Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
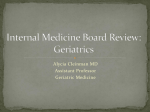
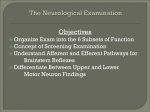
The 2nd International Conference Computational Mechanics and Virtual Engineering COMEC 2007 11 – 13 OCTOBER 2007, Brasov, Romania PROTOCOL FOR GAIT ANALYSIS BASED ON LABORATORY INVESTIGATIONS Mirela Toth-Taşcău, Dan Ioan Stoia, Mircea Dreucean Politehnica University of Timisoara, ROMANIA, [email protected], [email protected], [email protected] Abstract: The present study assigns a protocol for human gait investigations. In order to find a protocol, the gait cycles of a number of 20 healthy patients were recorded. The basic concept was to use three different systems in order to achieve the desired protocol. The protocol idea arises from the necessity to compare a record of a healthy person with a diseased one. The establishing of a normal gait pattern was also a main concern. The recording equipments used are: the human gait analysis system Zebris, the plantar force measurement system Zebris FDM and the electromyography system from ADInstruments. All of these systems are dedicated or can be adapted to our study purpose. The combination of the measurement and investigation concepts of the equipments involved in the study, lead us to a protocol for human gait evaluation. Keywords: kinematical analysis, gait, force distribution, electromyography 1. INTRODUCTION The gait is one of the main abilities of the human body. During a life time, different motion abnormalities can occur. The human lower limb skeleton may be considered a complex system composed of rigid bodies (bones), joints (articulations) and actuators (muscles). According to the complexity of the lower limb construction, the movement capacities at this level are really vast. The gait abnormalities can be caused by problems in bones, joints, muscles, ligaments or nerves. An investigation based on kinematical analysis is not sufficient for a diagnostic. The physicists can add their own medical experience to the results of the gait analyze system in order to define a diagnostic and to evaluate the level of the rehabilitation process. 2. KINEMATICAL GAIT ANALYSIS USING ZEBRIS CMS-HS MEASURING SYSTEM Figure 1: Geometrical model The Zebris measuring system allows an objective kinematical analysis of the human gait by means of analyzing the tracks of body surface markers [4]. The measuring method is based on the determination of spatial coordinates of miniature ultrasound receivers (markers) by measuring the delay between the emission of sonic pulses by the transmitters and their reception at the microphone sensors. The exact spatial position of the markers is determined by triangulation method. The measurement starts with the attachment of the two markers on the body in two key points. The first marker triplet is attached on the thigh and the second one on the upper part of the foot. In the next step, the anatomic 527 landmarks are marked with the pointer, and the dedicated software creates the geometrical model (figure 1). After this point, the recording can start. The steps number was isolated from the large data recorded and used to calculate the velocity, cadence and double support time. In a normal gait, the step time is about 1.3 seconds, but in this case the subject made small and short steps (figure 2). One can say that this parameter is characteristic for the investigated person. Another important parameter is the balance between the gait phases. For a normal gait, the swing phase must be around 40% of the gait cycle and the stance phase 60%. This case underlines an abnormality of the gait, with around 25% of swing and 75% of stance (figure 3). The difference between the left and right limb in gait phases is still insignificant. Figure 3: Swing –Stance phases Figure 2: Step diagram during gait cycles The joint angles recorded during the gait cycle are presented in the figure 4. Figure 4: Angular variation in lower limb joints during a gait cycle The diagram shows the angular variation for each individual joint in all the possible movements: flexion-extension, abduction-adduction and rotations. The flexion-extension movements of the thigh, knee and ankle present the highest 528 amplitudes, with the values included in the normal range for a gait cycle. The diagrams for the left limb joint variations are highlighted in the upper part of the figure 4, and at the bottom of the same figure, the same parameters for the right limb. The angular variations of the left and right limbs prove also, the similitude between the limbs. So, the angular parameters indicate a gait movement close to the normal one. 3. FORCE DISTRIBUTION MAPPING USING ZEBRIS FDM SYSTEM The Zebris FDM measuring system functions using high-quality capacitive force sensors that are arranged in matrix form. The measuring plate enables both the static and dynamic plantar force distribution to be analyzed during the patient standing and walking [5]. In order to compare the resulting gait parameters with the parameters from the first recording method the same subject was investigated. The general parameters indicate a particular type of gait (like in the first case), with large stance periods up to 78% on the right limb, and large stride time of 1.58 sec (a normal gait has a stride time of 1.3 sec). The specific parameter of the system is the plantar pressure distribution. The pressure distribution looks like a colored footprint (tracking). The values of the pressures are provided in N/cm² units and can be identified in comparison with a reference color bare (figure 5). Figure 5: Long platform picture Another specific parameter recorded with FDM system is the reaction force. The reaction forces at the plantar level vary like in the figure 6. The capacitive sensors of the system measure the instantaneous pressure and calculate the force F=P*S (S represents stance for the contact area between foot and platform). The graphic below reveal three major points for the force distribution: peaks, flat middle lines and valleys. The peaks on the graphic correspond to the double support of the limbs at the moment when the first initial heal contact happens. At this moment, the force is greater then the force of gravity because of the small contact area and the inertial forces caused by the movement. The valleys correspond to the double support of the limbs, with a large contact, when one foot is completely on the ground and the other one is in toe-off position. This large contact area explains the low values of the pressure. The flat lines between peaks and valleys indicate a single support. Because the movement is fully generated by the other limb, the forces correspond to a static loading. In this case, the force represents the gravity force of the subject. 529 Figure 6: Variation of the reaction forces during the gait Other parameters provided by this method are presented in the figure 7. The first one, the GLL (gait line length) parameter is the length of the line that describes the course of the pressure center, when only the individual ground contacts of the side of the body are taken into consideration. This parameter comprises the course of the pressure center for all the steps recorded of one by one sides of the body. Figure 7: GGL - Gait line length diagram Figure 8: Steps cyclogram In the steps cyclogram (figure 8), another two parameters are drawn. The SSL-single support line is equivalent to the average length of the lines that describe the course of the pressure center, when all the ground contacts are taken into consideration. The A/PP (anterior/posterior position) parameter describes the shift forwards/backwards of the intersection point of the CoP trajectory in the cyclogram, taking all the steps into consideration. 4. ELECTROMYOGRAPHIC INVESTIGATIONS USING AD INSTRUMENTS SYSTEM In addition to the first two investigations methods, EMG analysis can be used to discern a subtle gait disorder such as muscles or ligaments injuries. Each muscle contraction starts with the excitation of an upper motor neuron (UMN) in the motor cortex of the brain, which travels down the spinal cord to synapse with a lower motor neuron (LMN) in the vertebral horn of the spinal cord (figure 9) [1]. Figure 9: Muscle control: 1 Motor cortex, 2 Upper motor neuron; 3 Spinal cord; 4 Lower motor neuron; 5 Muscle 530 The summation of many bioelectrical signals from all the motor units active at a given time results in electrical activity called electromyogram. This can be picked up over the skin surface over the muscle (EMG), or by percutaneous fine needle electrodes inserted into the muscle belly. The signal recorded by surface electrodes is very small (less than 1mV) so, in order to analyze this, it must be amplified. During gait, different muscle groups are actuated in a certain order to perform skeleton movement. The main muscles groups of the lower limbs are: - iliopsoas, gluteus maximus, and gluteus medius – for hip joint - rectus femoris, adductor longus, vastus lateralis, vastus medialis, and biceps femoris – for knee joint - gastrocnemius, soleus, tibialis anterior, peroneus longus – for ankle joint In order to record and acquire an EMG signal, the ADInstruments measurement system can be used. The system is composed by the PowerLab data acquisition system suitable for a wide range of applications; the Dual Bio Amplifier/Stimulator dedicated to measure a wide variety of biological signals like EEG, ECG, and EMG; the EMG electrodes and Chart 5 software. EMG activity can be recorded using either a monopolar or bipolar recording arrangement. In monopolar recordings, one electrode is placed directly over the muscle and a second electrode is placed at an electrically neutral site, such as a bony prominence. Generally, monopolar signals yield lower frequency responses and less selectivity than bipolar recordings. The monopolar recordings are frequently used during static contractions and in a variety of clinical investigations. Monopolar recordings are appropriate for the assessment of H and T reflex and muscle M waves, however [1], [2]. Bipolar recordings are considerably more common. In a bipolar recording arrangement, two electrodes are placed in the muscle or on the skin overlaying the muscle and a third neural, or ground, electrode placed at an electrically neutral site. The amplitude and frequency spectrum of the EMG signal is affected by the location of the electrode with respect to the innervation zone (figure 10). Figure 10: EMG signals according to the electrode positions Placing the electrodes at the extremity of the muscle (insertion points) the acquired signal has small amplitude. The preferred location is in the midline of the belly of the muscle between the nearest innervation zone and the myotendonous junction. In this location the EMG signal with the greatest amplitude is detected (figure 10). Evaluating the muscular activities of the lower limb by electromyography some typical wave forms can be established (figure 11). a). Thigh muscles group b). Leg muscles group c). Foot muscles group Figure 11: Typically wave forms for the lower limb muscular activity 531 5. CONCLUSIONS The human gait can be successfully evaluated using the presented methods. The three methods succeed to evaluate the gait from three different points of view. First, the investigations using Zebris CMS-HS system leads to a kinematical approach by analyzing the angular variation of each joint. The second investigation method consisting of a force distribution measurement (Zebris FDM system) provides important data about the reaction forces acting at the plantar level. The third investigation succeeds to evaluate the gait from the electrical activity point of view. This last approach was possible using the ADInstruments electromyographic system. Combining the three methods in an investigation of a subject, a diagnostic can be more easily established. The different approaches allow discovering of all the gait abnormalities, helping to correct the problems in initial phase. Methods Kinematical analysis Table 1: Protocol for gait analysis Parameters Joints angles [deg] Double support time [sec] Velocity [cm/sec] Swing time [%] Stance time [%] Force distribution investigation Plantar pressure [N/cm²] Pressure center’s trajectory Gait line length [m] Single support line [m] Anterior/Posterior position [m] Electromyographic investigation Electrical activity of the muscles [mV] Evaluation of the parameters Kinematic parameters of the investigated limb Comparison with reference values Identification of the possible problems Determination of the real plantar pressure distribution Detection of the influences from gait analyze Detection of the influences from spine mobility Formulation of partial conclusions for diagnostic Clarification of suspicions provided by the kinematic analyze Definition of a most probable diagnostic based on multicriterial analyze REFERENCES [1] [2] [3] [4] [5] [6] KIRTLEY C.: Clinical Gait Analysis, theory and practice. Churchill Livingstone Elsevier 2006. GORDON D.E. ROBERTSON et al., Research Methods in Biomechanics, Human Kinetics,USA,2004 FISH D J.; NIELSEN J-P.: Clinical assessment of the human gait. Journal of Prosthetic and Orthotics 1993 *Zebris CMS-HS: Operating Instructions. *Zebris FDM: Operating Instructions. *ADInstruments: Operating Instructions. 532