Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
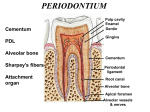
CEMENTUM INTRODUCTION CEMENTUM IN HEALTH CONTENTS TYPES OF CEMENTUM CLASSIFICATION COMPOSITION PERMEABILITY OF CEMENTUM FUNCTION OF CEMENTUM CEMENTO ENAMEL JUNCTION CEMENTODENTINAL JUNCTION THICKNESS OF CEMENTUM CEMENTUM IN DISEASE HYPERCEMENTOSIS ANKYLOSIS CEMENTUM RESORPTION & REPAIR EXPOSURE OF CEMENTUM IN ORAL ENVIRONMENT INTRODUCTION Periodontium is the functional unit of tissues supporting the tooth. It consists of four principal components: Gingiva Periodontal ligament Cementum Alveolar bone Cemetum- Its a calcified avascular mesenchymal tissue that forms the outer covering of anatomic root. It provides anchorage mainly to the principal fibres of periodontal ligament. CEMENTUM IN HEALTH TYPES OF CEMENTUM There are two main types of cementum: Acellular(primary) cementum Cellular(secondary) cementum Two main sources of collagen fibres in the cementum are: Sharpey’s fibres(extrinsic)-which are the embedded portion of principal fibres of periodontal ligament and are formed by the fibroblast Intrinsic fibres-Fibres that belongs to the cementum matrix and are produced by cementoblast Acellular cementum it is the first cementum formed, it covers approximately the cervical third or half of the root. It does not contain cells. It is formed before the tooth reaches the occlussal plane and its thickness ranges from 30-230 micronmeter. Sharpey’s fibres make up most of the structure of acelluler cementum which has a principal role in suppoting the tooth. Most fibres are inserted at approximately right angles into the root surface and penetrate deep into the cementum. But others enter from several different direction Acellular cementum also contains intrinsic collagen fibrils that are calcified and irregularly arranged or parellel to the surface Cellular cementum It is formed after the tooth reaches the occlusal plane, is more irregular and contain cells(cementocytes) in individual spaces(lacunae) that communicate with each other through a system of anastomosing canaliculi. It is less calcified tahn the acellular type. Sharpey’s fibres occupy smaller portion of cellular cementum and are seperated by other fibres that are arranged either parallel to the root surface or at random. ‘ •Sharpey’s fibres may be completely or partially calcified or may have a central uncalcified core surrounded by a calcified border •Both cellular and acellular cementum are arranged in lamellae separated by incremental lines parallel to the long axis of the root. These lines represent “rest periods” in cementum formation and are more mineralized than adjacent cementum CLASSIFICATION Based on location,morphology and histological appearence Schroeder has classified the cementum as follows: Acellular afibrillar cementum(AAC)- It contains neither cells nor extrinsic or intrinsic collagen fibres, apart from a mineralized ground substance. Acellular extrinsic fibre cementum(AEFC)-It is composed of densely packed bundles of Sharpey’s fibres and lack cells.It is a product of fibroblast and cementoblast and in humans is found in the cervical third of roots Cellular mixed stratified cementum(CMSC)- It is composed of composed of extrinsic (sharpey’s )and intrinsic fibers and contains cells.It is a co product of fibroblast and cementoblasts. Cellular intrinsic fiber cementum(CIFC)Contain cells but no extrinsic collagen fibers.It is formed by cementoblasts. Intermediate cementum It is poorly defined zone near the cementodentinal junction of certain teeth that appears to contain cellular remnants of Hertwig’s sheath embedded in calcified ground substance. COMPOSITION Cementum is composed of both inorganic and organic matter. The inorganic content of cementum (hydroxy apatite)is 45% -50% ,which is less than that of bone,enamel or dentin . The organic matrix is composed 90% type I collagen ,5% typeIII callagen,and non collagenous proteins like enamel protein ,adhesion molecules like tenacin,and fibronectin,glycosaminoglycans like chondroitin sulphate and heparan sulfate. The protein extract of mature cementum promote cell attachment and cell migration and stimulate protein CEMENTOENAMEL JUNCTION Three types of relationship involving the cementum exist at the CEJ . In about 60% -65% of cases cementum overlaps the enamel . In about 30% of cases an edge-to-edge butt joint exists. In 5%-10% of cases the cementum and the enamel fails to meet.In this case gingival recession may result in accentuated sensitivity because of exposed dentin. CEMENTO DENTINAL JUNCTION The terminal apical area of the cementum where it joins the the internal root canal dentin is known as cemento dentinal junction. When the root canal treatment performed ,the obturating material should be at the CDJ . There is no increase or decrease in the width of the CDJ with age. . CEMENTUM IN DISEASE HYPERCEMENTOSIS Hypercementosis refers to the prominent thickening of cementum,with nodular enlargement of apical third of the root. It is largely an age related phenomenon . It may be localised to one tooth or affect entire dentition. Excessive proliferation of cementum may occur in a braod spectrum of neoplastic and non neoplastic conditions. ETIOLOGY Etiology varies and is not completely understood. The spike like type of hypercementosis results from excessive tension from orthodontic appliances or occlusal forcers . The generalised type may be associated with a variety of situations like teeth without antagonists ,in teeth with chronic pulpal and periapical infection. Hypercementosis of the entire dentition may occur in patients with Paget’s disease. ANKYLOSIS Ankylosis refers the fusion of cementum and alveolar bone with obliteration of PDL. It develop after chronic peri apical inflammation,tooth replantation,and occlusal trauma and embedded tooth. Clinically, ankylosed teeth lack the physiological mobility of norrmal teeth. Ankylosed teeth usually have a special metallic percussion sound and if the ankylotic process continues they will be in infraocclusion. CEMENTUM RESORPTION & REPAIR Local condition causing cementum resorption include trauma from occlusion.pressure from malaligned erupting teeth,cysts and tumours,orthodontic movement,periapical diseases,and periodontal diseases. Systemic condition include calcium deficiency,hypothyroidism,hereditary fibrous osteodystrophy and paget’s disease. EXPOSURE OF CEMENTUM TO ORAL ENVIRONMENT Cementum may be exposed to the oral environment in cases of gingival recession and as a result of loss of attachment in pocket formation. In these cases, cementum is permiable to be penetrated by organic substances,inorganic ions and bacteria. Bacterial invasion of the cementum occur frequently in periodontal disease. Cementum caries can also develop.