Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
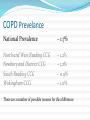
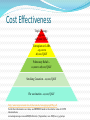
Use COPD: Up to date management and new drugs Catherine Thomas Consultant Respiratory Physician Sanjay Desai and Jillian Powell Medicines Optimisation Team Katy Beckford Respiratory Team Leader Objectives of the session COPD Fact and Figures NICE guidelines Inhaler Update COPD COPD is an obstructive and irreversible lung disease, a combination of emphysema and chronic bronchitis in varying proportions, predominantly caused by cigarette smoking. 3rd commonest cause of death worldwide by 2020 4th commonest cause of death in UK, with ~28,000 deaths Second commonest cause of acute hospital admission Cost to NHS - >£ 800 million in direct healthcare cost Diagnosis History Usually >10 pack yrs and >35y old Cough SOB Sputum production Activity level Exacerbation frequency Smoking status Evidence of cor pulmonale Weight loss – assoc. with poor outcome Diagnosis Diagnosis by spirometry (post bronchodilator) Nice guidelines grade severity on FEV1 FEV1/FVC Ratio <0.7 <0.7 <0.7 <0.7 FEV1 Stage 80% 50-79% 30-49% <30% Mild Moderate Severe Very Severe MRC dyspnoea score 1. Not troubled by breathlessness except on strenuous exercise 2. Short of breath when hurrying or walking up a slight hill 3. Walks slower than contemporaries on the level because of breathlessness, or has to stop for breath when walking at own pace 4. Stops for breath after about 100 m or after a few minutes on the level 5. Too breathless to leave the house, or breathless when dressing or undressing Cat score Assesses the impact of COPD on patients’ health status Score 0-40 Best use for monitoring patients ?3 monthly Exacerbations of COPD ~10% of acute medical admissions National Audit 2014 - 13% mean increase in COPD admissions cf. 2008 1 in 10 die within 90 days, 1/3 readmitted in same time frame National Audit 2014 – IP mortality ~5% One-year mortality ranging from 22% to 43%, and a 2- year mortality of 36 to 49% Treatment of COPD The Facts and Figures In 2013/14 the 4 CCGs in Berkshire West spent £55,437,915.50 on prescribing. How much of this was spent on drugs in the Respiratory chapter of the BNF? £7,376,079.41 (13.3% of total spend) This is £102,520 less than 2012/13 The 5 most costly drugs to the NHS (This data is from August 2013) In 5th Place – Novorapid Insulin - £5.8 million/month In 4th Place – Symbicort 200 Turbohaler - £7.9 million/month In 3rd Place – Seretide 500 Accuhaler - £8.0 million/month In 2nd Place – Tiotropium Handihaler - £12 million/month And in 1st Place Seretide 250 Evohaler £13.1 million/month Approximately £157.2 million/year How do the Berkshire West CCGs compare? Symbicort 200 Turbohaler £70,574/month Spiriva Handihaler £66,555/month Seretide 250 Evohaler £64,853/month Seretide 500 Accuhaler £53,378/month True Result Test Strips £50,834/month (Epact data for first 6 months of 2014/15) COPD Prevelance National Prevalence – 1.7% North and West Reading CCG Newbury and District CCG South Reading CCG Wokingham CCG – 1.2% – 1.2% – 0.9% – 1.0% There are a number of possible reasons for this difference How many COPD patients are there across the 4 Berkshire West CCGs? COPD Register 1600 1400 1200 1000 800 600 400 200 0 Newbury and District CCG North and West Reading CCG South Reading CCG 5201 patients (based on QOF 2013 data) Wokingham CCG What does NICE say? NICE clinical guideline 101: Chronic obstructive pulmonary disease; June 2010 Offer therapy Consider therapy SABA or SAMA as required* Exacerbations or persistent breathlessness FEV1≥50% LABA LAMA** Offer LAMA in preference to regular SAMA qds. Persistent exacerbations or breathlessness LABA + ICS combo Consider LABA+LAMA if ICS declined or not tolerated *SABA as required may continue at all stages FEV1<50% LABA + ICS combo Consider LABA+LAMA if ICS declined or not tolerated LAMA + LABA +ICS **Discontinue SAMA LAMA** Offer LAMA in preference to regular SAMA qds. What does NICE say? All people with COPD who still smoke, regardless of age, should be encouraged to stop, and offered help to do so at every opportunity. Offer pneumococcal vaccination and an annual influenza vaccine as recommended by the Chief Medical Officer Offer pulmonary rehabilitation to all appropriate people with COPD, including those who have had a recent hospitalisation for an exacerbation and those who consider themselves functionally disabled by COPD (usually MRC grade 3 and above) Give people at risk of exacerbations a course of antibiotics and corticosteroid tablets to keep at home. Monitor the use of these drugs and advise people to contact a healthcare professional if their symptoms do not improve. Patients should have a self management plan In the last 12 months there have been a number of new drugs, combinations of treatments and devices introduced in to the market. This makes the picture of COPD treatment more confusing and there are now treatment options without an obvious place on the previous chart e.g. LABA/LAMA combinations. NICE is not due to review the current guidance until June 2016. So how are we doing? Cost Effectiveness Triple Therapy £35,000£187,000/QALY Tiotropium or LABA - £5,000 to £8,000/QALY Pulmonary Rehab – £2,000 to £8,000/QALY Smoking Cessation - £2,000/QALY Flu vaccination - £1,000/QALY http://www.improvement.nhs.uk/documents/managingcopd/SP4.pdf For further information on value, see IMPRESS Guide to the relative value of COPD interventions. www.impressresp.com and BMJ Editorial, 17 September, 2012. BMJ 2012; 345:e6192 The updated cost effectiveness pyramid What do we prescribe? 2013 /14 Spend per Astro PU on the LAMA Agents £800.00 £700.00 £600.00 £500.00 £400.00 £300.00 £200.00 £100.00 £0.00 Tiotropium NEWBURY AND DISTRICT CCG Aclidinium Bromide NORTH & WEST READING CCG SOUTH READING CCG Glycopyrronium Bromide WOKINGHAM CCG BERKSHIRE WEST FEDERATION 2013/14 Spend per Astro PU on the Combined Inhalers used in COPD £900.00 £800.00 £700.00 £600.00 £500.00 £400.00 £300.00 £200.00 £100.00 £0.00 Fostair NEWBURY AND DISTRICT CCG Symbicort NORTH & WEST READING CCG Seretide Evohaler SOUTH READING CCG WOKINGHAM CCG Seretide Accuhaler BERKSHIRE WEST FEDERATION Tiotropium – Spiriva® Antimuscarinic Bronchodilator Licensed for maintenance treatment of COPD For Adults over 18 years of age Handihaler® Dose : 1 inhalation once daily Respimat® Dose : 2 puffs once daily Approved by APC in November 2013 Indacaterol – Onbrez Breezhaler® Long Acting Beta2 Agonist Bronchodilator Black Triangle▼ Licensed for maintenance treatment of COPD For Adults over 18 years of age Dose : 1 inhalation daily, increased to max. 2 inhalations daily Approved by EPC in March 2011 Aclidinium Bromide – Eklira Genuair® Antimuscarinic Bronchodilator Black Triangle▼ Licensed for maintenance treatment of COPD For Adults over 18 years of age Dose : 1 inhalation twice a day Glycopyrronium – Seebri Breezhaler® Antimuscarinic Bronchodilator Black Triangle▼ Licensed for maintenance treatment of COPD For Adults over 18 years of age Dose : 1 capsule once a day APC 024 November 2013 – Both of these agents are only to be used second line after Tiotropium , where there are no cardiovascular contraindications. New local guidelines will be launched soon and this may change the local choices. Fluticasone and Salmeterol – Seretide® Combination of Inhaled Corticosteroid and Long Acting Beta2 Agonist Accuhaler – Licensed for COPD and Asthma From 5 years of age depending on strength Dose : 1 puff twice daily Evohaler – Licensed for Asthma only From 5 years of age depending on strength Dose : 2 puff twice daily Budesonide and Formoterol – Symbicort Turbohaler® Combination of Inhaled Corticosteroid and Long Acting Beta2 Agonist Licensed for COPD and Asthma From 6 years of age, depending on strength and condition Dose : See SPC or BNF. Beclometasone and Formoterol – Fostair® Combination of Inhaled Corticosteroid and Long Acting Beta2 Agonist Licensed for COPD and Asthma From 18 years of age Dose for COPD: 2 puff twice daily Dose for Asthma: 1 or 2 puff twice daily Fluticasone and Formoterol – Flutiform® Combination of Inhaled Corticosteroid and Long Acting Beta2 Agonist Licensed for Asthma only From 12 years of age depending on strength Dose : 2 puff twice daily Some of the new products to enter the market Olodaterol – Striverdi Respimat® Long Acting Beta2 Agonist Bronchodilator Black Triangle▼ Licensed for maintenance treatment of COPD For Adults over 18 years of age Dose : 2 puffs once daily Umeclidimium – Incruse Ellipta® Antimuscarinic Bronchodilator Black Triangle▼ Licensed for maintenance treatment of COPD For Adults over 18 years of age Dose : 1 inhalation daily Vilanterol and Fluticasone – Relvar Ellipta® Combination of Long Acting Beta2 Agonist and Corticosteroid Black Triangle▼ NB. Two strengths available Low strength inhaler (22/92) - Licensed for COPD and Asthma High strength inhaler (22/184) - Licensed for Asthma only From 12 years of age Dose, regardless of strength and indication: 1 inhalation daily APC 080 May 2014 – This agent is not currently recommended Vilanterol and Umeclidinium – Anoro Ellipta® Combination of Long Acting Beta2 Agonist and Corticosteroid Black Triangle▼ Licensed for maintenance treatment of COPD For Adults over 18 years of age Dose : 1 inhalation daily So which inhaler is the most expensive? The one that never gets used or is not used correctly Why not seretide? Cost Risk of pneumonia Non-fatal pneumonia Trials only shown this with Fluticasone TORCH, INSPIRE (64% and 94% increased risk of pneumonia respectively). Mulitple other trials confirm Increased risk with advancing age, lower FEV1, increasing dose of steroid Recent large trial of severe COPD – no effect on disease off combination, decreased risk of pneumonia Trials show no significant increase with budesonide ?Relvar – Increase of approx 50% (3 to 6%) Take Home Messages Check your COPD register - Is it up to date? Check that all COPD patients have a COPD severity Check that rescue packs are on acute and not repeat Check what dose and duration of prednisolone you are issuing for an exacerbation Tiotropium remains the first line LAMA at present but watch out for the launch of the new local guidelines which will incorporate the new agents. Fostair first line for combination inhaler. Check compliance before assuming that a treatment is not working Always encourage the use of a spacer device with an MDI Ensure that inhaler technique is being reviewed at every opportunity Convinced yet that we need training on how to use inhalers? Health Professionals speed of inhalation when asked to inhale as if using an MDI “Slowly and Deeply” Speed of inhalation MDI Inhaler 91 L and above 61 – 90 L/min 60 L/min or less n = 2825 n = 287 Total = 3271 tests conducted : over 94% inhaled too fast n = 179 General Practitioners, Practice Nurses, Respiratory Nurses (Primary & Secondary Care), Pharmacists (Community, Retail and Hospital), Pharmacy Dispensers, Prescribing Advisors, Physiotherapists, Hospital Physicians (General Medicine and Thoracic), Pharmaceutical Company Employees (Representatives, Medical Advisors, Educational Staff) Presented at ERS Annual Scientific Meeting, Stockholm 2007 (No. 91, Primary Care Day, 15/9/07): Jon Bell, Canday Medical Ltd. data collected between 1st June 2006 and 5th September 2007 Asthmatics – Speed of inhalation through Metered Dose Inhaler Speed of inhalation MDI Inhaler 91 L/min and above 90 L/min or less n = 440 n = 36 n = 179 Total = 476 individuals tested: over 92% inhaled too fast Al-Showair R A M , Pearson S B, Chrystyn H. The Potential of a 2Tone Trainer To Help Patients Use Their Metered-Dose Inhalers Chest 2007; 131: 1776-1782 But this is Nationally…. Berkshire West are better than this… aren’t we? We recently put on an Inhaler Training course for BHFT Staff 39 Staff members attended (availability for 60 staff) Consisted of Respiratory Nurses Respiratory Physiotherapists Community Matrons Practice Nurses responsible for COPD Clinics Pharmacists What did we do? Invited Jon Bell (inventor of the InCheck device) to do 3 x 1 hour training sessions. As well as learning about why we need to use inhalers correctly staff were assessed, using the In-Check, to see if they were able to effectively use a Metered Dose Inhaler (MDI) The results are as follows…… Berkshire West Results Clinicans Inhaler Technique <40 L/Min N=4 >40 L/Min N = 35 0 10 20 30 40 Total = 39 tests conducted : over 90% inhaled too fast < 40 L/Min is required for effective inhalation of an MDI How can we improve this? ALL staff need to know how to use inhalers correctly Please do come to the respiratory team in the break to see if you are able to do this Encourage all staff to attend inhaler training courses that are put on (50% under utilised for this event) Refer to the Community Respiratory Team if you are struggling with any patients and wish them to be reviewed. Who are the Respiratory Team and what do they do? Team leader Katy Beckford Respiratory Nurses Martin Weighman Ann McKinnon Caroline Smeeton Respiratory Physiotherapists Cath Darby Alexandra Christie Maria Nogueira Heather Yuille Marc Bowen – Physiotherapist Assistant Admin Lisa McCreery What we can offer Supportive discharges (all patients who have had an admission for COPD exacerbation) 2hr Rapid Response service with the aim of preventing unnecessary or unplanned admissions Education and advice for patients and clinicians MDT education and attend GP meetings Pulmonary Rehabilitation 6 Month and Annual review of patients on Home Oxygen Smoking Cessation Telehealth How do you refer to us? All referrals are taken via the Health Hub Telephone 0300 365 1234 Fax 0300 365 0400 Email: [email protected] What do we need? All we require is that a patient has a confirmed diagnosis. With the referral we require Patient Summary Most recent Spirometry Why the patient needs to be seen How soon the patient needs to be seen How can we improve in Berkshire West? Earlier referral to the CRT All suitable patients to have back up antibiotics and steroids Referring to the CRT after 1 week if no improvement on treatment All patients with an MRC 3> should have a PR referral What to do next… Smoking cessation Pulmonary rehabilitation – re-offer if done already, particularly post exacerbation/admission to aid recovery Influenza vaccination, pneumococcal vaccination Check inhalers - correct for spirometry, can use? Consider dietician – Low BMI associated with inc. mortality Rescue pack Self management plan Carbocisteine – 750mg tds Theophylline Steroid enhancing effects even at low dose Discharge Checklist Faxed to practice Activity level, sputum, discharge saturations Inhaler technique Smoking cessation Pulmonary rehab Rescue pack Community COPD team referral (seen within 2 weeks post discharge) Respiratory CNS call at 48h to check patient When to refer Unsure of diagnosis Young patients Severe COPD Rapid decline in FEV1 Frequent exacerbators (>2 per year) Evidence from COPD cohorts suggest ~30% have bronchiectasis and managed as such Evidence of complications – cor pulmonale, weight loss, haemoptysis What might we do… PDE4 inhibitors - Roflulimast / Rolipram – not used Azithromycin Used in trials for between 8 weeks to 1 yr in frequent exacerbators Reduces exacerbation rate and time to next hospitalization Risks of resistance? Assessment for LTOT Severe COPD, Sats <92%, cor pulmonale, polycythaemia Two ABG’s at least 3/52 apart in stable COPD Also ambulatory oxygen NIV End of life care What might we do Consider surgical therapies LVRS endobronchial treatment (valves/coils) Endobronchial valves Full lung function criteria Reasonable performance status Heterogeneous emphysema on scans High flow oxygen, significant PH contra-indications Coils Homogenous emphysema Still only at trial stage For listening! Useful websites and resources Chronic obstructive pulmonary disease (updated) (CG101) http://www.nice.org.uk/cg101 An Outcomes Strategy for Chronic Obstructive Pulmonary Disease (COPD) and Asthma in England https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/2161 39/dh_128428.pdf Interactive Health Atlas for Lung Conditions in England http://www.inhale.nhs.uk/ Summary of Product Characteristics for all drugs and devices http://www.medicines.org.uk/emc/ Medicines Optimisation Team generic email address [email protected]