Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
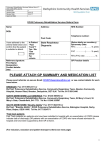
REFERRER CHECK LIST as appropriate New patient Patient already on caseload Past medical history attached Medication list attached Spirometry results attached Last five consultations attached SINGLE POINT OF ACCESS (SPA) DEMOGRAPHICS AND REASON FOR REFERRAL Date of first visit/urgency of visit (as appropriate): Patient name: ………………..…………………………………………….. Title: National Health Service Number (NHS No.) Gender: Male/Female Date of Birth (D.O.B.) Current address: Postcode: Telephone number: Does this patient live alone? City Wide Alarms: Yes/No Special information to access the property: Risks: Key Safe/Door Code: Additional info: Next of kin – Name: Relationship: Ethnicity: Telephone Number: Religion (if known): General Practitioner (GP)/Consultant: Does the next of kin wish to be notified prior to visit: Yes/No First language: Interpreter needed?: GP Telephone Number: GP Fax Number: GP Practice Name/Address: Date last seen by GP: Consent to share information with appropriate service: Yes Reason for referral: Referrer: Print Full Name: Designation: Telephone Number: Please send SPA by fax on 0114-305-1461, or by mail to SPA at Lightwood House, Sheffield, S8 8BG, or phone 0114 305 1460 Version 1.0: May 2013 APPENDIX F: PULMONARY REHABILITATION REFERRAL Patient name: NHS Number/D.O.B: Please state whether patient is being referred for: For Early supported discharge referrals please state date of discharge from hospital : Group Pulmonary Rehabilitation Home based (state reason e.g. housebound/ anxiety) Respiratory diagnosis: Does the patient have chest pain? Yes/No Is the patient aware of their diagnosis? Yes/No If present has the chest pain been investigated? Yes/No GTN used and in date? Previous type II failure? Yes/No Yes/No MRC (Medical Research Council) SCALE (circle as appropriate) Referral criteria is functionally limited breathlessness - usually MRC 3 or above 1. only get breathless with strenuous exercise, 2. get short of breath hurrying on level or uphill, 3. walk slower than people same age or have to stop due to breathlessness, 4. have to stop after a few hundred yards of walk due to breathlessness, 5. too breathless to leave house or get breathless getting dressed/undressed. Previous Pulmonary rehabilitation Yes (when? ……………………..) No Don’t know Does the patient have any serious disability or mobility problems, or severe arthritic limitations to exercise, or other limitations to exercise, e.g. CVA, amputation, etc: YES/NO If Yes, please state limitation: Patient receiving oxygen Long term oxygen therapy? Yes/No therapy (LTOT)? Yes/No Prescription l/min if available Ambulatory oxygen? Yes/No Prescription l/min IF not on LTOT If on LTOT Oxygen saturations on air: Oxygen saturations on LTOT: If available PLEASE COMPLETE FOLLOWING INFORMATION ONLY IF NOT SHARING ON TPP Are there any services already involved with this patient? Past Medical History: Please attach full past medical history Medication: Please attach list of current medications Any known allergies? Latex allergy? Yes/No MRSA status? Positive/Negative/Unknown Pulse: Rhythm: Regular/Irregular Blood pressure: Spirometry: Please attach report if not scanned on TPP: % predicted FEV1: % predicted FVC: Ratio: Please see attached inclusion/ exclusion criteria sheet for reference Please send SPA by fax on 0114-305-1461, or by mail to SPA at Lightwood House, Sheffield, S8 8BG, or phone 0114 305 1460 Version 1.0: May 2013 For enquiries please telephone Active Programmes Team on 0114 305 4200 Pulmonary Rehabilitation Referral Criteria and Exclusion criteria The following are inclusion criteria for pulmonary rehabilitation: *Guidance is given in italics Diagnosed respiratory condition i.e. COPD, Bronchiectasis, Pulmonary Fibrosis. Functionally limited by their disease, usually MRC grade 3 or above. Asthma *may be considered – liaise with team Pre and post lung resection *may be considered –liaise with team Post chest trauma *may be considered –liaise with team The following are exclusion criteria for pulmonary rehabilitation *Guidance is given in italics Unstable Angina Unresolved chest pain Myocardial Infarction within the last 6 weeks *refer to cardiac rehabilitation unless otherwise indicated Severe cardiac arrhythmias or uncontrolled arrhythmias History of supraventricular tachycardia Tachycardia (HR >100) Bradycardia (HR< 60 not betablocked) Uncontrolled heart failure Moderate to severe Heart failure *If Mild/ Moderate heart failure please forward a copy of most recent ECHO report Hypertrophic cardiomyopathy Severe Aortic Stenosis – or if symptomatic at any severity. *If mild/ moderate require confirmation via ECHO within past 6 months and confirmation of safety to exercise from cardiologist. Active endocarditis Aortic aneurysm >5cm *if less than 5cm will need to have had review within past 6 months and confirmation of suitability to exercise from cardiology Uncontrolled medical co morbidities Hypertension >180 systolic / 100 diastolic Hypoxia, Spo2 at rest <92% unless has supplementary oxygen * refer for LTOT assessment as appropriate Cataract surgery within 2 weeks (contact opthalmology if any concerns) Acute, recurrent or suboptimally managed Pulmonary embolism Acute thrombosis of extremity Pulmonary hypertension without confirmation from consultant on safety to exercise. * Need guidelines from consultant for level of acceptable oxygen desaturation on exertion History of cardiac arrest not associated with surgical procedure Cardiac defibrillator insitu *please refer to cardiac rehabilitation LTOT but no ambulatory oxygen * refer for ambulatory oxygen assessment prior to pulmonary rehabilitation referral if LTOT in situ without ambulatory oxygen Syncope Dizziness without investigation Spirometry not done in last 12 months Electrolyte imbalance *please liaise with team Acute confusion Chronic confusion/ memory difficulties without the support of a carer Please send SPA by fax on 0114-305-1461, or by mail to SPA at Lightwood House, Sheffield, S8 8BG, or phone 0114 305 1460 Version 1.0: May 2013