The relationship between the redox changes of pyridine nucleotide and cytochrome a + a3 in the heart and in isolated mitochondria. The plots (O) were calculated from data in Figure 3A and by others (Oshino el al., 1974; Tamura et al., 1978). The solid line was obtained by Sugano et al. (1974) in state 3 of isolated mitochondria with glutamate and the dashed line in state 4. Araki et a/./Myocardial Tissue Oxygenation sponses of pyridine nucleotide fluorescence to epinephrine. A triphasic response of the fluorescence seen in Figure 7 A agrees with the result of Williamson (1964), who has interpreted the abnormality as follows: the initial oxidation corresponds mainly to oxidation of mitochondrial pyridine nucleotide through an increase in ADP, and the subsequent reduction is ascribed to reduction of pyridine nucleotide due to glycogenolysis and glycolysis (Williamson and Jamieson, 1966). Figure 7 A shows that the reduction of pyridine nucleotide commences when about 40% of myoglobin is deoxygenated. Then, the intracellular oxygen concentration is about 8 HM. This concentration appears to be critical to determine the direction of oxidation-reduction of pyridine nucleotide in our perfused rat heart (Fig. 6). Downloaded from http://circres.ahajournals.org/ by guest on August 1, 2017 This study was supported by Grant in Aid for Scientific Research (343029, 57440097) from the Ministry of Education, Science, and Culture of japan. Address for reprints: Mamoru Tamura, Biophysics Division, Research Institute of Applied Electricity, Sapporo 060, Japan. Received November 2, 1982; accepted for publication July 20, 1983. References Broelsch C, Hoper J, Kessler M (1978) Oxygen supply to the cirrhotic liver following various portacaval shunt procedures. Adv Exp Med Biol 94: 633-641 Chance B (1959) The response of mitochondria to muscular contraction. Ann NY Acad Sci 81: 477-489 Chance B (1964) Discussion. In Oxygen in the Animal Organisms, edited by F Dickens, E Neil. London, Pergamon Press, pp 355358 Chance B (1965) Reaction of oxygen with the respiratory chain in cells and tissues. J Gen Physiol 49: 163-188 Chance B (1976) Pyridine nucleotide as an indicator of the oxygen requirements for energy-linked functions of mitochondria. Ore Res 38: (suppl I): 31-38 Chance B, Schoener B (1962) Correlation of oxidation-reduction changes of intracellular reduced pyridine nucleotide and changes in electroencephalogram of the rat in anoxia. Nature 195: 956-958 Chance B, Schoener B, Schindler F (1964) The intracellular oxidation-reduction state. In Oxygen in the Animal Organisms, edited by F Dickens, E Neil. London, Pergamon Press, pp 367392 Chance B, Williamson JR, Jamieson D, Schoener B (1965) Properties and kinetics of reduced pyridine nucleotide fluorescence of the isolated and in vivo rat heart. Biochem Z 341: 357-377 Gutmann I, Wahlefeld AW (1974) L(+) lactate. Determination with lactate dehydrogenase and NAD. In Methods of Enzymatic Analysis, vol 3, edited by HV Bergmeter. New York, Academic Press, pp 1464-1468 Hiraoka T, DeBuysere M, Olson MS (1980) Studies of the effects of a-adrenergic agonists on the regulation of pyruvate dehydrogenase in the perfused rat heart. J Biol Chem 255: 76047609 Jobsis FF (1963) Spectrophotometric studies on intact muscle. II. 455 Recovery from contractile activity. J Gen Physiol 46: 928-969 Jobsis FF (1972) Oxidative metabolism at low Po2. Fed Proc 31: 1404-1413 Jobsis FF (1977) Noninvasive, infrared monitoring of cerebral and myocardial oxygen sufficiency and circulatory parameters. Science 198: 1264-1267 Kobayashi K, Neely JR (1979) Control of maximum rates of glycolysis in rat cardiac muscle. Circ Res 44: 166-175 Longmuir IS (1957) Respiration rate of rat-liver cells at low oxygen concentrations. Biochem J 65: 378-382 Longmuir IS, Knopp JA (1976) Measurement of tissue oxygen with a fluorescent probe. J Appl Physiol 41: 598-602 Millikan GA (1937) Experiments on muscle hemoglobin in vivo: The instantaneous measurements of muscle metabolism. Proc R Soc Lond [Biol] 123: 218-241 Neely JR, Morgan HE (1974) Relationship between carbohydrates and lipid metabolism and the energy balance of heart muscle. Annu Rev Physiol 36: 413-458 Neely JR, Liebermeister H, Battersby EJ, Morgan HE (1967) Effect of pressure development on oxygen consumption by isolated rat heart. Am J Physiol 212: 804-814 Nishiki K, Erecinska M, Wilson DF (1979) Effect of Amytal on metabolism of perfused rat heart: Relationship between glycolysis and oxidative phosphorylation. Am J Physiol 237: 221-230 Opie LH (1976) Effects of regional ischemia on metabolism of glucose and fatty acids. Circ Res 38: (suppl I): 52-67 Opitz N, Weigelt H, Barankay T, Lubbers DW (1978) Application of the optode to measurements of surface Po2 and Pco2 of the isolated guinea-pig heart. Adv Exp Biol Med 94: 99-105 Oshino N, Sugano T, Oshino R, Chance B (1974) Mitochondrial function under hypoxic conditions. The steady states of cytochrome a + a3 and their relation to mitochondrial energy states. Biochim Biophys Acta 368: 298-310 Silver IA (1979) The significance of clinical assessment of brain tissue oxygenation in different pathological conditions. An overview. Fed Proc 38: 2495-2500 Sugano T, Oshino N, Chance B (1974) Mitochondrial functions under hypoxic conditions. The steady states of cytochrome c reduction and of energy metabolism. Biochim Biophys Acta 347: 340-358 Tamura M, Oshino N, Chance B, Silver IA (1978) Optical measurements of intracellular oxyen concentration of rat heart in vitro. Arch Biochem Biophys 191: 8-22 Tamura M, Araki R, Yamazaki I (1983) Myoglobin-probed optical studies on myocardial tissue oxygenation. Effect of adenosine and hypoxia. In Physiology and Pharmacology of Adenosine Derivatives, edited by JW Daly, Y Kuroda, JW Phillis, H Shimizu, M Ui. New York, Raven Press, pp 13-20 Williamson JR (1964) Metabolic effects of epinephrine in the isolated, perfused rat heart. J Biol Chem 239: 2721-2729 Williamson JR (1966a) Glycolytic control mechanisms. II. Kinetics of intermediate changes during the aerobic-anoxic transition in perfused rat heart. J Biol Chem 241: 5026-5036 Williamson JR (1966b) Kinetic studies of epinephrine effects in the perfused rat heart. Pharmacol Rev 18: 205-210 Williamson JR, Jamieson D (1966) Metabolic effects of epinephrine in the perfused rat heart. I. Comparison of intracellular redox states, tissue PO2, and force of contraction. Mol Pharmacol 2: 191-205 Wilson DF, Owen C, Mela L, Weiner L (1973) Control of mitochondrial respiration by the phosphate potential. Biochem Biophys Res Commun 53: 326-333 Wittenberg JB (1970) Myoglobin-facilitated oxygen diffusion. Role of myoglobin in oxygen entry into muscle. Physiol Rev 50: 559-636 INDEX TERMS: Myoglobin • Hypoxia • Intracellular oxygen concentration • Critical oxygen concentration The effect of intracellular oxygen concentration on lactate release, pyridine nucleotide reduction, and respiration rate in the rat cardiac tissue. R Araki, M Tamura and I Yamazaki Downloaded from http://circres.ahajournals.org/ by guest on August 1, 2017 Circ Res. 1983;53:448-455 doi: 10.1161/01.RES.53.4.448 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1983 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/53/4/448 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/