Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Maternal rubella and the congenital rubella syndrome
The major goal of rubella immunization is the prevention of the congenital rubella
syndrome. As many as 20 per cent of women in the reproductive age group in the United
States continue to be susceptible to rubella despite the immunization programs currently
in place. Intensified efforts are therefore needed to identify persons at risk for infection
and to vaccinate them. Women who develop a rubella-like illness during pregnancy
should have the diagnosis confirmed serologically because a diagnosis based on clinical
criteria alone is unreliable and because of the serious implications of gestational rubella
infection. The rubella virus can infect the fetus at any stage of pregnancy, but defects are
rarely noted when this occurs after the 16th week of gestation. The most common
abnormalities in the congenital rubella syndrome are hearing loss, mental retardation,
cardiac malformations, and eye defects. Diabetes mellitus, thyroid disease, glaucoma, and
other delayed manifestations of congenital rubella syndrome are common, thereby
necessitating long-term followup of these patients. The detection of rubella-specific IgM
antibodies in fetal blood is helpful in establishing the diagnosis prenatally and can aid in
the management of pregnancies complicated by this infection. Susceptible women
identified through screening during pregnancy should be immunized in the immediate
postpartum or postabortion period. Although the live, attenuated rubella vaccine is
contraindicated during pregnancy, pregnant women who are inadvertently immunized are
not candidates for pregnancy termination because no defects consistent with congenital
rubella have been reported to date in the offspring of other similarly vaccinated women.
Rubella can cause congenital rubella syndrome in the newly born. The syndrome
(CRS) follows intrauterine infection by Rubella virus and comprises cardiac, cerebral,
ophthalmic and auditory defects. It may also cause prematurity, low birth weight, and
neonatal thrombocytopenia, anaemia and hepatitis. The risk of major defects or
organogenesis is highest for infection in the first trimester. CRS is the main reason a
vaccine for rubella was developed. Many mothers who contract rubella within the first
critical trimester either have a miscarriage or a still born baby. If the baby survives the
infection, it can be born with severe heart disorders (PDA being the most common),
blindness, deafness, or other life threatening organ disorders. The skin manifestations are
called "blueberry muffin lesions."
Cause:
Main article: Rubella virus
The disease is caused by Rubella virus, a togavirus that is enveloped and has a
single-stranded RNA genome. The virus is transmitted by the respiratory route and
replicates in the nasopharynx and lymph nodes. The virus is found in the blood 5 to 7
days after infection and spreads throughout the body. The virus has teratogenic properties
and is capable of crossing the placenta and infecting the fetus where it stops cells from
developing or destroys them.
Increased susceptibility to infection might be inherited as there is some indication
that HLA-A1 or factors surrounding A1 on extended haplotypes are involved in virus
infection or non-resolution of the disease.
Diagnosis:
Rubella virus specific Ig M antibodies are present in people recently infected by
Rubella virus but these antibodies can persist for over a year and a positive test result
needs to be interpreted with caution. The presence of these antibodies along with, or a
short time after, the characteristic rash confirms the diagnosis.
Prevention:
Rubella infections are prevented by active immunisation programs using live,
disabled virus vaccines. Two live attenuated virus vaccines, RA 27/3 and Cendehill
strains, were effective in the prevention of adult disease. However their use in
prepubertile females did not produce a significant fall in the overall incidence rate of
CRS in the UK. Reductions were only achieved by immunisation of all children.
The vaccine is now usually given as part of the MMR vaccine.
The WHO recommends the first dose is given at 12 to 18 months of age with a second
dose at 36 months. Pregnant women are usually tested for immunity to rubella early on.
Women found to be susceptible are not vaccinated until after the baby is born because the
vaccine contains live virus.
The immunisation program has been quite successful. Cuba declared the disease
eliminated in the 1990s, and in 2004 the Centers for Disease Control and
Prevention announced that both the congenital and acquired forms of rubella had been
eliminated from the United States.
Treatment:
There is no specific treatment for Rubella; however, management is a matter of
responding to symptoms to diminish discomfort. Treatment of newly born babies is
focused on management of the complications. Congenital heart defects[citation
needed] and cataracts can be corrected by direct surgery. Management for ocular CRS is
similar to that for age-related macular degeneration, including counseling, regular
monitoring, and the provision of low vision devices, if required.
Prognosis:
Rubella infection of children and adults is usually mild, self-limiting and often
asymptomatic. The prognosis in children born with CRS is poor.
Signs and symptoms:
After an incubation period of 14–21 days, German measles causes symptoms that
are similar to the flu. The primary symptom of rubella virus infection is the appearance of
a rash (exanthem) on the face which spreads to the trunk and limbs and usually fades
after three days (that is why it is often referred to as three-day measles). The facial rash
usually clears as it spreads to other parts of the body. Other symptoms include low grade
fever, swollen glands (sub occipital & posterior cervical lymphadenopathy), joint pains,
headache and conjunctivitis.[6] The swollen glands or lymph nodes can persist for up to a
week and the fever rarely rises above 38 degree C (100.4 degree F). The rash of German
measles is typically pink or light red. The rash causes itching and often lasts for about
three days. The rash disappears after a few days with no staining or peeling of the skin.
When the rash clears up, the patient may notice that his skin sheds in very small flakes
wherever the rash covered it. Forchheimer's sign occurs in 20% of cases, and is
characterized by small, red papules on the area of the soft palate.
Rubella can affect anyone of any age and is generally a mild disease, rare in
infants or those over the age of 40. The older the person is the more severe the symptoms
are likely to be. Up to two-thirds of older girls or women experience joint pain or arthritic
type symptoms with rubella. The virus is contracted through the respiratory tract and has
an incubation period of 2 to 3 weeks. During this incubation period, the patient is
contagious typically for about one week before he develops a rash and for about one
week thereafter.
Crouzon syndrome
Crouzon syndrome is a genetic disorder known as a branchial arch syndrome.
Specifically, this syndrome affects the first branchial (or pharyngeal) arch, which is the
precursor of themaxilla and mandible. Since the branchial arches are important
developmental features in a growing embryo, disturbances in their development create
lasting and widespread effects
Causes:
Associations with mutations in the genes of FGFR2[3] and FGFR3[4] have been
identified.
Symptoms:
As a very complicating result of the changes to the developing embryo, the
symptoms are very pronounced features, especially in the facial areas. Low-set ears is a
typical characteristic, as in all of the disorders which are called branchial arch syndromes.
The reason for this abnormality is that ears on a fetus are much lower than those on an
adult. During normal development, the ears "travel" upward on the head; however, in
Crouzon patients, this pattern of development is disrupted. Ear canal malformations are
extremely common, generally resulting in some hearing loss. In particularly severe
cases, Ménière's disease may occur.
The most notable characteristic of Crouzon syndrome is cranial synostosis, as
described above, but it usually presents as brachycephaly, which results in the appearance
of a short and broad head. Exophthalmos (bulging eyes due to shallow eye sockets after
early fusion of surrounding bones), hypertelorism (greater than normal distance between
the eyes), and psittichorhina (beak-like nose) are also symptoms. Additionally, a common
occurrence is external strabismus, which can be thought of as opposite from the eye
position found in Down syndrome. Lastly, hypoplastic maxilla (insufficient growth of the
midface) results in relative mandibular prognathism (chin appears to protrude despite
normal growth of mandible) and gives the effect of the patient having a concave face.
For reasons that are not entirely clear, most Crouzon patients also have noticeably
shorter humerus and femur bones, in proportion to the rest of their bodies, than members
of the general population. A small percentage of Crouzon patients also have what is
called "Type II" Crouzon syndrome, distinguished by partial syndactyly.
Incidence:
Incidence of Crouzon syndrome is currently estimated to occur in 1 out of every
25,000 people out of the general population.[citation needed]There is a greater frequency
in families with a history of the disorder, but that doesn't mean that everyone in the
family is affected (as referred to above).
Management:
A child with Crouzon syndrome wearing a corrective cranial band.
Surgery is typically used to prevent the closure of sutures of the skull from
damaging the brain's development. Without surgery, blindness and mental retardation are
typical outcomes. Craniofacial surgery is a discipline of plastic surgery. To move the
orbits forward, plastic surgeons work with neurosurgeons to expose the skull and orbits
and reshape the bone. To treat the midface deficiency, plastic surgeons can move the
lower orbit and midface bones forward (this does not need neurosurgical assistance). For
jaw surgery, either plastic surgeons have experience to perform these operations. It is rare
to wear a custom-fitted helmet (or cranial band) for several months after surgery as that is
only for single-suture "strip craniectomy" repair. Crouzon patients tend to have multiple
sutures involved, most specifically bilateral coronal craniosynostoses, therefore an open
operation is used rather than the strip craniectomy with helmeting.
Once treated for the cranial vault symptoms, Crouzon patients generally go on to
live a normal lifespan.
Dental significance:
For dentists, this disorder is important to understand since many of the physical
abnormalities are present in the head, and particularly the oral cavity. Common features
are a narrow/high-arched palate, posterior bilateral crossbite, hypodontia (missing some
teeth), and increased spacing between teeth. Due to maxillary hypoplasia, Crouzon
patients generally have a considerable permanent underbite and subsequently cannot
chew using their incisors. For this reason, Crouzon patients sometimes eat in an unusual
way--eating fried chicken with a fork, for example, or breaking off pieces of a sandwich
rather than taking a bite in it.
Background:
In 1912, Crouzon described the hereditary syndrome of craniofacial dysostosis in
a mother and son. He described the triad of calvarial deformities, facial anomalies, and
exophthalmos.
Crouzon syndrome is an autosomal dominant disorder with complete penetrance
and variable expressivity.1 It is characterized by premature closure of calvarial and
cranial base sutures as well as those of the orbit and maxillary complex
(craniosynostosis).
Other clinical features include hypertelorism, exophthalmos, strabismus, beaked
nose, short upper lip, hypoplastic maxilla, and relative mandibular prognathism. Unlike
some other forms of autosomal dominant craniosynostosis, no digital abnormalities are
present.
Pathophysiology:
Crouzon syndrome is caused by mutations in the fibroblast growth factor
receptor-2 (FGFR2) gene but exhibits locus heterogeneity with causal mutations
in FGFR2 (Crouzon syndrome) and FGFR3 (Crouzon syndrome with acanthosis
nigricans) in different affected individuals.
Premature synostosis of the coronal, the sagittal, and, occasionally, the
lambdoidal sutures begins in the first year of life and is completed by the second or third
year. The order and rate of suture fusion determine the degree of deformity and disability.
Once a suture becomes fused, growth perpendicular to that suture becomes restricted, and
the fused bones act as a single bony structure. Compensatory growth occurs at the
remaining open sutures to allow continued brain growth. However, multiple sutural
synostoses frequently extend to premature fusion of the skull base sutures, causing
midfacial hypoplasia, shallow orbits, a foreshortened nasal dorsum, maxillary hypoplasia,
and occasional upper airway obstruction.
Rubinstein-Taybi Syndrome
Rubinstein-Taybi Syndrome (RTS; also known as Broad Thumb-Hallux
syndrome) is a condition characterized by short stature, moderate to severe learning
difficulties, distinctive facial features, and broad thumbs and first toes. Other features of
the disorder vary among affected individuals. People with this condition have an
increased risk of developing noncancerous and cancerous tumors, leukemia,
and lymphoma. This condition is inherited in an autosomal dominant pattern and is
uncommon, occurring in an estimated 1 in 125,000 births.
Typical features of the disorder include:
Broad thumbs and broad first toes
Mental disability
Small height, bone growth, small head
Cryptorchidism in males
Unusual faces involving the eyes, nose, and palate
A 2009 study found that children with RTS were more likely to be overweight
and to have a short attention span, motor stereotypies, and poor coordination, and
hypothesized that the identified CREBBP gene impaired motor skills learning.[3]
Mutations in the CREBBP gene cause Rubinstein–Taybi syndrome.[4] The
CREBBP gene makes a protein that helps control the activity of many other genes. The
protein, called CREB-binding protein, plays an important role in regulating cell
growth and division and is essential for normalfetal development. If one copy of the
CREBBP gene is deleted or mutated, cells make only half of the normal amount of CREB
binding protein. A reduction in the amount of this protein disrupts normal development
before and after birth, leading to the signs and symptoms of Rubinstein–Taybi syndrome.
Mutations in the EP300 gene are responsible for a small percentage of cases of
Rubinstein–Taybi syndrome. These mutations result in the loss of one copy of the gene in
each cell, which reduces the amount of p300 protein by half. Some mutations lead to the
production of a very short, nonfunctional version of the p300 protein, while others
prevent one copy of the gene from making any protein at all. Although researchers do not
know how a reduction in the amount of p300 protein leads to the specific features of
Rubinstein–Taybi syndrome, it is clear that the loss of one copy of the EP300 gene
disrupts normal development. 1 out of 100.000 to 125.000 children are born with RTS
Conradi–Hünermann syndrome
Conradi–Hünermann syndrome (also known as "Conradi–Hünermann–Happle
syndrome", "Happle syndrome," and "X-linked dominant chondrodysplasia punctata") is
a type of chondrodysplasia punctata. It is associated with the gene EBP (gene) and affects
between one in 100,000 and one in 200,000 babies.
Conradi-Hunermann syndrome is a form of chondrodysplasia punctata, a group of
rare genetic disorders of skeletal development involving abnormal accumulations of
calcium salts within the growing ends of long bones. Conradi-Hunermann syndrome is
commonly associated with mild to moderate growth deficiency, disproportionate
shortening of long bones, particularly those of the upper arms and the thigh bones, short
stature, and/or curvature of the spine. In rare cases, mental retardation may also be
present. While evidence suggests that Conradi-Hunermann syndrome predominantly
occurs in females and is usually inherited as an X-linked dominant trait, rare cases in
which males were affected have also been reported.
Genetics:
The genetics of Conradi-Hunermann syndrome has perplexed
medical geneticists, pediatricians and dermatologists for some time, but a number of
perplexing features of the genetics of the syndrome have now been resolved, including
the fact that the disease is caused bymutations in a gene, and these mutations are simple
substitutions, deletions or insertions and are therefore not "unstable". Scientists are still
trying to understand exactly where the mutation occurs so that they can correct it.
Symptoms:
Possible symptoms include
Growth deficiency,
Low nasal bridge,
Flat face,
Down-slanting space between eyelids,
Cataracts,
Asymmetric limb shortness,
Joint shortening or spasms,
Frequent scoliosis,
Abnormal redness of the skin,
Thick scales on infant skin,
Large skin pores,
Flaky Skin,
Sparse hair,
Coarse hair, and
Bald spots.
It is associated with use of warfarin
Management:
Treatment can involve operations to lengthen the leg bones, which involves many
visits to the hospital. Other symptoms can be treated with medicine or surgery. Most
female patients with the syndrome to it can live a long and normal life, while males have
only survived in rare cases.
Hypoplastic left heart syndrome
Hypoplastic left heart syndrome (also known as HLHS), is a rare congenital heart
defect in which the left side of the heart is severely underdeveloped.
Causes:
If part of the endocardial tube gets pinched shut in a region that becomes the
future ventricle, hypoplastic heart syndrome will occur. If the pinched part of the
endocardial tube is the bulbus-cordis region of the developing heart, hypoplastic RIGHT
syndrome will occur. If it is in the ventricle region it will be the LEFT side that is
hypoplastic. There is evidence associating it with Gap junction protein, alpha 1.
Clinical Presentation:
In babies with HLHS, the aorta and left ventricle are very small, and
the aortic and mitral valves are either too small to allow sufficient blood flow or are
atretic (closed) altogether. As blood returns from the lungs to the left atrium, it must pass
through an atrial septal defect to the right side of the heart.
In a healthy human, the left side of the heart receives oxygen-rich blood from the
lungs and pumps it out to the rest of the body; with these structures underdeveloped, they
cannot circulate blood to other organs, and the right ventricle must pump blood to both
the lungs, as it would normally, and to the rest of the body, a situation which cannot be
sustained for long.
In cases of HLHS, the right side of the heart often must pump blood to the body
through a patent ductus arteriosus. As the ductus arteriosus usually closes within eleven
days after birth, blood flow is severely restricted and eventually cutoff, leading to
dangerously low circulation and eventually to shock.
Management:
Without life-prolonging interventions, HLHS is fatal, but with intervention, an
infant may survive. A pediatric cardiothoracic surgeon may perform a series of
operations or a full heart transplant. In the meantime, the ductus may be kept open to
allow blood-flow using medication containing prostaglandin. Because these operations
are complex and need to be individualized for each patient, a cardiologist must assess all
medical and surgical options on a case-by-case basis.
While infants successfully treated for HLHS have a good chance of survival, they
may experience chronic health problems for the rest of their lives. The 3-stage surgeries
were developed in the early 1980s with no survivors prior to that time. Therefore, the
earliest survivors are in their mid 20s and the long term prognosis is unknown. However,
the advances in surgical and medical techniques have helped increase the survival rate
dramatically since the surgeries were first developed.
As is true for patients with other types of heart defects involving malformed
valves, HLHS patients run a high risk of endocarditis, and must be monitored by a
cardiologist for the rest of their lives to check on their heart function.
The three stage Norwood procedure only increases the life of the heart as HLHS
cannot be cured. The child may need a heart transplant at some point in the child's
lifetime.
Eisenmenger Syndrome
Eisenmenger syndrome (or Eisenmenger's reaction) is defined as the process in
which aleft-to-right shunt caused by a congenital heart defect causes increased flow
through the pulmonary vasculature, causing pulmonary hypertension, which in turn,
causes increased pressures in the right side of the heart and reversal of the shunt into
a right-to-left shunt.In adults, the most common causes of cyanotic congenital heart
disease are Eisenmenger syndrome and tetralogy of Fallot. Eisenmenger's syndrome
specifically refers to the combination of systemic-to-pulmonary communication,
pulmonary vascular disease and cyanosis. It can cause serious complications
in pregnancy, though successful delivery has been reported
Pathophysiology:
Eisenmenger syndrome occurs in patients with large congenital cardiac or
surgically created extracardiac left-to-right shunts. These shunts initially cause increased
pulmonary blood flow. Subsequently, usually before puberty, pulmonary vascular disease
causes pulmonary hypertension, ultimately resulting in reversed or bidirectional shunt
flow with variable degrees of cyanosis.
Pathogenesis:
The larger, more muscular, left side of the heart generates the higher pressures
required to supply blood to the whole body. The smaller, right side of the heart generates
the lower pressure required to circulate blood solely through the lungs. If a large
anatomic defect exists between the two sides of the heart, blood will flow from the left
side to the right side. This results in high blood flow and pressure travelling through the
lungs. The increased pressure causes damage to delicate capillaries, which then are
replaced with scar tissue. Scar tissue does not contribute to oxygen transfer, therefore
decreasing the useful volume of the pulmonary vasculature. The scar tissue also provides
less flexibility than normal lung tissue, causing further increases in blood pressure, and
the heart must pump harder to continue supplying the lungs, leading to damage of more
capillaries.
The reduction in oxygen transfer reduces oxygen saturation in the blood, leading
to increased production of red blood cells in an attempt to bring the oxygen saturation up.
The excess of red blood cells is called Erythrocytosis. Desperate for enough circulating
oxygen, the body begins to dump immature red cells into the blood stream. Immature red
cells are not as efficient at carrying oxygen as mature red cells, and they are less flexible,
less able to easily squeeze through tiny capillaries in the lungs, and so contribute to death
of pulmonary capillary beds. The increase in red blood cells also causes hyperviscosity
syndrome.
A person with Eisenmenger syndrome is paradoxically subject to the possibility
of both uncontrolled bleeding due to damaged capillaries and high pressure, and random
clots due to hyperviscosity and stasis of blood.
Eventually, due to increased resistance, pulmonary pressures may increase
sufficiently to cause a reversal of blood flow, so blood begins to travel from the right side
of the heart to the left side, and the body is supplied with deoxygenated blood, leading
to cyanosis and resultant organ damage.
Signs and Symptoms:
Signs and symptoms of Eisenmenger syndrome include:
Cyanosis, a blue tinge to the skin resulting from lack of oxygen
High red blood cell count
Swollen or clubbed finger tips(clubbing)
Fainting, called syncope
Heart failure
Arrhythmia or irregular heart rhythms
Bleeding disorders
Coughing up blood
Iron deficiency
Kidney problems
Stroke
Gout, rare, due to increased uric acid resorption and production with impaired
excretion
Gallstones
DiGeorge syndrome
DiGeorge syndrome, (DGS) 22q11.2 deletion syndrome,, DiGeorge
anomaly,[2][3] velo-cardio-facial syndrome, Shprintzen syndrome, conotruncal anomaly
face syndrome, Strong syndrome, congenital thymic aplasia, andthymic hypoplasia is a
syndrome caused by the deletion of a small piece of chromosome 22. The deletion occurs
near the middle of the chromosome at a location designated q11.2 i.e., on the long arm of
one of the pair of chromosomes 22. It has a prevalence estimated at 1:4000.[4]The
syndrome was described in 1968 by the pediatric endocrinologist Angelo DiGeorge.
The features of this syndrome vary widely, even among members of the same
family, and affect many parts of the body. Characteristic signs and symptoms may
include birth defects such as congenital heart disease, defects in the palate, most
commonly related to neuromuscular problems with closure (velo-pharyngeal
insufficiency), learning disabilities, mild differences in facial features, and
recurrent infections. Infections are common in children due to problems with the immune
system's T-cell mediated response that in some patients is due to an absent
or hypoplastic thymus. 22q11.2 deletion syndrome may be first spotted when an affected
newborn has heart defects or convulsions from hypocalcemia due to
malfunctioning parathyroid glands and low levels of parathyroid hormone
(parathormone). Affected individuals may also have any other kind of birth defect
including kidney abnormalities and significant feeding difficulties as
babies. Autoimmune disorders such
is hypothyroidism and hypoparathyroidism or thrombocytopenia (low platelet levels),
and psychiatric illnesses are common late-occurring features. Microdeletions in
chromosomal region 22q11.2 are associated with a 20 to 30-fold increased risk
of schizophrenia.
Studies provide various rates of 22q11.2 deletion syndrome in schizophrenia,
ranging from 0.5 to 2% and averaging about 1%, compared with the overall estimated
0.025% risk of the 22q11.2 deletion syndrome in the general population.
Salient features can be summarized using the mnemonic CATCH-22 to describe
DiGeorge's syndrome, with the 22 to remind one the chromosomal abmormality is found
on the 22 chromosome, as below:
Cardiac Abnormality (especially tetralogy of Fallot)
Abnormal facies
Thymic aplasia
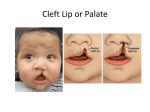
Cleft palate
Hypocalcemia.
Individuals with a 22q11.2 deletion can suffer from many possible features,
ranging in number of associated features and from the mild to the very serious.
Symptoms shown to be common include:
Congenital heart disease (40% of individuals),
particularly conotruncal malformations (tetralogy of Fallot, interrupted aortic
arch, ventricular septal defect, and persistent truncus arteriosus)
palatal abnormalities (50%), particularly velopharyngeal incompetence (VPI),
submucosal cleft palate, and cleft palate; characteristic facial features (present in the
majority of Caucasian individuals) including hypertelorism.
learning difficulties (90%) but broad range
hypocalcemia (50%)(due to hypoparathyroidism)
significant feeding problems (30%)
renal anomalies (37%)
hearing loss (both conductive and sensorineural) (Hearing loss with craniofacial
syndromes)
laryngotracheoesophageal anomalies
Growth hormone deficiency
Autoimmune disorders
Seizures (without hypocalcemia)
Skeletal abnormalities
Cause:
The syndrome is caused by genetic deletions (loss of a small part of the genetic
material) found on the long arm of one of the two 22nd chromosomes. Very rarely,
patients with somewhat similar clinical features may have deletions on the short arm of
chromosome 10.
The mechanism that causes all of the associated features of the syndrome is
unknown. 22q11.2 deletion syndrome may involve migration defects of neural crestderived tissues, particularly affecting development of the third and fourth branchial
pouches (pharyngeal pouches). This affects the thymus gland; a mediastinal organ largely
responsible for differentiation and induction of tolerance in T-cells, and the Parathyroid
glands, responsible for regulation of blood calcium levels.
Management:
There is no cure for 22q11.2 deletion syndrome. Certain individual features are
treatable using standard treatments. The key is to identify each of the associated features
and manage each using the best available treatments.
For example, in children it is important that the immune problems are identified
early as special precautions are required regarding blood transfusion and immunisation
with live vaccines. Thymus transplantation can be used to address absence of the thymus
in the rare, so-called "complete" DiGeorge syndrome.[12] Bacterial infections are treated
with antibiotics. Cardiac surgery is often required for congenital heart abnormalities.
Hypoparathyroidism causing hypocalcaemia often requires lifelong vitamin D and
calcium supplements.
Alagille syndrome
Alagille syndrome is a genetic disorder that affects the liver, heart, kidney, and
other systems of the body. Problems associated with the disorder generally become
evident in infancy or early childhood. The disorder is inherited in an autosomal
dominant pattern, and the estimated prevalence of Alagille syndrome is 1 in every
100,000 live births.
Pathophysiology:
Microdeletion of the 20p12 gene corresponding to JAG1 results in Alagille
syndrome, similar to the inheritance pattern of Williams syndrome.[3] The JAG1 gene is
involved in signaling between adjacent cells during embryonic development. This
signaling influences how the cells are used to build body structures in the
developing embryo. Mutations in JAG1 disrupt the signaling pathway, causing errors in
development, especially of the heart, bile ducts in the liver, spinal column, and certain
facial features.
NOTCH2 is also associated with Alagille syndrome.[4]
Narrowed and malformed bile ducts in the liver produce many of the health
problems associated with Alagille syndrome. Bile is produced in the liver and moves
through the bile ducts into the small intestine, where it helps to digest fat. In Alagille
syndrome, the bile builds up in the liver and causes scarring that prevents the liver from
working properly to eliminate wastes from the bloodstream.
Clinical Presentation:
The severity of the disorder can vary within the same family, with symptoms
ranging from so mild as to go unnoticed to severe heart and/or liver disease
requiring transplantation.
Signs and symptoms arising from liver damage in Alagille syndrome may include
a yellowish tinge in the skin and the whites of the eyes (jaundice), itching, and deposits
of cholesterol in the skin (xanthomas). A liver biopsy may indicate too few bile
ducts (bile duct paucity). Other signs of Alagille syndrome include congenital heart
problems, particularly Tetralogy of Fallot, and an unusual butterfly shape of the bones of
the spinal column that can be seen in an x-ray. Many people with Alagille syndrome have
similar facial features, including a broad, prominent forehead, deep-set eyes, and a small
pointed chin. The kidneys and central nervous system may also be affected.
Genetics:
This condition is inherited in an autosomal dominant pattern, which means one
copy of the altered gene is sufficient to cause the disorder. In some cases, an affected
person inherits the mutation from one affected parent. Other cases may result from new
mutations in the gene. These cases occur in people with no history of the disorder in their
family.
Management:
There is no known cure for Alagille's Syndrome. Most of the treatments available
are aimed at improving the functioning of the heart, and reducing the effects of impaired
liver function.
Corrective surgery is sometimes needed to repair heart defects associated with
Allagile's Syndrome. Also, because the pulmonary arteries are often narrow in Alagilles
patients, a catheterization process similar to angioplasty may be used to widen the arteries
to reduce pressure on the heart's pumping valves. In moderate to severe cases, stents may
be placed in the arteries to increase their diameter. Transplantation of the liver has been a
successful alternative to medication in severe cases.
Recently, a procedure called partial biliary diversion has been used to
significantly reduce pruritus, jaundice, and xanthomas caused by poor bile flow. A
portion of the bile produced by the liver is directed through a surgically
created stoma into a plastic pouch on the patient's lower right abdomen. The pouch is
periodically drained as it fills with bile.
Marfan syndrome
Marfan syndrome (also called Marfan's syndrome) is a genetic disorder of
the connective tissue. People with Marfan's tend to be unusually tall, with long limbs and
long, thin fingers.
It is sometimes inherited as a dominant trait. It is carried by a gene called FBN1,
which encodes a connective protein called fibrillin-1. People have a pair of FBN1 genes.
Because it isdominant, people who have inherited one affected FBN1 gene from either
parent will have Marfan's.
This syndrome has a range of expressions, from mild to severe. The most serious
complications are defects of the heart valves and aorta. It may also affect the lungs, eyes,
the dural sac surrounding the spinal cord, skeleton and the hard palate.
In addition to being a connective protein that forms the structural support for
tissues outside the cell, the normal fibrillin-1 protein binds to another
protein, transforming growth factor beta (TGF-β). TGF-β has deleterious effects on
vascular smooth muscle development and the integrity of the extracellular matrix.
Researchers now believe that secondary to mutated fibrillin there is excessive TGF-β at
the lungs, heart valves, and aorta, and this weakens the tissues and causes the features of
Marfan syndrome. Since angiotensin II receptor blockers (ARBs) also reduce TGF-β,
they have tested this by giving ARBs (losartan, etc.) to a small sample of young, severely
affected Marfan syndrome patients. In some patients, the growth of the aorta was indeed
reduced.
Signs and symptoms:
Although there are no unique signs or symptoms of Marfan syndrome, the
constellation of long limbs, the dislocated lenses, and the aortic root dilation are
sufficient to make the diagnosis with confidence. There are more than 30 other clinical
features that are variably associated with the syndrome, most involving the skeleton, skin,
and joints. There is a great deal of clinical variability even within families that carry the
identical mutation.
The body systems most often affected by Marfan syndrome are:
Skeleton
Eyes
Heart and blood vessels (cardiovascular system
Nervous system
Skin
Lungs
Cardiovascular system
The most serious signs and symptoms associated with Marfan syndrome involve
the cardiovascular system. Undue fatigue, shortness of breath, heart palpitations, racing
heartbeats, or Angina pectoris with pain radiating to the back, shoulder, or arm. Cold
arms, hands and feet can also be linked to Marfan's syndrome because of inadequate
circulation. A heart murmur, abnormal reading on an EKG, or symptoms of angina can
indicate further investigation. The signs of regurgitation from prolapse of the mitral or
aortic valves (which control the flow of blood through the heart) result from cystic medial
degeneration of the valves, which is commonly associated with Marfan's syndrome
(see mitral valve prolapse, aortic regurgitation). However, the major sign that would lead
a doctor to consider an underlying condition is a dilated aorta or an aortic aneurysm.
Sometimes, no heart problems are apparent until the weakening of the connective tissue
(cystic medial degeneration) in the ascending aorta causes an aortic aneurysm or aortic
dissection, a surgical emergency. An aortic dissection is most often fatal and presents
with pain radiating down the back, giving a tearing sensation.
Because of the underlying connective tissue abnormalities that cause Marfan
syndrome, there is an increased incidence of dehiscence of prosthetic mitral
valve.[10] Care should be taken to attempt repair of damaged heart valves rather than
replacement.
During pregnancy, even in the absence of preconceived cardiovascular
abnormality, women with Marfan syndrome are at significant risk ofaortic dissection,
which is often fatal even when rapidly treated. For this reason, women with Marfan
syndrome should receive a thorough assessment prior to conception,
and echocardiography should be performed every six to ten weeks during pregnancy, to
assess the aortic root diameter. For most women, safe vaginal delivery is possible
Pathogenesis:
Marfan syndrome is caused by mutations in the FBN1 gene on chromosome
15, which encodes a glycoprotein called fibrillin-1, a component of the extracellular
matrix. The Fibrillin 1 protein is essential for the proper formation of the extracellular
matrix including the biogenesis and maintenance of elastic fibers. The extracellular
matrix is critical for both the structural integrity of connective tissue but also serves as a
reservoir for growth factors. Elastin fibers are found throughout the body but are
particularly abundant in the aorta, ligaments and the ciliary zonules of the eye;
consequently, these areas are among the worst affected.
A transgenic mouse has been created carrying a single copy of a mutant fibrillin
1, a mutation similar to that found in the human fibrillin 1 gene that is known to cause
Marfan syndrome. This mouse strain recapitulates many of the features of the human
disease and promises to provide insights into the pathogenesis of the disease. Reducing
the level of normal fibrillin-1 causes a Marfan-related disease in mice.[14]
Transforming growth factor beta (TGFβ) plays an important role in Marfan
syndrome. Fibrillin-1 indirectly binds a latent form of TGFβ keeping it sequestered and
unable to exert its biological activity. The simplest model of Marfan syndrome suggests
that reduced levels of fibrillin-1 allow TGFβ levels to rise due to inadequate
sequestration. Although it is not proven how elevated TGFβ levels are responsible for the
specific pathology seen with the disease, an inflammatory reaction releasing proteases
that slowly degrade the elastin fibers and other components of the extracellular matrix is
known to occur. The importance of the TGFβ pathway was confirmed with the discovery
of a similar syndromeLoeys-Dietz syndrome involving the TGFβR2 gene
on chromosome 3, a receptor protein of TGFβ. Marfan syndrome has often been confused
with Loeys-Dietz syndrome, because of the considerable clinical overlap between the two
syndromes.
Management:
There is no cure for Marfan syndrome, but life expectancy has increased
significantly over the last few decades, and clinical trials are underway for a promising
new treatment. The syndrome is treated by addressing each issue as it arises, and, in
particular, considering preventive medication, even for young children, to slow
progression of aortic dilation.
Regular checkups by a cardiologist are needed to monitor the health of the heart
valves and the aorta. The goal of treatment is to slow the progression of aortic dilation
and damage to heart valves by eliminating arrythmias, minimizing the heart rate, and
minimizing blood pressure. Beta blockers have been used to control arrythmias and slow
the heart rate. Other medications might be needed to further minimize blood pressure
without slowing the heart rate, such as ACE inhibitors and angiotensin II receptor
antagonists, also known as angiontensin receptor blockers (ARBs). If the dilation of the
aorta progresses to a significant diameter aneurysm, causes a dissection or a rupture, or
leads to failure of the aortic or other valve, then surgery (possibly a composite aortic
valve graft [CAVG] or valve-sparing procedure) becomes necessary. Although aortic
graft surgery (or any vascular surgery) is a serious undertaking it is generally successful
if undertaken on an elective basis. Surgery in the setting of acute aortic dissection or
rupture is considerably more problematic. Elective aortic valve/graft surgery is usually
considered when aortic root diameter reaches 50 millimeters (2.0 inches), but each case
needs to be specifically evaluated by a qualified cardiologist. New valve-sparing surgical
techniques are becoming more common. As Marfan patients live longer, other vascular
repairs are becoming more common, e.g., repairs of descending thoractic aortic
aneurysms and aneurysms of vessels other than the aorta.
Ehlers–Danlos syndrome (EDS) (also known as "Cutis hyperelastica") is a group
of inheritedconnective tissue disorders, caused by a defect in the synthesis of collagen (a
protein in connective tissue - usually Type I and III). The collagen in connective tissue
helps tissues to resist deformation (decreases its elasticity). In the skin, muscles,
ligaments, blood vessels and visceral organs, collagen plays a very significant role and
with increased elasticity, secondary to abnormal collagen, pathology results. Depending
on the individual mutation, the severity of the syndrome can vary from mild to lifethreatening. There is no cure, and treatment is supportive, including close monitoring of
the digestive, excretory and particularly the cardiovascular systems. Corrective surgery
may help with some of the problems that may develop in certain types of EDS, although
the condition means that extra caution is advised and special practices observed.
Signs vary widely based on which type of EDS the patient has. In each case,
however, the signs are ultimately due to faulty or reduced amounts of collagen. EDS most
typically affects the joints, skin, and blood vessels, the major signs and symptoms
include:
Highly flexible fingers and toes
Loose, unstable joints that are prone to: sprain, dislocation,subluxation (partial
dislocation) and hyperextension (double jointedness)
Flat feet
Joint pain without inflammation
Fatigue, which can be debilitating
High and narrow palate, resulting in dental crowding
Vulnerability to chest and sinus infections
Easy bruising
Fragile blood vessels resulting from cystic medial necrosis with tendency
towards aneurysm(even abdominal aortic aneurysm)
Velvety-smooth skin which may be stretchy and is often translucent, with blue
veins clearly visible on limbs and particularly in the hands
Abnormal wound healing and scar formation (scars may appear like cigarette
burns)[citation needed]
Low muscle tone and muscle weakness
Early onset of osteoarthritis
Cardiac effects: Dysautonomia typically accompanied by Valvular heart
disease (such as mitral valve prolapse, which creates an increased risk for
infective endocarditis during surgery, as well as possibly progressing to a life-threatening
degree of severity of the prognosis of mitral valve prolapse) [6]
Unexplained "pins and needles" or numbness in extremities
Difficulty regulating own body temperature, resulting in a vulnerability to the
cold and heat. Many patients suffer fatigue and dizziness when exposed to hot conditions,
eg. having to sit outside on a hot day
Severe mouth ulcers. Many patients complain of having several mouth ulcers at
any one time. This is believed to be due to tissue fragility and vulnerability to infection
Food allergies and intolerances are very common
Sensitivity to medications. One of the cruelest aspects of EDS is that many
patients experience bad reactions to medications, such as pain killers, making it very
difficult to find safe, effective pain management[citation needed]
Insensitivity to the dental anesthesia Lidocaine.
Migraines and headaches, including postural headaches from spontaneous
intracranial hypontension
Fibromyalgia symptoms: Myalgia and arthralgia[
The types of Ehlers-Danlos syndromes
Classical type
(formerly types I & II)
Marked joint hypermobility, skin hyperextensibility (laxity), and fragility are
characteristic of the classic type of Ehlers-Danlos syndrome. The smooth, velvety skin is
fragile and tears or bruises easily with minor trauma. Joint dislocations andscoliosis are
common. Joint instability can lead to sprains and strains. This classical type is inherited
as an autosomal dominant genetic trait (directly passed on from one parent to child).
Hypermobility type
(formerly type III)
Joint hypermobility is the major manifestation of this form of Ehlers-Danlos
syndrome. Any joint can be affected, and dislocations are frequent. This type is also
inherited as an autosomal dominant genetic trait.
Vascular type
(formerly type IV, the arterial form)
In this form of Ehlers-Danlos syndrome, spontaneous rupture of arteries and
bowel is a serious manifestation that can lead to death. Clubfoot can be present at birth.
Skin laxity is of varying degrees. Veins can be very visible through the skin. It is
primarily inherited as an autosomal dominant (directly passed on from one parent to
child) genetic trait, but recessive (not seen in family members or only in one generation
of members of the same family, meaning that an individual must inherit two copies of the
mutation, one from each parent) trait inheritance has been described.
Kyphoscoliosis type
(formerly type VI)
Fragile globe of the eyes, significant skin and joint laxity, and severe curvature of
the spine (scoliosis) are typical features. Its inheritance pattern is autosomal recessive.
Arthrochalsia type
(formerly type VIIB, arthrochalasis multiplex congenita)
Patients are short in height and severely affected by joint laxity and dislocations.
Skin involvement is variable. Both utosomal dominant and recessive inheritance is
possible. A skin biopsy can be used to diagnose this disorder.
Dermatosparaxis type
(formerly type VIIC)
Patients have severely fragile skin that is soft and doughy with sagging and
folding. This rare form of Ehlers-Danlos syndrome can be diagnosed with a skin biopsy.
Tenascin-X deficient type
Joint hypermobility, hyperelastic skin, and fragile tissue are seen. Patients with
this type lack the multiple shrinking (atrophied) scars in the skin that are often seen in
classic Ehlers-Danlos. It is inherited as an autosomal recessive genetic trait.
Genetics
Mutations in the following can cause Ehlers–Danlos syndrome:
Fibrous proteins: COL1A1, COL1A2, COL3A1, COL5A1, COL5A2, and TNXB
Enzymes: ADAMTS2, PLOD1
Mutations in these genes usually alter the structure, production, or processing
of collagen or proteins that interact with collagen. Collagen provides structure and
strength to connective tissue throughout the body. A defect in collagen can weaken
connective tissue in the skin, bones, blood vessels, and organs, resulting in the features of
the disorder.
Inheritance patterns depend on the type of Ehlers–Danlos syndrome. Most forms
of the condition are inherited in an autosomal dominantpattern, which means only one of
the two copies of the gene in question must be altered to cause the disorder. The minority
are inherited in an autosomal recessive pattern, which means both copies of the gene
must be altered for a person to be affected by the condition. It can also be an individual
(de novo or "sporadic") mutation. Please refer to the summary for each type of Ehlers–
Danlos syndrome for a discussion of its inheritance pattern.
Management:
There is no cure for Ehlers Danlos Syndrome. The treatment is supportive. Close
monitoring of the cardiovascular system, physical therapy, occupational therapy, and
orthopedic instruments (e.g., wheelchairs, bracing) may be helpful. One should avoid
activities that cause the joint to lock or overextend.
A physician may prescribe bracing to stabilize joints. Surgical repair of joints may
be necessary at some time. Physicians may also consult a physical and/or occupational
therapist to help strengthen muscles and to teach people how to properly use and preserve
their joints. To decrease bruising and improve wound healing, some patients have
responded to ascorbic acid (vitamin C) by taking 1 to 4 grams daily.[citation needed]
In general, medical intervention is limited to symptomatic therapy. Prior to
pregnancy, patients with EDS should have genetic counseling. Children with EDS should
be provided with information about the disorder, so they can understand why contact
sports and other physically stressful activities should be avoided. Children should be
taught early on that demonstrating the unusual positions they can maintain due to loose
joints should not be done as this may cause early degeneration of the joints. Family
members, teachers and friends should be provided with information about EDS so they
can accept and assist the child as necessary.
Prognosis:
The outlook for individuals with EDS depends on the type of EDS with which
they have been diagnosed. Symptoms vary in severity, even within one sub-type, and the
frequency of complications changes on an individual basis. Some individuals have
negligible symptoms while others are severely restricted in their daily life. Extreme joint
instability, pain, and spinal deformities may limit a person's mobility. Most individuals
will have a normal lifespan. However, those with blood vessel involvement have an
increased risk of fatal complications.
EDS is a lifelong condition. Affected individuals may face social obstacles related
to their disease on a daily basis. Some people with EDS have reported living with fears of
significant and painful ruptures, becoming pregnant,[16] their condition worsening,
becoming unemployed due to physical and emotional burdens, and social stigmatization
in general.
Patau syndrome
Patau syndrome, also known as trisomy 13 and trisomy D, is
a chromosomal abnormality, asyndrome in which a patient has an additional chromosome
13 due to a nondisjunction of chromosomes during meiosis. Some are caused
by Robertsonian translocations. The extra chromosome 13 disrupts the normal course of
development, causing heart and kidney defects amongst other features characteristic of
Patau syndrome.[vague] Like all nondisjunctionconditions (such as Down
syndrome and Edwards syndrome), the risk of this syndrome in the offspring increases
with maternal age at pregnancy, with about 31 years being the average. Patau syndrome
affects approximately one in 10,000 live births.
Causes:
Most cases of Patau's syndrome result from trisomy 13, which means each cell in
the body has three copies of chromosome 13 instead of the usual two copies. A small
percentage of cases occur when only some of the body's cells have an extra copy,
resulting in a mixed population of cells with a differing number of chromosomes; such
cases are called mosaic Patau.
Patau syndrome can also occur when part of chromosome 13 becomes attached to
another chromosome (translocated) before or at conception. Affected people have two
copies of chromosome 13, plus extra material from chromosome 13 attached to another
chromosome. With a translocation, the person has a partial trisomy for chromosome 13
and often the physical signs of the syndrome differ from the typical Patau syndrome.
Manifestations and physical findings
A 37 2/7 week gestational age male infant with Patau syndrome demonstrating
polydactyly
Of those fetuses that do survive to gestation and subsequent birth, common
abnormalites include:
Nervous system
Mental and motor challenged
Microcephaly
Holoprosencephaly (failure of the forebrain to divide properly).
Structural eye defects, including microphthalmia, Peters anomaly, cataract, iris
and/or fundus (coloboma), retinal dysplasia or retinal detachment,
sensory nystagmus, cortical visual loss, and optic nerve hypoplasia
Meningomyelocele (a spinal defect)
Musculoskeletal and cutaneous
Polydactyly (extra digits)
Low-set ears[3]
Prominent heel
Deformed feet known as rocker-bottom feet
Omphalocele (abdominal defect)
Abnormal palm pattern
Overlapping of fingers over thumb
Cutis aplasia (missing portion of the skin/hair)
Cleft palate
Urogenital
Abnormal genitalia
Kidney defects
Other
Heart defects (ventricular septal defect)
Single umbilical artery[4
Management:
Medical management of children with Trisomy 13 is planned on a case-by-case
basis and depends on the individual circumstances of the patient. Treatment of Patau
syndrome focuses on the particular physical problems with which each child is born.
Many infants have difficulty surviving the first few days or weeks due to severe
neurological problems or complex heart defects. Surgery may be necessary to repair heart
defects or cleft lip and cleft palate. Physical, occupational, and speech therapy will help
individuals with Patau syndrome reach their full developmental potential.
Prognosis:
More than 80% of children with Patau syndrome die within the first month of life
Trisomy 18 (T18) (also known as Trisomy E or Edwards syndrome) is a genetic
disordercaused by the presence of all or part of an extra 18th chromosome. It is named
after John H. Edwards, who first described the syndrome in 1960.[1] It is the second most
common autosomaltrisomy, after Down Syndrome, that carries to term.
Trisomy 18 is caused by the presence of three – as opposed to two – copies
of chromosome 18in a fetus or infant's cells. The incidence of the syndrome is estimated
as one in 3,000 live births.[2] The incidence increases as the mother's age increases. The
syndrome has a very low rate of survival, resulting from heart abnormalities, kidney
malformations, and other internal organ disorders.
It is impossible to predict the exact prognosis of a child with Edwards syndrome
during pregnancy or the neonatal period.[4]The median lifespan is 5–15 days.[5][6] One
percent of children born with this syndrome live to age 10, typically in less severe cases
of themosaic Edwards syndrome.[4] The small percentage of babies with the full
Edwards syndrome who survive birth and early infancy may live to adulthood, and
children with mosaic or partial forms of this trisomy may have a completely different and
much more hopeful prognosis
Edwards syndrome
Edwards syndrome is a chromosomal abnormality characterized by the presence
of an extra copy of genetic material on the 18th chromosome, either in whole
(trisomy 18) or in part (such as due to translocations). The additional chromosome
usually occurs before conception. The effects of the extra copy vary greatly, depending
on the extent of the extra copy, genetic history, and chance. Edwards syndrome occurs in
all human populations but is more prevalent in female offspring.
A healthy egg or sperm cell contains individual chromosomes, each of which
contributes to the 23 pairs of chromosomes needed to form a normal cell with a typical
human karyotype of 46 chromosomes. Numerical errors can arise at either of the
two meiotic divisions and cause the failure of a chromosome to segregate into the
daughter cells (nondisjunction). This results in an extra chromosome, making
the haploidnumber 24 rather than 23. Fertilization of eggs or insemination by sperm that
contain an extra chromosome results in trisomy, or three copies of a chromosome rather
than two.
Trisomy 18 (47,XX,+18) is caused by a meiotic nondisjunction event.
With nondisjunction, a gamete (i.e., a sperm or egg cell) is produced with an extra copy
of chromosome 18; the gamete thus has 24 chromosomes. When combined with a normal
gamete from the other parent, the embryo has 47 chromosomes, with three copies of
chromosome 18.
Features and characteristics:
Infants born with Edwards syndrome may have some or all of the following
characteristics: kidney malformations, structural heart defects at birth (i.e., ventricular
septal defect, atrial septal defect,patent ductus arteriosus), intestines protruding outside
the body (omphalocele), esophageal atresia,mental retardation, developmental delays,
growth deficiency, feeding difficulties, breathing difficulties, and arthrogryposis (a
muscle disorder that causes multiple joint contractures at birth).[10][11]
Some physical malformations associated with Edwards syndrome include small
head (microcephaly) accompanied by a prominent back portion of the head (occiput);
low-set, malformed ears; abnormally small jaw (micrognathia); cleft lip/cleft palate;
upturned nose; narrow eyelid folds (palpebral fissures); widely spaced eyes (ocular
hypertelorism); drooping of the upper eyelids (ptosis); a short breast bone; clenched
hands; choroid plexus cysts; underdeveloped thumbs and or nails absent
radius, webbing of the second and third toes; clubfoot or Rocker bottom feet; and
in males, undescended testicles.
In utero, the most common characteristic is cardiac anomalies, followed by
central nervous system anomalies such as head shape abnormalities. The most common
intracranial anomaly is the presence of choroid plexus cysts, which is a pocket of fluid on
the brain that is not problematic in itself but may be a marker for Trisomy 18. Sometimes
excess amniotic fluid or polyhydramnios is exhibited.
Management:
The Edward’s Syndrome is untreatable, though medical treatment can be provided
to abate the symptoms of the disease. The treatment should be focused on providing good
nutrition and tackling the frequent infections, while also working towards keeping the
heart healthy. Parents and other family members would need enormous emotional support
as the babies suffering from Edward’s Syndrome bare survive beyond their first year.
Prognosis:
The survival rate is very low in the Edward’s Syndrome as half of them die while
in the womb. Of those born, fifty percent die within two or three months of their birth,
while others die by the time they enter their first year. Usually the deaths are due to
malformations of heart.
Lutembacher's syndrome
Lutembacher's syndrome is a form of congenital heart disease. It is atrial septal
defect which involves mitral stenosis.
Lutembacher syndrome is defined as a combination of mitral stenosis and a leftto-right shunt at the atrial level. Typically, the left-to-right shunt is an atrial septal
defect (ASD) of the ostium secundum variety. Both these defects, ASD and mitral
stenosis, can be either congenital or acquired.
The definition of Lutembacher syndrome has undergone many changes. The
earliest description in medical literature is found in a letter written by anatomist Johann
Friedrich Meckel to Albrecht von Haller in 1750.1 In 1916, Lutembacher described his
first case of this syndrome, involving a 61-year-old woman, and he attributed the mitral
valvular lesion to congenital mitral stenosis. Because the mitral stenosis was, in fact,
rheumatic in etiology, the syndrome was defined eventually as a combination of
congenital ASD and acquired, almost always rheumatic, mitral stenosis.
In the current era of mitral valvuloplasty for acquired mitral stenosis, however,
residual iatrogenic ASD secondary to transseptal puncture is more common than
congenital ASD, as is the combination of ASD and mitral stenosis. Although this
syndrome is generally defined as mitral stenosis in combination with ASD, some have
argued to define the syndrome as a combination of ASD and any mitral valve lesion, ie,
mitral stenosis, mitral insufficiency, or mixed lesion. Currently, any combination of ASD,
congenital or iatrogenic, and mitral stenosis, congenital or acquired, is referred as
Lutembacher syndrome.
Pathophysiology:
Mitral stenosis can be either congenital, as initially described, or acquired in
origin, most commonly due to rheumatic mitral valve disease. Isolated mitral stenosis is
now known to be a rare congenital disorder, and most cases of mitral stenosis initially
thought to be congenital were, in fact, caused by rheumatic mitral valve disease.
Similarly, understanding of the etiology of ASD as associated with Lutembacher
syndrome has evolved over time. Initially, high left atrial pressure due to mitral stenosis
was thought to stretch open the patent foramen ovale (PFO), causing left-to-right shunt
and providing another outlet for the left atrium. Now ASD in this syndrome, like mitral
stenosis, is recognized as being either congenital or acquired, as already described.
Acquired ASD is almost always iatrogenic, either intentional or as a complication
of a percutaneous interventional procedure. The incidence of left-to-right atrial shunt
following mitral valvuloplasty is estimated at 11-12%. Although most of these ASDs are
small and hemodynamically insignificant, some can be large enough to have
hemodynamic consequences, especially in patients who develop restenosis of the mitral
valve.
The hemodynamic effects of this syndrome are a result of the interplay between
the relative effects of ASD and mitral stenosis. In its initial description, the ASD was
typically large in Lutembacher syndrome, thus providing another route for blood flow.
Iatrogenic ASDs tend to be smaller but still may be hemodynamically significant. The
direction of blood flow is determined largely by the compliance of left and right
ventricles. Normally, the right ventricle is more compliant than the left ventricle.
As a result, in the presence of mitral stenosis, blood flows to the right atrium
through the ASD instead of going backward into the pulmonary veins, thus avoiding
pulmonary congestion. This happens at the cost of progressive dilatation and, ultimately,
failure of the right ventricle and reduced blood flow to the left ventricle. Development of
Eisenmenger syndrome or irreversible pulmonary vascular disease is very uncommon in
the presence of large ASD and high left atrial pressure because of mitral stenosis.
The term reverse Lutembacher syndrome is sometimes used to describe those rare
cases in which a predominant right-to-left shunt develops owing to development of
severe tricuspid stenosis.
Causes:
Mitral stenosis is mostly rheumatic in origin.
Congenital mitral stenosis is very rare.
ASD is either congenital or iatrogenic.
Patients may remain asymptomatic for many years. Symptoms are mainly due to
the ASD, and signs and symptoms vary according to the size of the ASD. With a large
ASD, symptoms of pulmonary congestion, typical of isolated mitral stenosis, do not
appear until late in the course of the disease. Conversely, these symptoms may appear
early if the patient has an associated small ASD or develops pulmonary hypertension for
other reasons. Patients with large ASD and moderate-to-severe mitral stenosis have signs
and symptoms due mainly to right ventricular overload and right-sided heart failure,
while patients with a small ASD and moderate-to-severe mitral stenosis have signs and
symptoms of pulmonary congestion typical of mitral stenosis.
The patient may or may not have a history of rheumatic fever.
Fatigue and reduced exercise tolerance result from decreased systemic blood
flow. The presence of mitral stenosis and left-to-right blood flow in diastole through the
ASD reduces the forward flow of blood into the left ventricle, thereby reducing systemic
blood flow and leading to fatigue and poor exercise tolerance.
Palpitations are a common presenting symptom. Because of the augmented leftto-right shunt caused by higher left atrial pressure and mitral stenosis, both atria are
dilated. This predisposes patients to atrial arrhythmias; atrial fibrillation is very common.
Weight gain, ankle edema, right upper quadrant pain, and ascites are seen more
commonly in patients with large ASD. Such symptoms are manifestations of the
development of right-sided heart failure. A chronically increased left-to-right blood flow
at the atrial level can eventually lead to right-sided heart failure.
Paroxysmal nocturnal dyspnea, orthopnea, and hemoptysis are signs of pulmonary
venous congestion. Such symptoms are caused by mitral stenosis and are seen less
frequently in Lutembacher syndrome than in isolated mitral stenosis. They are more
common in patients with small ASD and are probably more common in patients who
develop reverse Lutembacher syndrome. In some patients with large pulmonary blood
flow due to a large left-to-right shunt, orthopnea can develop because of decreased
compliance of the lungs.
Physical
Physical examination reveals signs due to the ASD and mitral stenosis, which are
modified because of the presence of both lesions in the same patient.
Arterial pulse
Small volume
Rhythm regular or irregular -Atrial fibrillation most common arrhythmia
Jugular venous pulse
Distended jugular veins, even in the absence of right heart failure
Large a waves when sinus rhythm is present
Increased right ventricular pressure a more important determinant than
equalization of atrial pressures in increasing jugular venous pressure
Precordial examination
Left parasternal lift, caused by transmitted right ventricular and pulmonary artery
impulse, is common.
Left ventricular impulse is unimpressive, owing to reduced filling of the left
ventricle secondary to mitral stenosis.
A tapping apex impulse due to the palpable, loud first heart sound of mitral
stenosis may be present.
A diastolic thrill at the apex is unusual.
Heart sounds
Loud first heart sound, opening snap, and a mitral early-to-mid diastolic murmur
are the classic auscultatory findings of mitral stenosis and are variably present.
Reduced transmitral pressure gradient resulting from decompression of the left
atrium through the ASD and displacement of the left ventricular apex due to a large right
ventricle attenuate these classic findings of mitral stenosis.
Development of pulmonary hypertension and, consequently, an increase in right
atrial and left atrial pressures may increase transmitral pressure gradient and bring out
these auscultatory findings, but this phenomenon is canceled by further dilatation of the
right ventricle, thus obscuring the left ventricular apex.
The second heart sound (S2) may be widely split for 2 reasons. Increased right
heart flow of ASD can result in late closure of the pulmonary component of the S2, and
decreased left ventricular and aortic flow, secondary to mitral stenosis and ASD, can
cause early closure of the aortic component of S2.
Additional heart sounds and murmurs
Third and fourth heart sounds of right ventricular origin may be audible at the left
sternal border and are louder with inspiration.
Systolic murmurs are due to the following:
ASD along the upper left parasternal area - Typically a flow murmur due to
increased flow across the pulmonic valve
Tricuspid regurgitation along the lower left parasternal area - Due to the displaced
tricuspid valve secondary to right ventricular dilatation; common
Holosystolic murmur at the left parasternal area due to tricuspid regurgitation Usually increases with inspiration (Carvallo sign), which differentiates it from ASD and
mitral regurgitation
Mid diastolic murmurs are due to the following:
Increased flow across the tricuspid valve due to ASD or accompanying tricuspid
stenosis, best heard at left lower sternal border or at apex for reasons already mentioned
Mitral stenosis, best heard with stethoscope bell at apex after exercise and with
patient in left lateral position
Continuous murmur in the lower right sternal area is due to continuous shunting
of blood across a small ASD in the presence of severe mitral stenosis. This is an unusual
finding on physical examination.
Abdomen: Ascites and hepatomegaly may be noted in the presence of right heart
failure.
Extremities: Ankle edema may be present in the presence of right-sided heart
failure.
Management:
Medical Care
Symptomatic relief
Right-sided heart failure - Diuretics
Atrial arrhythmias - Digoxin, beta-blockers, and calcium channel blockers used
mainly for rate control, while amiodarone and sotalol used not only for rate control but
also for conversion into and maintenance of normal sinus rhythm
Subacute bacterial endocarditis (SBE) prophylaxis: Patients with Lutembacher
syndrome, unlike those with isolated ASD, are at high risk for SBE owing to associated
mitral stenosis; thus, SBE prophylaxis is warranted.
Surgical Care
Until recently, surgery was the only definite curative treatment available and
involved closure of the ASD and mitral commissurotomy or mitral valve replacement.5
Percutaneous closure of ASD and mitral balloon valvuloplasty6,7,8,9,10
Percutaneous closure of the ASD with a clamshell device and mitral valvuloplasty
provides a nonsurgical approach to correct these defects. Although mitral valvuloplasty
has been performed for several decades, percutaneous closure of an ASD with a device
represents a still-developing technology.
As already described, mitral valvuloplasty alone can be complicated by
development of ASD secondary to transseptal puncture performed as a part of the
procedure.
Indications for surgery or percutaneous intervention
ASD with a Qp/Qs ratio of more than 1.5
Moderate-to-severe mitral stenosis
Any degree of pulmonary hypertension, except individuals with irreversible
pulmonary hypertension (Eisenmenger syndrome, see below)
Surgery is now performed early rather than late because the rates of heart failure
and cardiac arrhythmia increase with age. Patients with pulmonary hypertension should
demonstrate reversibility of pulmonary vascular resistance prior to surgical (or
percutaneous) correction of ASD. Patients with pulmonary hypertension and irreversibly
increased pulmonary vascular resistance (ie, Eisenmenger physiology) invariably develop
progressive right-sided heart failure after ASD closure and die.
Cri du chat syndrome
Cri du chat syndrome, also known as chromosome 5p deletion syndrome, 5p
minus syndrome or Lejeune’s syndrome, is a rare genetic disorder due to a missing part
ofchromosome 5. Its name is a French term (cat-cry or call of the cat) referring to the
characteristic cat-like cry of affected children. It was first described by Jérôme Lejeune in
1963.[1] The condition affects an estimated 1 in 50,000 live births, strikes all ethnicities,
and is more common in females by a 4:3 ratio.
Signs and symptoms:
The syndrome gets its name from the characteristic cry of affected infants, which
is similar to that of a meowing kitten, due to problems with the larynx and nervous
system. About 1/3 of children lose the cry by age 2. Other symptoms of cri du chat
syndrome may include:
feeding problems because of difficulty swallowing and sucking.
low birth weight and poor growth.
severe cognitive, speech, and motor delays.
behavioral problems such as hyperactivity, aggression, tantrums, and repetitive
movements.
unusual facial features which may change over time.
excessive drooling.
constipation.
Other common findings include hypotonia, microcephaly, growth retardation, a
round face with full cheeks, hypertelorism, epicanthal folds, down-slanting palpebral
fissures, strabismus, flat nasal bridge, down-turned mouth, micrognathia, low-set ears,
short fingers, single palmar creases, and cardiac defects (e.g., ventricular septal
defect [VSD], atrial septal defect [ASD], patent ductus arteriosus [PDA], tetralogy of
Fallot). People with Cri du chat are fertile and can reproduce.
Less frequently encountered findings include cleft lip and palate, preauricular tags
and fistulas, thymic dysplasia, intestinal malrotation,megacolon, inguinal
hernia, dislocated hips, cryptorchidism, hypospadias, rare renal malformations
(e.g., horseshoe kidneys, renal ectopia or agenesis, hydronephrosis), clinodactyly of
the fifth fingers, talipes equinovarus, pes planus, syndactyly of the second and third
fingers and toes, oligosyndactyly, and hyperextensible joints. The syndrome may also
include various dermatoglyphics, including transverse flexion creases, distal axial
triradius, increased whorls and arches on digits, and a single palmar crease.
Late childhood and adolescence findings include significant intellectual
disability, microcephaly, coarsening of facial features, prominent supraorbital ridges,
deep-set eyes, hypoplastic nasal bridge, severe malocclusion, and scoliosis.
Affected females reach puberty, develop secondary sex characteristics, and
menstruate at the usual time. The genital tract is usually normal in females except for a
report of a bicornuate uterus. In males, testes are often small, but spermatogenesis is
thought to be normal.
Genetics:
Cri du chat syndrome is due to a partial deletion of the short arm
of chromosome number 5, also called "5p monosomy". Approximately 90% of cases
results from a sporadic, or randomly-occurring, de novo deletion. The remaining 10-15%
are due to unequal segregation of a parentalbalanced translocation where the 5p
monosomy is often accompanied by a trisomic portion of the genome. These individuals
may have more severe disease than those with isolated monosomy of 5p.
Most cases involve total loss of the most distant 20-10% of the material on the
short arm. Fewer than 10% of cases have other rare cytogenetic aberrations (e.g.,
interstitial deletions, mosaicisms, rings and de novo translocations). The deleted
chromosome 5 is paternal in origin in about 80% of de novo cases.
Loss of a small region in band 5p15.2 (cri du chat critical region) correlates with
all the clinical features of the syndrome with the exception of the catlike cry, which maps
to band 5p15.3 (catlike critical region). The results suggest that 2 noncontiguous critical
regions contain genes involved in this condition's etiology. Two genes in these
regions, Semaphorine F (SEMA5A) and delta catenin (CTNND2), are potentially
involved in cerebral development. The deletion of the telomerase reverse
transcriptase (hTERT) gene localized in 5p15.33 may contribute to the phenotypic
changes in cri du chat syndrome as well.
Diagnosis and Management:
Diagnosis is based on the distinctive cry and accompanying physical
problems. Genetic counseling and genetic testing may be offered to families with
individuals who have cri du chat syndrome. Children may be treated by speech, sound,
and occupational therapists. Cardiac abnormalities often require surgical correction.
Cornelia De Lange Syndrome
Cornelia de Lange syndrome (CdLS) is a syndrome of multiple congenital
anomalies characterized by a distinctive facial appearance, prenatal and postnatal growth
deficiency, feeding difficulties, psychomotor delay, behavioral problems, and associated
malformations that mainly involve the upper extremities. Cornelia de Lange first
described it as a distinct syndrome in 1933,1 although Brachmann had described a child
with similar features in 1916.2Diagnosing classic cases of Cornelia de Lange syndrome is
usually straightforward; however, diagnosing mild cases may be challenging, even for an
experienced clinician.
Facial appearance of a patient with Cornelia de Lange syndrome. Courtesy of Ian
Krantz, MD, Children's Hospital of Philadelphia.
Facial profile of a patient with Cornelia de Lange syndrome. Courtesy of Ian
Krantz, MD, Children's Hospital of Philadelphia.
Severe upper-extremity malformations in a patient with Cornelia de Lange
syndrome. Courtesy of Ian Krantz, MD, Children's Hospital of Philadelphia.
Pathophysiology:
More than 99% of cases are sporadic. Cornelia de Lange syndrome is
occasionally transmitted in an autosomal dominant pattern, according to several instances
in which a usually mildly affected parent had one or more affected offspring. Twins with
concordance and discordance have been reported. Although possible autosomal recessive
inheritance has been reported in some families, these instances were likely to be due to
germline mosaicism. The recurrence risk is 0.5-1.5% if parents are unaffected and 50% if
a parent is affected.
Heterozygous mutations in a gene named NIPBL, the human homolog of the Drosophila
melanogaster Nipped-B gene,3 have been identified in approximately 50% of individuals
with Cornelia de Lange syndrome.4 Although the exact function of the protein product
of NIPBL in humans (delangin) remains unknown, its homologs in other species are
known to play roles in developmental regulation and in cohesion of sister chromatids.
Mutations in genes, coding for two other proteins involved in cohesion of sister
chromatids, SMC1A and SMC3, have been reported in 5% and 1% of patients with
Cornelia de Lange syndrome, respectively.5 Thus, Cornelia de Lange syndrome is
considered to be a cohesinopathy, along with Roberts syndrome/SC phocomelia.
Inheritance is autosomal dominant in families with NIPBL and SMC3 mutations
and is X-linked dominant in families with SMC1A mutations.
All types of NIPBL mutations, including missense, splice-site, nonsense, and frameshift
mutations, have been reported to result in the Cornelia de Lange syndrome phenotype.
The most likely effect of these mutations is haploinsufficiency. The mutation-detection
rate is approximately 50%. Genomic deletions and duplications of theNIPBL locus are
rare.6 Reported mutations of SMC1A include missense mutations and in-frame
deletions. One reported SMC3 mutation is an in-frame deletion.
The correlation between genotype and phenotype suggested that individuals with an
identifiable mutation in NIPBLhave a phenotype more severe than the phenotype of those
without mutations. Moreover, missense mutations inNIPBL are associated with mild
phenotypic features. Patients with mutations in SMC1A and SMC3consistently have a
milder phenotype, with absence of severe limb defects and other structural anomalies.
The phenotype in some patients is close to those with nonsyndromic mental retardation.
A phenotype similar to that of Cornelia de Lange syndrome may be observed in
patients with a duplication of band q26-27 on chromosome 3.7 Molecular studies of
genes mapped to this region of chromosome arm 3q have failed to reveal mutations in
patients with Cornelia de Lange syndrome.
Some autopsy data have indicated cerebral dysgenesis, with a decreased number
of neurons, neuronal heterotopias, and focal gyral folding abnormalities as causes of
psychomotor delay.
hysical findings in patients with Cornelia de Lange syndrome may include the
following:
Short stature: In some patients, extreme short stature may be caused by growth
hormone deficiency. Specific growth curves in Cornelia de Lange syndrome are
available. Average adult weight is 30.5 kg in females and 47.6 kg in males; average
height is 131 cm in females and 156 cm in males.
Microcephaly (98%): Average adult head circumference is 49 cm in both sexes.
Facial features
These are perhaps the most diagnostic of all the physical signs and combine to
create a unique gestalt for the clinician. This combination of findings may be absent in
postpubertal male patients.
The following are classic features:
Confluent eyebrows (synophrys) (99%)
Long curly eyelashes (99%)
Low anterior and posterior hairline (92%)
Underdeveloped orbital arches (100%)
Neat, well-defined, and arched eyebrows (as though they had been penciled)
Long philtrum
Anteverted nares (88%)
Down-turned angles of the mouth (94%)
Thin lip (especially upper vermillion border)
Low-set and posteriorly rotated ears
Depressed nasal bridge (83%)
High arched palate (86%) and overt or submucous cleft palate (20%)
Late eruption of widely spaced teeth (86%)
Micrognathia (84%)
Short neck (66%)
Hirsutism (78%)
Generalized hirsutism is observed most easily in dark-haired individuals.
Many infants lose their obvious excessive body hair later in life.
Cutis marmorata and perioral cyanosis (56%)
Hypoplastic nipples and umbilicus (50%)
Micromelia (93%)
Severe abnormalities, such as oligodactyly (missing digits) or other deficiencies
of the arms, may be present (27%). They usually occur in severely affected patients.
Less-striking limb findings include single palmar flexion crease, clinodactyly of
the fifth fingers, proximally placed thumbs, partial syndactyly of the second and third
toes, and limitation of elbow extension.
Relative smallness of the hands or feet is almost universal.
Congenital heart disease (25%), typically ventricular septal defect or atrial septal
defect: Any lesion may be seen.
Hip abnormalities, including dislocation or dysplasia (10%), scoliosis, tight
Achilles tendons and the development of bunions
Hypoplastic external male genitalia (57%), small labia majora
Undescended testes (73%)
Hypospadias (33%)
Ophthalmologic manifestations (50%)
Myopia (58%), ptosis (44%), blepharitis (25%), epiphora (22%), microcornea
(21%), strabismus (16%), nystagmus (14%) occur. Peripapillary pigment ring was noted
in most patients.
Glasses are often poorly tolerated.
Astigmatism, optic atrophy, coloboma of the optic nerve, aniridia, and congenital
glaucoma have been described.
Causes:
Heterozygous mutations in the NIPBL and SMC3 and heterozygous (in females)
or hemizygous (in males) mutations in SMC1A result in Cornelia de Lange syndrome.
Most cases are sporadic due to de novo mutations
Management:
Medical Care
Early intervention in patients with Cornelia de Lange syndrome (CdLS) is
necessary for feeding problems, hearing and visual impairment, congenital heart disease,
and urinary system abnormalities.
Early intervention for psychomotor delay is also indicated.
Computer programs that emphasize visual memory are more beneficial than
standard methods of verbal instruction.
Perceptual organizational tasks should be emphasized.
Tactile stimulation during indirection helps the children remember and perform
maximally.
Fine motor activities, when physical impairments do not limit them, should be
stressed in education, especially activities related to activities of daily living.
Surgical Care
Surgery may be necessary for the following conditions:
Cleft palate
Nasal polyps
Gastroesophageal reflux disease
Pyloric stenosis
Intestinal malrotation/volvulus
Undescended testis
Lacrimal duct stenosis
Hip dislocations
Klippel-Feil Syndrome
Maurice Klippel and Andre Feil independently provided the first descriptions of
Klippel-Feil syndrome. They described patients who had a short, webbed neck; decreased
range of motion (ROM) in the cervical spine; and a low hairline. Feil subsequently
classified the syndrome into 3 categories:
Type I - a massive fusion of the cervical spine
Type II - the fusion of 1 or 2 vertebrae
Type III - the presence of thoracic and lumbar spine anomalies in association with
type I or type II Klippel-Feil syndrome
In a series of articles, Samartzis and colleagues suggested a new classification
system.1,2 In this classification system, type I patients have a single-level fusion; type II
patients have multiple, noncontiguous fused segments; and type III patients have
multiple, contiguous fused segments. Using their system, the investigators reviewed a
series of patients to clarify prognosis (see Clinical). See images below.
Posterior photo of a patient with Klippel-Feil syndrome and an anomaly of the
occipitocervical junction. The image shows an elevated left shoulder due to a Sprengel
anomaly; a short, webbed neck; and a low hairline.
This patient has Klippel-Feil syndrome and an anomaly of the occipitocervical
junction. The patient's flexion and extension after the occipitocervical fusion is
demonstrated. His rotation was very limited.
Flexion of the cervical spine in a patient who had an occipitocervical fusion.
This photo demonstrates synkinesia. As the patient attempts to oppose the thumb
and finger of the right hand, the same movement occurs involuntarily in the left.
Patients with Klippel-Feil syndrome usually present with the disease during
childhood, but may present later in life. The challenge to the clinician is to recognize the
associated anomalies that can occur with Klippel-Feil syndrome and to perform the
appropriate workup for diagnosis.
Etiology:
The etiology of Klippel-Feil syndrome and its associated conditions is unknown.
The syndrome can present with a variety of other clinical syndromes, including fetal
alcohol syndrome, Goldenhar syndrome, and anomalies of the
extremities.5,6,7 Gunderson suggested that it is a genetic condition, while Gray found a
low incidence of inheritance.8,9 Others have considered Klippel-Feil syndrome to be
some type of global fetal insult, which could explain the other associated conditions.
Some have considered it to be caused by vascular disruption
Clinical presentation:
Clinical presentation is varied because of the different associated syndromes and
anomalies that can occur in patients with Klippel-Feil syndrome. A complete history and
careful physical examination may reveal some associated anomalies. From an orthopedic
standpoint, most of the workup involves imaging (see Workup, Imaging Studies).
Klippel-Feil syndrome is detected throughout life, often as an incidental finding.
Patients with upper cervical spine involvement tend to present at an earlier age than those
whose involvement is lower in the cervical spine. Most patients present with a short neck
and a decreased cervical ROM, with a low hairline occurring in 40-50% of patients.
Decreased ROM is the most frequent clinical finding. Rotational loss usually is more
pronounced than is the loss of flexion and extension.
Other patients present with torticollis or facial asymmetry. Neurologic problems
may develop in 20% of patients.
Patients with Klippel-Feil syndrome present at different ages with varying clinical
manifestations. Indications for workup vary individually. For the orthopedic surgeon, the
most frequent indications for surgery depend on the amount of deformity, its location,
and its progression with time. Other indications include instability of the cervical spine
and/or neurologic problems. These indications can occur with craniocervical junction
anomalies and when 2 fused segments are separated by a normal segment.
Some patients present early in life with complex cervical and cervicothoracic
deformity that is progressive and disfiguring. Some of these patients require cervical
spine fusions to prevent progression.
Other patients may develop compensatory or associated congenital scoliosis,
which also can be progressive over time and requires fusion to prevent progressive
deformity. Over 50% of the patients in Hensinger's study had scoliosis.14 Treatment of
the scoliosis with bracing or surgery was required in 18 of the 50 patients.
Outcome and Prognosis:
The prognosis for Klippel-Feil syndrome depends on the specific anomalies.
Careful evaluation, consistent follow-up, and coordination with other providers are
required to avoid pitfalls and to avoid missing any diagnoses. The classification system
created by Samartzis and colleagues is useful in predicting which patients may develop
symptoms.
Velocardiofacial Syndrome
Velocardiofacial syndrome (VCFS) is a genetic condition characterized by
abnormal pharyngeal arch development that results in defective development of the
parathyroid glands, thymus, and conotruncal region of the heart. Shprintzen and
colleagues first described the syndrome in 1978.1 More than 180 different clinical
features are associated with velocardiofacial syndrome, with no single anomaly present in
every patient. Some abnormalities are more common than others. Affected
individuals may present with structural or functional palatal abnormalities, cardiac
defects, unique facial characteristics, hypernasal speech, hypotonia, and defective thymic
development.
Clinical Features:
Cyanosis may be present in individuals with velocardiofacial syndrome (VCFS) if
cardiac disease is also present (eg, truncus arteriosus, tetralogy of Fallot).
Feeding difficulty and slow growth may occur due to congestive heart failure,
palatal abnormality, or hypotonia.
Nasal regurgitation of formula in infancy is common in patients later diagnosed
with submucous cleft palate.
Delayed speech development associated with poor articulation and hypernasality
can be caused by velopharyngeal incompetence (VPI). Patients may be unresponsive to
speech therapy.
Recurrent otitis media associated with palatal abnormality can contribute to
speech delay and hearing loss, which often require the placement of ventilating tubes.
Developmental delay in infants with a learning disorder becomes apparent in
childhood. Attention deficit hyperactivity disorder (ADHD) occurs in 35-55% of persons
with velocardiofacial syndrome.
Poor social interaction or behavioral difficulties are common. Psychiatric
disorders (including obsessive-compulsive disorder and schizophrenia) are reported in at
least 10% of patients.
Seizures related to hypocalcemia generally occur in the first year of life. The
hypocalcemia generally resolves spontaneously over time, although a small number of
patients present with hypocalcemia in the teen years. Frequent upper respiratory
infections are commonly reported.
Short stature has been reported in approximately 30% of patients with
velocardiofacial syndrome.
Physical
Cyanosis may be present if an obligate systemic-to-pulmonic (right-to-left) shunt
is present.
A heart murmur is present in most patients with a cardiac defect.
Craniofacial dysmorphism is often observed as a round face in infancy with
prominent parietal bones and a bulbous nasal tip. The face appears long and hypotonic
with narrow palpebral fissures, puffy upper eyelids, a squared nasal root, and a narrow
alar base with thin alae nasi. Facial asymmetry, microcephaly, and small, often unusually
shaped, ears may be noted at any age.
A palatal abnormality can manifest as an overt cleft palate affecting the hard or
soft palate or as a submucous cleft palate that can be detected upon palpation of the hard
palate. Even a normal-appearing palate can be associated with velopharyngeal
incompetence.
Hypernasal speech and poor articulation often are observed.
Hypospadias or cryptorchidism may be present in males.
Varying degrees of hypotonia are observed in patients and may be associated with
delay of motor, speech, and feeding skills. The presence of developmental delays is
independent from the presence of a hearing defect.
Long and tapering fingers are a common sign of velocardiofacial syndrome.
Causes:
Most patients with velocardiofacial syndrome have a microdeletion at the q11.2
locus of the long arm of chromosome 22. About 10% of patients inherit this deletion from
a parent, and the rest have it as the result of a new mutation.
Abnormal exchange between chromosome 22s during meiosis is the predominant
mechanism for this deletion.
Management:
Medical Care
Evaluation of patients with velocardiofacial syndrome (VCFS) usually occurs in
an outpatient setting. In newborns, diagnosis may be made in the hospital.
If needed, use medical therapy to treat heart failure, hypocalcemia, immune
deficiency, feeding problems, and inadequate growth.
In terms of neurocognitive issues associated with velocardiofacial syndrome,
during infancy and preschool years, feeding problems, cleft palate, and developmental
disorders occupy most of the clinical management in these patients. During school years,
management shifts to cognitive, behavioral, and learning disorders. The most common
cognitive finding in these patients is functioning within the low-borderline range. Related
features include significant visuospatial dysfunction, diminished math attainment, and
executive dysfunction. In late adolescence and adult years, psychiatric illness such as
schizophrenia or bipolar disorder become more of a concern because these may develop
in 10% of adults with this condition.
Surgical Care
At the time of surgery, the complex cardiovascular anatomy in association with
depressed immunological status, pulmonary vascular reactivity, neonatal hypocalcemia,
bronchomalacia and bronchospasm, laryngeal web, and tendency for airway bleeding
must be considered.
Irradiated cell blood products should be used in patients susceptible to
developing graft versus host disease; if the immune status of the patient is not known,
irradiated cell blood products must be used.
A cleft palate should be repaired.
Pharyngeal flap surgery may be required to treat velopharyngeal incompetence
(VPI) and improvement in hypernasality; in planning the surgery, consider that the
internal carotid is commonly medially displaced and tortuous.
Ventilation of ear tubes may be indicated.
Fetal alcohol syndrome
Fetal alcohol syndrome (FAS) is a pattern of mental and physical defects that can
develop in a fetus when a woman drinks alcohol during pregnancy. The timing and
frequency of alcohol consumption during pregnancy are major factors in the risk of a
child developing fetal alcohol syndrome. While the ingestion of alcohol does not always
result in FAS, there are no medically established guidelines for safe levels of alcohol
consumption during pregnancy. The current recommendation of both the Surgeon
General of the United States and the British Department of Health is to drink no alcohol
at all during pregnancy.
Alcohol crosses the placental barrier and can stunt fetal growth or weight, create
distinctive facial stigmata, damage neurons and brain structures, which can result in
psychological or behavioral problems, and cause other physical damage. Surveys found
that in the United States, 10–15% of pregnant women report having recently used
alcohol, and up to 30% use alcohol at some point during pregnancy.
The main effect of FAS is permanent central nervous system damage, especially
to the brain. Developing brain cells and structures can be malformed or have
development interrupted by prenatal alcohol exposure; this can create an array of
primary cognitive and functional disabilities (including poor memory, attention deficits,
impulsive behavior, and poor cause-effect reasoning) as well as secondary disabilities
(for example, predispositions to mental health problems and drug addiction). Alcohol
exposure presents a risk of fetal brain damage at any point during a pregnancy, since
brain development is ongoing throughout pregnancy.
Fetal alcohol exposure is the leading known cause of intellectual disability in the
Western world. In the United States and Europe, the FAS prevalence rate is estimated to
be between 0.2-1.5 in every 1000 live births. The lifetime medical and social costs of
FAS are estimated to be as high as US$800,000 per child born with the disorder.
Signs and symptoms:
Growth deficiency:
Growth deficiency is defined as below average height, weight or both due to
prenatal alcohol exposure, and can be assessed at any point in the lifespan. Growth
measurements must be adjusted for parental height, gestational age (for a premature
infant), and other postnatal insults (e.g., poor nutrition), although birth height and weight
are the preferred measurements. Deficiencies are documented H191 when height or
weight falls at or below the 10th percentile of standardized growth charts appropriate to
the patient's population.
The CDC and Canadian guidelines use the 10th percentile as a cut-off to
determine growth deficiency. The "4-Digit Diagnostic Code" allows for mid-range
gradations in growth deficiency (between the 3rd and 10th percentiles) and severe growth
deficiency at or below the 3rd percentile. Growth deficiency (at severe, moderate, or mild
levels) contributes to diagnoses of FAS and PFAS (Partial Fetal Alcohol Syndrome), but
not ARND (Alcohol-Related Neurodevelopmental Disorder) or static encephalopathy.
Growth deficiency is ranked as follows by the "4-Digit Diagnostic Code:"
Severe — Height and weight at or below the 3rd percentile.
Moderate — Either height or weight at or below the 3rd percentile, but not both.
Mild — Both height and weight between the 3rd and 10th percentiles.
None — Height and weight both above the 10th percentile.
Facial features:
Baby with Fetal alcohol syndrome.
Several characteristic craniofacial abnormalities are often visible in individuals
with FAS. The presence of FAS facial features indicates brain damage, though brain
damage may also exist in their absence. FAS facial features (and most other visible, but
non-diagnostic, deformities) are believed to be caused mainly during the 10th and 20th
week of gestation.
Refinements in diagnostic criteria since 1975 have yielded three distinctive and
diagnostically significant facial features known to result from prenatal alcohol exposure
and distinguishes FAS from other disorders with partially overlapping
characteristics. The three FAS facial features are:
A smooth philtrum — The divot or groove between the nose and upper lip flattens
with increased prenatal alcohol exposure.
Thin vermilion — The upper lip thins with increased prenatal alcohol exposure.
Small palpebral fissures — Eye width decreases with increased prenatal alcohol
exposure.
Measurement of FAS facial features uses criteria developed by the University of
Washington. The lip and philtrum are measured by a trained physician with the LipPhiltrum Guide, a 5-point Likert Scale with representative photographs of lip and
philtrum combinations ranging from normal (ranked 1) to severe (ranked 5). Palpebral
fissure length (PFL) is measured in millimeters with either calipers or a clear ruler and
then compared to a PFL growth chart, also developed by the University of Washington.
Ranking FAS facial features is complicated because the three separate facial
features can be affected independently by prenatal alcohol. A summary of the criteria
follows:[16][26]
Severe — All three facial features ranked independently as severe (lip ranked at 4
or 5, philtrum ranked at 4 or 5, and PFL two or more standard deviations below average).
Moderate — Two facial features ranked as severe and one feature ranked as
moderate (lip or philtrum ranked at 3, or PFL between one and two standard deviations
below average).
Mild — A mild ranking of FAS facial features covers a broad range of facial
feature combinations:
Two facial features ranked severe and one ranked within normal limits,
One facial feature ranked severe and two ranked moderate, or
One facial feature ranked severe, one ranked moderate and one ranked within
normal limits.
None — All three facial features ranked within normal limits.
These distinctive facial features in a patient do strongly correlate to brain
damage. Sterling Clarren of the University of Washington's Fetal Alcohol and Drug Unit
told a conference in 2002:
“I have never seen anybody with this whole face who doesn't have some brain
damage. In fact in studies, as the face is more FAS-like, the brain is more likely to be
abnormal. The only face that you would want to counsel people or predict the future
about is the full FAS face. But the risk of brain damage increases as the eyes get smaller,
as the philtrum gets flatter, and the lip gets thinner. The risk goes up but not the
diagnosis.“
“At one-month gestation, the top end of your body is a brain, and at the very front
end of that early brain, there is tissue that has been brain tissue. It stops being brain and
gets ready to be your face ... Your eyeball is also brain tissue. It's an extension of the
second part of the brain. It started as brain and "popped out." So if you are going to look
at parts of the brain from alcohol damage, or any kind of damage during pregnancy, eye
malformations and midline facial malformations are going to be very actively related to
the brain across syndromes ... and they certainly are with FAS.”
Central nervous system:
Central nervous system (CNS) damage is the primary feature of any Fetal Alcohol
Spectrum Disorder (FASD) diagnosis. Prenatal exposure to alcohol — which is classified
as a teratogen — can damage the brain across a continuum of gross to subtle
impairments, depending on the amount, timing, and frequency of the exposure as well as
genetic predispositions of the fetus and mother.[3][28] While functional abnormalities are
the behavioral and cognitive expressions of the FAS disability, CNS damage can be
assessed in three areas: structural, neurological, and functional impairments.
All four diagnostic systems allow for assessment of CNS damage in these areas,
but criteria vary. The IOM system requires structural or neurological impairment for a
diagnosis of FAS. The "4-Digit Diagnostic Code" and CDC guidelines state that
functional anomalies must measure at two standard deviations or worse in three or more
functional domains for a diagnosis of FAS. The "4-Digit Diagnostic Code" further
elaborates the degree of CNS damage according to four ranks:
Definite — Structural impairments or neurological impairments for FAS or static
encephalopathy.
Probable — Significant dysfunction of two standard deviations or worse in three
or more functional domains.
Possible — Mild to moderate dysfunction of two standard deviations or worse in
one or two functional domains or by judgment of the clinical evaluation team that CNS
damage cannot be dismissed.
Unlikely — No evidence of CNS damage.
Prevention:
The only certain way to prevent FAS is to simply avoid drinking alcohol during
pregnancy.
Prognosis:
Primary disabilities:
The primary disabilities of FAS are the functional difficulties with which the child
is born as a result of CNS damage due to prenatal alcohol exposure. Often, primary
disabilities are mistaken as behavior problems, but the underlying CNS damage is the
originating source of a functional difficulty (rather than a mental health condition, which
is considered a secondary disability).
The exact mechanisms for functional problems of primary disabilities are not
always fully understood, but animal studies have begun to shed light on some correlates
between functional problems and brain structures damaged by prenatal alcohol
exposure. Representative examples include:
Learning impairments are associated with impaired dendrites of the hippocampus
Impaired motor development and functioning are associated with reduced size of
the cerebellum
Hyperactivity is associated with decreased size of the corpus callosum
Functional difficulties may result from CNS damage in more than one domain,
but common functional difficulties by domain include: (This is not an exhaustive list of
difficulties.)
Achievement — Learning disabilities
Adaptive behavior — Poor impulse control, poor personal boundaries, poor anger
management, stubbornness, intrusive behavior, too friendly with strangers, poor daily
living skills, developmental delays
Attention — Attention-Deficit/Hyperactivity Disorder (ADHD), poor attention or
concentration, distractible
Cognition — Mental retardation, confusion under pressure, poor abstract skills,
difficulty distinguishing between fantasy and reality, slowercognitive processing
Executive functioning — Poor judgment, Information-processing disorder, poor at
perceiving patterns, poor cause and effect reasoning, inconsistent at linking words to
actions, poor generalization ability
Language — Expressive or receptive language disorders, grasp parts but not
whole concepts, lack understanding of metaphor, idioms, or sarcasm
Memory — Poor short-term memory, inconsistent memory and knowledge base
Motor skills — Poor handwriting, poor fine motor skills, poor gross motor skills,
delayed motor skill development (e.g., riding a bicycle at appropriate age)
Sensory integration and soft neurological problems — sensory integration
dysfunction, sensory defensiveness, undersensitivity to stimulation
Social communication — Intrude into conversations, inability to
read nonverbal or social cues, "chatty" but without substance
Secondary disabilities:
The secondary disabilities of FAS are those that arise later in life secondary to
CNS damage. These disabilities often emerge over time due to a mismatch between the
primary disabilities and environmental expectations; secondary disabilities can be
ameliorated with early interventions and appropriate supportive services.[10]
Six main secondary disabilities were identified in a University of Washington
research study of 473 subjects diagnosed with FAS, PFAS (partial fetal alcohol
syndrome), and ARND (alcohol-related neurodevelopmental disorder):[6][10]
Mental health problems — Diagnosed with ADHD, Clinical Depression, or
other mental illness, experienced by over 90% of the subjects
Disrupted school experience — Suspended or expelled from school or dropped
out of school, experienced by 60% of the subjects (age 12 and older)
Trouble with the law — Charged or convicted with a crime, experienced by 60%
of the subjects (age 12 and older)
Confinement — For inpatient psychiatric care, inpatient chemical dependency
care, or incarcerated for a crime, experienced by about 50% of the subjects (age 12 and
older)
Inappropriate sexual behavior — Sexual advances, sexual touching, or
promiscuity, experienced by about 50% of the subjects (age 12 and older)
Alcohol and drug problems — Abuse or dependency, experienced by 35% of the
subjects (age 12 and older)
Two additional secondary disabilities exist for adult patients:[6][10]
Dependent living — Group home, living with family or friends, or some sort of
assisted living, experienced by 80% of the subjects (age 21 and older)
Problems with employment — Required ongoing job training or coaching, could
not keep a job, unemployed, experienced by 80% of the subjects (age 21 and older)
Apert syndrome
Apert syndrome is a form of acrocephalosyndactyly, a congenital
disorder characterized by malformations of the skull, face, hands and feet. It is classified
as a branchial arch syndrome, affecting the first branchial (or pharyngeal) arch, the
precursor of the maxilla and mandible. Disturbances in the development of the branchial
arches in fetal development create lasting and widespread effects.
Apert syndrome is a genetic disease in which the seams between the skull bones
close earlier than normal. This affects the shape of the head and face.
Causes, incidence, and risk factors:
Apert syndrome can be passed down through families (inherited). The syndrome
is inherited as an autosomal dominant trait, which means that only one parent needs to
pass on the faulty gene for a child to have the condition.
Some cases may occur without a known family history.
Apert syndrome is caused by mutations in a gene called fibroblast growth factor
receptor 2. This gene defect causes some of the bony sutures of the skull to close too
early, a condition called craniosynostosis.
People with Apert syndrome have a distinctive looking face, and there may be
full-length webbing or fusion between the 2nd, 3rd, and 4th fingers, as well as the toes.
As the child grows, the bones in the hands and feet become progressively fused, which
reduces flexibility and function.
Several other syndromes that include craniosynostosis can lead to a similar
appearance of the face and head, but do not include the severe hand and foot problems of
Apert syndrome. These similar syndromes include:
Carpenter syndrome (kleeblattschadel, cloverleaf skull deformity)
Crouzon disease (craniofacial dysostosis)
Pfeiffer syndrome
Saethre-Chotzen syndrome
Symptoms
Early closure of sutures between bones of the skull, noted by ridging along
sutures
Frequent ear infections
Fusion or severe webbing of the 2nd, 3rd, and 4th fingers, often called "mitten
hands"
Hearing loss
Large or late-closing soft spot on a baby's skull
Possible, slow intellectual development (varies from person to person)
Prominent or bulging eyes
Severe under-development of the mid-face
Skeletal (limb) abnormalities
Short height
Webbing or fusion of the toes
Signs and tests
A skull x-ray and physical exam can confirm the diagnosis of craniosynostosis.
Hand or foot x-rays are also very important to determine the extent of bone
problems.
A genetic test for mutations in the fibroblast growth factor receptor 2 gene can
confirm the diagnosis of Apert syndrome. Hearing tests should also always be performed.
Management:
The patient should be evaluated by a multispecialty cranio-facial surgery team at a
children's medical center. Treatment consists of surgery to correct abnormal bone growth
of the skull, mid-face, and jaw area.
Plastic Surgery is needed to prevent the closing of the coronal sutures from
damaging brain development. In particular, the LeFort III, a plastic surgical procedure,
detaches the midface from the rest of the skull in order to reposition it in the correct
plane. Aggressive surgery is needed to separate as many fingers and toes as possible.
Maladie de Roger syndrome
Also known as Roger's disease, Maladie de Roger (French), Roger’s syndrome
Interventricular septal defect, ventricular septal defect, VSD.
Description
A congenital, small, asymptomatic defect of the septum between the ventricles of
the heart. Occurs in two types, with mild pulmonic stenosis and with severe pulmonic
stenosis.
A ventricular septal defect (VSD) is a hole or a defect in the septum that divides
the 2 lower chambers of the heart and that results in a communication between the
ventricular cavities. The defect may occur as a primary anomaly with or without
additional major associated cardiac defects. A ventricular septal defect may occur as a
single component of a wide variety of intracardiac anomalies, including tetralogy of
Fallot (TOF), complete atrioventricular (AV) canal defects, transposition of great arteries,
and corrected transpositions.
The following image represents the various types of ventricular septal defects.
Schematic representation of the location of various types of ventricular septal
defects (VSDs) from the right ventricular aspect. A = Doubly committed subarterial
ventricular septal defect; B = Perimembranous ventricular septal defect; C = Inlet or
atrioventricular canal–type ventricular septal defect; D = Muscular ventricular
septal defect.
In this the term ventricular septal defect refers to an isolated ventricular septal
defect, or a defect in a heart with AV concordance. That is, the atria are attached to the
correct ventricle and the normally related arteries (great arteries arising from the
appropriate ventricle [ie, an otherwise normal heart]) with no other major lesions.
Isolated ventricular septal defect occurs in approximately 2-6 of every 1000 live births
and accounts for more than 20% of all congenital heart diseases. Ventricular septal
defects are the most common congenital heart defects encountered after bicuspid aortic
valves.
Credit for the first clinical description is generally given to Roger's article
published in 1879.1 The phrase maladie de Roger is still used to refer to a small
asymptomatic ventricular septal defect. In 1898, Eisenmenger described a patient with
ventricular septal defect, cyanosis, and pulmonary hypertension. This combination of a
ventricular septal defect, pulmonary vascular disease, and cyanosis has been termed the
Eisenmenger complex. Pulmonary vascular disease and cyanosis in combination with any
other systemic-to-pulmonary connection has been called the Eisenmenger
syndrome.2 Heath and Edwards described the morphologic changes associated with
pulmonary vascular disease in 1958, and their 6 categories of vascular change have
remained the standard of comparison to the present.3
Since 1979, real-time 2-dimensional echocardiography has dramatically improved
the noninvasive anatomic assessment of ventricular septal defect.
Definition:
Ventricular septal defect is a developmental defect of the interventricular septum,
wherein communication between the cavities of the 2 ventricles is observed.
Embryology:
At 4-8 weeks' gestation, the single ventricular chamber is effectively divided into
2. This division is accomplished with the fusion of the membranous portion of the
ventricular septum, the endocardial cushions, and the bulbous cordis (proximal portion of
the truncus arteriosus).
The muscular portion of the ventricular septum grows cephalad as each
ventricular chamber enlarges, eventually meeting with the right and left ridges of the
bulbous cordis. The right ridge fuses with the tricuspid valve and the endocardial
cushions, separating the pulmonary valve from the tricuspid valve. The left ridge fuses
with a ridge of the interventricular septum, leaving the aortic ring in continuity with the
mitral ring.
The endocardial cushions develop concomitantly and finally fuse with the bulbar
ridges and the muscular portion of the septum.
The fibrous tissue of the membranous portion of the interventricular septum
makes the final closure and separates the 2 ventricles.
Anatomy:
The interventricular septum is a curvilinear complex structure and can be divided
into 4 zones by anatomic landmarks in the right ventricle (RV) as shown in the image
below. The RV has many heavy trabeculations. The stoutest of these is a Y -shaped
bundle (ie, the trabecula septomarginalis), which proceeds toward the apex and which
gives rise to the moderator band that courses transversely near the apex. The trabecula
septomarginalis is an important structure that helps in the identification of the RV,
regardless of its location in the chest. The 2 limbs of the Y travel superiorly, and the
anterior, or parietal, limb supports the pulmonic valve and the posterior limb (septal
band) extends to the membranous septum.
A: Image shows a ventricular septum viewed from the right side. It has the
following 4 components: inlet septum from the tricuspid annulus to the attachments of
the tricuspid valve (I); trabecular septum from inlet to apex and up to the smooth-walled
outlet (T); outlet septum, which extends to the pulmonary valve (O); and membranous
septum. B: Anatomic positions of the defects are as follows: outlet defect (a); papillary
muscle of the conus (b); perimembranous defect (c); marginal muscular defects (d);
central muscular defects (e); inlet defect (f); and apical muscular defects (g).
The 4 parts of the ventricular septum are as follows:
the inlet septum is smooth walled and extends from the septal attachments of the
tricuspid valve to the distal attachments of the tricuspid tensor apparatus. This region has
also been called the AV canal septum.4
The apical trabecular zone separates the coarse trabeculations of the RV from the
fine ones seen in the left ventricle (LV). Van Praagh et al refer to this as the muscular
septum or the ventricular sinus septum.4
The smooth-walled outlet or infundibular septum is separated from the
trabeculated portion of the RV by the septal band of the trabecula marginalis. Van Praagh
et al called this area the parietal band or the distal conal septum and refer to defects in
this area as conal septal defects.4
The last and the smallest region in the ventricular septum is the membranous
septum. This lies between the anterior and the septal tricuspid leaflets and below the right
and the noncoronary cusps of the aortic valve.
The 3 muscular components of the ventricular septum described above abut on the
membranous septum and fan out from it as triangles, with the apices touching this
septum. In the normal heart, the tricuspid and mitral valves are attached to the ventricular
septum at different levels so that the tricuspid-valve attachment is apically displaced
compared with the mitral-valve attachment. Therefore, a portion of the interventricular
septum, called the AV septum, lies between the right atrium (RA) and the LV. This
portion consists of a membranous part anteriorly and a muscular part posteriorly and is
usually present in most hearts with an isolated ventricular septal defect.
In the anterior aspect, the tricuspid-valve attachment divides the area of
membranous septum into an interventricular component (between the LV and RV) and an
AV component (between the LV and RA). When a ventricular septal defect is isolated,
the AV component of membranous septum is usually intact.
Classifications of ventricular septal defects
Many classifications of ventricular septal defects have been proposed. An
underlying classification that is surgically and clinically useful is described below. Please
also refer to the image shown below.
Schematic representation of the location of various types of ventricular septal
defects (VSDs) from the right ventricular aspect. A = Doubly committed subarterial
ventricular septal defect; B = Perimembranous ventricular septal defect; C = Inlet or
atrioventricular canal–type ventricular septal defect; D = Muscular ventricular
septal defect.
Perimembranous (infracristal, conoventricular) ventricular septal defects lie in the
LV outflow tract just below the aortic valve. Because they occur in the membranous
septum with defects in the adjacent muscular portion of the septum, they are subclassified
as perimembranous inlet, perimembranous outlet, or perimembranous muscular. These
are the most common types of ventricular septal defects and account for 80% of such
defects. Perimembranous ventricular septal defects are associated with pouches or
aneurysms of the septal leaflet of the tricuspid valve, which can partially or completely
close the defect. In addition, an LV-to-RA shunt may be associated with this defect.
Supracristal (conal septal, infundibular, subpulmonic, subarterial, subarterial
doubly committed, outlet) ventricular septal defects account for 5-8% of isolated
ventricular septal defects in the United States but 30% of isolated ventricular septal
defects in Japan. These defects lie beneath the pulmonic valve and communicate with the
RV outflow tract above the supraventricular crest and are associated with aortic
regurgitation secondary to the prolapse of the right aortic cusp.
Muscular ventricular septal defects (trabecular) are entirely bounded by the
muscular septum and are often multiple. The term Swiss-cheese septum has been used to
describe multiple muscular ventricular septal defects. Other subclassifications depend on
the location and include central muscular or midmuscular, apical, or marginal when the
defect is along the RV-septal junction. These ventricular septal defects account for 5-20%
of all defects. Any single defect observed from the LV aspect may have several openings
on the RV aspect.
Posterior (canal-type, endocardial cushion–type, AV septum–type, inlet,
juxtatricuspid) ventricular septal defects lie posterior to the septal leaflet of the tricuspid
valve. Although locations of posterior ventricular septal defects are similar to those of
ventricular septal defect observed with AV septal defects, they are not associated with
defects of the AV valves. About 8-10% of ventricular septal defects are of this type.
Pathophysiology:
A defect in the ventricular septum allows a communication between the systemic
and pulmonary circulations. As a result, flow moves from a region of high pressure to
low pressure (from the LV to the RV [ie, left-to-right shunt]). The pathophysiologic
effects of a ventricular septal defect are secondary to hemodynamic effects secondary to a
left-to-right shunt and changes in the pulmonary vasculature.
Left-to-right shunt
A left-to-right shunt at the ventricular level has 3 hemodynamic consequences:
increased LV volume load, excessive pulmonary blood flow, and reduced systemic
cardiac output.
Blood flow through the defect from the LV to the RV results in oxygenated blood
entering the pulmonary artery (PA). This extra blood in addition to the normal pulmonary
flow from the vena cava increases blood flow to the lungs and subsequently increases
pulmonary venous return into the left atrium (LA) and ultimately into the LV. This
increased LV volume results in LV dilatation and then hypertrophy. It increases the enddiastolic pressure and consequently LA pressure and then pulmonary venous pressure.
The increased pulmonary blood flow raises pulmonary capillary pressure, which
can increase pulmonary interstitial fluid. When this condition is severe, patients can
present with pulmonary edema. Therefore, both PA pressure and pulmonary venous
pressure are elevated in a ventricular septal defect. The increase in pulmonary venous
pressure is not seen with an atrial septal defect because LA pressures are low, as blood
can readily exit it through the atrial communication.
Finally, as blood is shunted through the ventricular septal defect away from the
aorta, cardiac output decreases, and compensatory mechanisms are stimulated to maintain
adequate organ perfusion. These mechanisms include increased catecholamine secretion
and salt and water retention by means of the renin-angiotensin system.
The degree of the left-to-right shunt determines the magnitude of the changes
described above. The left-to-right shunt depends on 2 factors: One is anatomic, and the
other is physiologic. The anatomic factor is the size of the ventricular septal defect. In a
normal heart, RV pressure is about 25% that of the LV. In a large ventricular septal
defect, this pressure difference is no longer maintained because a large hole offers no
resistance to blood flow. They are consequently called nonrestrictive ventricular septal
defects. On the other hand, in a small ventricular septal defect, the normal pressure
difference between the ventricles is maintained. These are called restrictive ventricular
septal defects because blood flow across the defects is somewhat restricted, such that the
normal pressure difference is maintained.
The physiologic factor is the resistance of the pulmonary vascular bed.
The location of the ventricular septal defect is irrelevant in terms of the degree of
the shunt.
Changes in the pulmonary vasculature
The terms pulmonary hypertension, high pulmonary resistance, and pulmonary
vascular disease are often confused.
Pulmonary hypertension merely indicates a high blood pressure in the pulmonary
circuit, and, depending on the duration, it can be reversible. Pulmonary resistance is a
function of numerous factors, including age, altitude, hematocrit, and diameter of the
pulmonary arterioles.
A neonate has increased resistance secondary to the increase in the media of the
pulmonary arterioles and this decreases the effective diameter of the vessels. In addition
to this, neonates have a relative polycythemia. This elevated pulmonary resistance
usually declines to adult levels by 6-8 weeks.
Pulmonary vascular disease is ultimately an irreversible condition and may occur
in individuals with a large left-to-right shunt over time. It may also occur in the absence
of a shunt; this condition is called primary pulmonary hypertension.
A characteristic series of histologic changes ranging from grade I to grade VI are
described.3
The ultimate consequences of pulmonary vascular obstructive disease are
irreversible vascular changes and pulmonary resistance equal to or exceeding systemic
resistance.
Causes:
Epidemiology: The incidence of ventricular septal defect in all live births is 1.53.5 cases per 1000 term infants and 4.5-7 cases per 1000 premature infants. The lowered
prevalence in adults is because many of the defects spontaneously close.
Inheritance:
At present, a multifactorial etiology based on an interaction between hereditary
predisposition and environmental influences is assumed to cause the defects. The
following questions have relevance to children, their family, and their parents alike:
What caused a child's heart defect?
What is the risk of the other children and grandchildren having a heart defect?
Maternal factors
Maternal diabetes: Maternal diabetes has long been recognized as a risk factor for
congenital cardiovascular malformations (CCVMs).
Maternal phenylketonuria: The risk of CCVMs remains high for infants of women
with poorly controlled elevated phenylalanine levels.
Maternal alcohol consumption and fetal alcohol syndrome: No population-based
data are available to define the range of risk alcohol consumption poses to the developing
cardiovascular system. Investigators from the Baltimore-Washington Infant Study
(BWIS) reported that maternal alcohol consumption was associated with only muscular
ventricular septal defect.8
Genetic risk factors (familial aggregation of cardiac and noncardiac
abnormalities)
The single largest determinant in the BWIS data set is the presence of a genetic
risk factor defined as a preoccurrence of a congenital cardiovascular defect in the family.
A family history of a cardiac or noncardiac defect in either a parent or a preceding
sibling is a major risk factor.
The incidence of ventricular septal defect in siblings of patients with the same
malformation is about 3 times that of the general population.
Ventricular septal defects have been reported in identical twins, but the frequency
of discordance is high, even in identical twins.
Familial congenital heart defects are often concordant by phenotype and
developmental mechanism. Among cases with ventricular septal defects, preoccurrence
of transposition, tetralogy of Fallot (TOF), and truncus arteriosus is higher than expected.
Genotype-phenotype correlation
The challenge for the next generation of pediatric cardiologists is to collaborate
with geneticists to define genotype-phenotype correlations.
Regarding genetic counseling and prospects for prevention, the single greatest
change in counseling regarding the recurrence risk for CCVMs is the recognition of
familial and chromosomally based defects. Thorough evaluation includes the following:
An accurate clinical diagnosis of the cardiovascular defect(s) organized in a
hierarchy (This is necessary to specify the type of ventricular septal defect.)
Carefully detailed noncardiac defects
Careful family history of first-degree and second-degree relatives, including
detailed analysis of pregnancy loss, racial origin, and consanguinity
A search for risk factors, such as gestational diabetes mellitus
Management:
Medical Care
Children with small ventricular septal defects (VSDs) are asymptomatic and have
an excellent long-term prognosis. Neither medical therapy nor surgical therapy is
indicated. Prophylactic antibiotic prophylaxis against endocarditis is no longer indicated.
Surgical closure
The first operation described for the treatment of a ventricular septal defect was a
palliative one and involved placing a restrictive band across the main PA.13 This was
proposed since pulmonary vascular disease as a result of unimpeded flow to the lungs
was recognized as a dreaded complication of a ventricular septal defect. This surgery was
popular for about 2 decades because it was associated with low mortality and morbidity.
Lillehei and associates performed the first intracardiac repair was at the
University of Minnesota in 1954 using a parent as an oxygenator and a pump in
controlled cross-circulation.14 In the 1970s, the current techniques ofhypothermia and
cardiopulmonary bypass were first reported.15,16,17 At present, direct surgical repair by
using cardiopulmonary bypass is the preferred surgical therapy in most centers. PA
banding, part of a 2-stage procedure, is largely reserved for critically ill infants with
multiple ventricular septal defect or for those with associated anomalies.
Acute Coronary Syndrome
The initial diagnosis of acute coronary syndrome (ACS) is based on history, risk
factors, and, to a lesser extent, ECG findings. The symptoms are due to myocardial
ischemia, the underlying cause of which is an imbalance between supply and demand of
myocardial oxygen.
Patients with ACS include those whose clinical presentations cover the following
range of diagnoses: unstable angina, non–ST-elevation myocardial infarction (NSTEMI),
and ST-elevation myocardial infarction (STEMI). This ACS spectrum concept is a useful
framework for developing therapeutic strategies.
Pathophysiology:
Myocardial ischemia is most often due to atherosclerotic plaques, which reduce
the blood supply to a portion of myocardium. Initially, the plaques allow sufficient blood
flow to match myocardial demand. When myocardial demand increases, the areas of
narrowing may become clinically significant and precipitate angina. Angina that is
reproduced by exercise, eating, and/or stress and is subsequently relieved with rest, and
without recent change in frequency or severity of activity that produce symptoms, is
called chronic stable angina. Over time, the plaques may thicken and rupture, exposing a
thrombogenic surface upon which platelets aggregate and thrombus forms. The patient
may note a change in symptoms of cardiac ischemia with a change in severity or of
duration of symptoms. This condition is referred to as unstable angina.
Patients with STEMI have a high likelihood of a coronary thrombus occluding the
infarct artery. Angiographic evidence of coronary thrombus formation may be seen in
more than 90% of patients with STEMI but in only 1% of patients with stable angina and
about 35-75% of patients with unstable angina or NSTEMI. However, not every STEMI
evolves into a Q-wave myocardial infarction (MI); likewise, a patient with NSTEMI may
develop Q waves.
The excessive mortality rate of coronary heart disease is primarily due to rupture
and thrombosis of the atherosclerotic plaque. Inflammation plays a critical role in plaque
destabilization and is widespread in the coronary and remote vascular beds. Systemic
inflammatory, thrombotic, and hemodynamic factors are relevant to the outcome.
Evidence indicates that platelets contribute to promoting plaque inflammation as well as
thrombosis. A new theory of unbalanced cytokine-mediated inflammation is emerging,
providing an opportunity for intervention.
A less common cause of angina is dynamic obstruction, which may be caused by
intense focal spasm of a segment of an epicardial artery (Prinzmetal angina). Coronary
vasospasm is a frequent complication in patients with connective tissue disease. Other
causes include arterial inflammation and secondary unstable angina. Arterial
inflammation may be caused by or related to infection. Secondary unstable angina occurs
when the precipitating cause is extrinsic to the coronary arterial bed, such as fever,
tachycardia, thyrotoxicosis, hypotension, anemia, or hypoxemia. Most patients who
experience secondary unstable angina have chronic stable angina as a baseline medical
condition.
Spontaneous and cocaine-related coronary artery dissection remains an unusual
cause of ACS and should be included in the differential diagnosis, especially when a
younger female or cocaine user is being evaluated. An early clinical suspicion of this
disease is necessary for a good outcome. Cardiology consultation should be obtained for
consideration for urgent percutaneous coronary intervention.
Although rare, pediatric and adult ACS may result from the following
(see Myocardial Infarction in Childhood):
ACS may occur with Marfan syndrome; Kawasaki disease; Takayasu arteritis; or
cystic medial necrosis with aortic root dilatation, aneurysm formation, and dissection into
the coronary artery.
Anomalous origin of the left coronary artery from the pulmonary artery may
occur as unexplained sudden death in a neonate.
Coronary artery ostial stenosis may occur after repair of a transposition of the
great arteries in the neonatal period.
An aberrant left main coronary artery with its origin at the right sinus of Valsalva
may cause ACS, especially with exertion.
Traumatic myocardial infarction can occur in patients at any age.
Accelerated atherosclerosis is known to occur in cardiac transplant recipients on
immunosuppressive therapy.
ACS may occur with progeria.
Irrespective of the cause of unstable angina, the result of persistent ischemia is
MI.
Physical
Physical examination results are frequently normal. If chest pain is ongoing, the
patient will usually lie quietly in bed and may appear anxious, diaphoretic, and pale.
Hypertension may precipitate angina or reflect elevated catecholamine levels due
to either anxiety or exogenous sympathomimetic stimulation.
Hypotension indicates ventricular dysfunction due to myocardial ischemia,
infarction, or acute valvular dysfunction.
Jugular venous distention
Third heart sound (S3) may be present.
A new murmur may reflect papillary muscle dysfunction.
Rales on pulmonary examination may suggest left ventricular (LV) dysfunction or
mitral regurgitation.
Presence of a fourth heart sound (S4) is a common finding in patients with poor
ventricular compliance due to preexisting ischemic heart disease or hypertension.
Management:
Prehospital Care
Generally, patients transported with chest pain should initially be managed under
the assumption that the pain is ischemic in origin. Prehospital interventions should be
guided by the nature of the presenting complaint, individual risk factors, and associated
symptoms (eg, breathing difficulty, hemodynamic instability, appearance of ectopy).
Airway, breathing, and circulation should be rapidly assessed with institution of CPR,
ACLS-guided interventions, or other measures as indicated for the unstable patient.
The goals of treatment are to preserve patency of the coronary artery, augment
blood flow through stenotic lesions, and reduce myocardial oxygen demand. All patients
should receive antiplatelet agents, and patients with evidence of ongoing ischemia should
receive aggressive medical intervention until signs of ischemia, as determined by
symptoms and ECG, resolve.
Syndrome X
Also known as Metabolic syndrome, Insulin resistance syndrome; Syndrome X
Metabolic syndrome is a name for a group of risk factors that occur together and
increase the risk for coronary artery disease, stroke, and type 2 diabetes.
Causes, incidence, and risk factors:
Metabolic syndrome is becoming more and more common in the United States.
Researchers are not sure whether the syndrome is due to one single cause, but all of the
syndrome's risk factors are related to obesity.
Metabolic syndrome is associated with many conditions and risk factors. The two
most important risk factors are:
Extra weight around the middle of the body (central obesity). The body may be
described as "apple-shaped."
Insulin resistance, in which the body cannot use insulin effectively. Insulin is
needed to help control the amount of sugar in the body.
Insulin helps blood sugar (glucose) enter cells. If you have insulin resistance, your
body doesn't respond to insulin, and blood sugar cannot get into cells. As a result, the
body produces more and more insulin. Insulin and blood sugar levels rise, affecting
kidney function and raising the level of blood fats, such as triglycerides.
Other risk factors include:
Aging
Genes that make you more likely to develop this condition (genetic
predisposition)
Hormonal changes
Lack of exercise
Symptoms
Extra weight around your waist (central or abdominal obesity)
Signs and tests:
Metabolic syndrome is present if you have three or more of the following signs:
Blood pressure equal to or higher than 130/85 mmHg
Fasting blood sugar (glucose) equal to or higher than 100 mg/dL
Large waist circumference (length around the waist):
Men - 40 inches or more
Women - 35 inches or more
Low HDL cholesterol:
Men - under 40 mg/dL
Women - under 50 mg/dL
Triglycerides equal to or higher than 150 mg/dL
Tests that may be done to diagnose metabolic syndrome include:
Blood pressure measurement
Glucose test
HDL cholesterol level
LDL cholesterol level
Total cholesterol level
Triglyceride level
Treatment
The goal of treatment is to reduce your risk of heart disease and diabetes. Your
doctor will recommend lifestyle changes or medicines to help reduce your blood
pressure, LDL cholesterol, and blood sugar.
Recommendations include:
Lose weight. The initial goal is to lose between 7 and 10% of your current weight.
This generally means that you need to eat 500 - 1,000 fewer calories per day.
Get 30 minutes of moderate intensity exercise, such as walking, 5 - 7 days per
week.
Lower your cholesterol using weight loss, exercise, and cholesterol lowering
medications, if needed.
Lower your blood pressure using weight loss, exercise, and medications, if
needed.
Some people may need daily low-dose aspirin.
People who smoke should quit.
Prognosis:
People with metabolic syndrome have an increased long-term risk for developing
cardiovascular disease and type 2 diabetes.
Complications:
Atherosclerosis
Diabetes
Heart attack
Kidney disease
Nonalcoholic fatty liver disease
Peripheral artery disease
Stroke
Calling your health care provider
Call your health care provider if you have signs or symptoms of this condition.
Prevention:
Preventing (and managing) the condition involves:
Eating a diet low in fat, with a variety of fruits, vegetables, and whole-grain
products
Getting regular exercise, at least 30 minutes of moderate activity almost every day
Losing weight so that your body mass index (BMI) is less than 25
Managing blood pressure and blood sugar
Not smoking
Trying to include fish, preferably oily fish, in your diet at least twice a week
Dressler's syndrome
Dressler's syndrome is a secondary form of pericarditis that occurs in the setting
of injury to the heart or the pericardium (the outer lining of the heart).
Dressler's syndrome is also known as postmyocardial infarction syndrome[1] and
the term is sometimes used to refer to post-pericardiotomy pericarditis.
(It should not be confused with the Dressler's syndrome
of haemoglobinuria named for Lucas Dressler, who characterized it in 1854)
Clinical Presentation:
Dressler's syndrome is largely a self limiting disease that very rarely leads to
pericardial tamponade. The syndrome consists of a persistent low-grade fever, chest
pain (usually pleuritic in nature), a pericardial friction rub, and /or a pericardial effusion.
The symptoms tend to occur 2 weeks post myocardial infarction, but can be delayed for a
few months after infarction. It tends to subside in a few days. An elevated ESR is an
objective laboratory finding.
Causes:
It is believed to result from an autoimmune inflammatory reaction to myocardial
neo-antigens.
Dressler's syndrome is associated with myocardial infarction (heart attack). A
similar pericarditis can be associated with any pericardiotomy or trauma to the
percardium or heart surgery.
Wolff-Parkinson-White syndrome
Wolff-Parkinson-White syndrome is a heart condition in which there is an extra
electrical pathway (circuit) in the heart. The condition can lead to episodes of rapid heart
rate (tachycardia).
Wolff-Parkinson-White is one of the most common causes of fast heart rate
disorders in infants and children.
Causes, incidence, and risk factors:
Normally, electrical signals in the heart go through a pathway that helps the heart
beat regularly. The wiring of the heart prevents extra beats from occurring and keeps the
next beat from happening too soon.
In people with Wolff-Parkinson-White syndrome, there is an extra, or accessory,
pathway that may cause a very rapid heart rate. This is called supraventricular
tachycardia.
Symptoms:
How often the rapid heart rate occurs depends on the patient. Some people with
Wolff-Parkinson-White syndrome may have just a few episodes of rapid heart rate.
Others may have the rapid heart rate once or twice a week. Sometimes there are no
symptoms, and the condition is detected when a heart tests are done for another reason.
A person with WPW syndrome may have:
Chest pain or chest tightness
Dizziness
Light-headedness
Fainting
Palpitations (a sensation of feeling your heart beat)
Shortness of breath
Signs and tests:
An exam performed during a tachycardia episode will reveal a heart rate greater
than 230 beats per minute andblood pressure that is normal or low. A normal heart rate is
60 - 100 beats per minute in adults, and under 150 beats per minute in neonates, infants,
and small children.
If the patient is currently not having tachycardia, the physical exam may be
completely normal.
A test called EPS may help identify the location of the extra electrical pathway.
Wolff-Parkinson-White syndrome may be revealed by the following tests:
ECG (electrocardiogram) may show an abnormality called a "delta" wave.
Continuous ambulatory monitoring (Holter monitor)
Expectations (prognosis)
Catheter ablation cures this disorder in most patients. The success rate for the
procedure ranges between 85 - 95%. Success rate will vary depending on location of
accessory pathway and number of accessory pathways.
Complications:
Complications of surgery
Reduced blood pressure (caused by continous rapid heart rate)
Heart failure
Side effects of medications
The most severe form of a rapid heart beat is atrial fibrillation. It may rapidly lead
to shock, and requires emergency treatment (cardioversion).
Romano-Ward Syndrome
Long QT Syndrome, Autosomal Dominant; Romano-Ward Long QT Syndrome.
Includes: LQT1, LQT2, LQT3, LQT5, LQT6
Disease characteristics. Romano-Ward syndrome (RWS) is purely a cardiac
electrophysiologic disorder, characterized by QT prolongation and T-wave abnormalities
on the ECG and the ventricular tachycardia torsade de pointes (TdP). TdP is usually selfterminating, thus causing a syncopal event, the most common symptom in individuals
with RWS. Syncope typically occurs during exercise and high emotions, less frequently
at rest or during sleep, and usually without warning. In some instances, TdP degenerates
to ventricular fibrillation and causes aborted cardiac arrest (if the individual is
defibrillated) or sudden death. Approximately 50% of individuals with a disease-causing
mutation in one of the genes associated with RWS have symptoms, usually one to a few
syncopal spells. While cardiac events may occur from infancy through middle age, they
are most common from the pre-teen years through the 20s.
Diagnosis / testing. Diagnosis of RWS is established by prolongation of the QTc
interval in the absence of specific conditions known to lengthen it (for example, QTprolonging drugs) and/or molecular genetic testing of the following genes known to be
associated with RWS: KCNQ1 (locus name LQT1), KCNH2 (locus
nameLQT2), SCN5A (locus name LQT3), KCNE1 (locus name LQT5),
and KCNE2 (locus name LQT6). In the past, approximately 30% of families meeting
clinical diagnostic criteria for RWS did not have detectable mutations in any one of the
five previously associated genes using current test methods; at this time, it is not known
what proportion of these mutation-negative families may have a mutation in the recently
identified SCN4B gene(proposed locus name LQT10).
Inheritance:
Romano-Ward syndrome is inherited in anautosomal dominant pattern.
Romano-Ward syndrome is inherited in an autosomal dominant pattern. It is the
most common form of inherited long QT syndrome, affecting an estimated 1 in 5,000
people worldwide, although more people may be affected but never experience any signs
or symptoms of the condition.
Causes:
Mutations in the ANK2, KCNE1, KCNE2, KCNH2, KCNQ1, and SCN5A genes
cause Romano-Ward syndrome. The proteins made by most of these genes form channels
that transportpositively-charged ions, such as potassium and sodium, in and out of cells.
In cardiac muscle, these ion channels play critical roles in maintaining the heart's normal
rhythm. Mutations in any of these genes alter the structure or function of channels, which
changes the flow of ions between cells. A disruption in ion transport alters the way the
heart beats, leading to the abnormal heart rhythm characteristic of Romano-Ward
syndrome.
Unlike most genes related to Romano-Ward syndrome, the ANK2 gene does not
produce an ion channel. The protein made by the ANK2 gene ensures that other proteins,
particularly ion channels, are inserted into the cell membrane appropriately. A mutation
in the ANK2 gene likely alters the flow of ions between cells in the heart, which disrupts
the heart's normal rhythm and results in the features of Romano-Ward syndrome.
This article incorporates public domain text from The U.S. National Library of
Medicine
Management:
An imbalance between the right and left sides of the sympathetic nervous system
may play a role in the etiology of this syndrome. The imbalance can be temporarily
abolished with a left stellate ganglion block, which shorten the QT interval. If this is
successful, surgical ganglionectomy can be performed as a permanent treatment.[1]
Romano-Ward syndrome, is the major variant of long QT syndrome. It is a
condition that causes a disruption of the heart's normal rhythm. This disorder is a form
of long QT syndrome, which is a heart condition that causes the cardiac muscle to take
longer than usual to recharge between beats. If untreated, the irregular heartbeats can lead
to fainting, seizures, or sudden death.
Jervell and Lange-Nielsen syndrome
Jervell and Lange-Nielsen syndrome, a type of long QT syndrome, causes
the cardiac muscle to take longer than usual to recharge between beats. If untreated, the
irregular heartbeats, called arrhythmias, can lead to fainting, seizures, or sudden death.
The disorder also contributes to hearing loss.
Genetic prevalence
Jervell and Lange-Nielsen syndrome has an autosomal recessive pattern of
inheritance.
This condition is an autosomal recessive disorder that affects an estimated 1.6 to 6
in 1 million children, and is responsible for less than 10 percent of all cases of long QT
syndrome.
Mutations in the KCNE1 and KCNQ1 genes cause Jervell and Lange-Nielsen
syndrome. The proteins produced by these two genes work together to form a potassium
channel that transports positively charged potassium ions out of cells. The movement of
potassium ions through these channels is critical for maintaining the normal functions of
the inner ear and cardiac muscle.
About 90 percent of cases of Jervell and Lange-Nielsen syndrome are caused by
mutations in the KCNQ1 gene. KCNE1 mutations are responsible for the remaining 10
percent of cases. Mutations in these genes alter the usual structure and function of
potassium channels or prevent the assembly of normal channels. These changes disrupt
the flow of potassium ions in the inner ear and in cardiac muscle, leading to the hearing
loss and irregular heart rhythm characteristic ofJervell and Lange-Nielsen syndrome.
Sick sinus syndrome
Bradycardia-tachycardia syndrome; Sinus node dysfunction
Last reviewed: May 4, 2010.
Sick sinus syndrome is a collection of heart rhythm disorders that include:
Sinus bradycardia -- slow heart rates from the natural pacemaker of the heart
Tachycardias -- fast heart rates
Bradycardia-tachycardia -- alternating slow and fast heart rhythms
Causes, incidence, and risk factors:
Sick sinus syndrome is relatively uncommon. Sinus bradycardia occurs more
often than the other types.
Tachycardias that start in the upper chambers of the heart are also common forms.
These include atrial fibrillation, atrial flutter/tachycardia, and supraventricular
tachycardia. A period of elevated heart rates is typically followed by very slow heart rates
when the tachycardia ends.
Abnormal heart rhythms are often made worse by medications such as digitalis,
calcium channel blockers, beta-blockers, and anti-arrhythmics. Disorders that cause
scarring, degeneration, or damage to the conduction system of the heart can cause sick
sinus syndrome.
Sick sinus syndrome usually occurs in people older than 50, in whom the cause is
often a nonspecific, scar-like degeneration of the heart's conduction system.
In children, a common cause of sick sinus syndrome is heart surgery, especially
on the upper chambers.
Coronary artery disease, high blood pressure, and aortic and mitral valve diseases
may be associated with sick sinus syndrome, although those diseases may have nothing to
do with the syndrome.
Symptoms:
Usually, no symptoms occur. Symptoms that do occur are nonspecific and may
mimic other disorders.
Symptoms may include:
Chest pain or angina
Confusion or other changes in mental status
Fainting or near-fainting
Fatigue
Dizziness or light-headedness
Sensation of feeling the heart beat (palpitations)
Shortness of breath
Signs and tests
The patient's heart rate may be very slow at any time. Blood pressure may be
normal or low.
Sick sinus syndrome may cause symptoms of heart failure to occur or worsen.
Sick sinus syndrome is diagnosed when the symptoms occur only during episodes of
arrhythmia. However, this often is difficult to prove.
An ECG may show various abnormal heart rhythms related to this syndrome.
Holter monitoring is an effective tool for diagnosing sick sinus syndrome because
of the episodic nature of the disorder. Extremely slow heart rate and prolonged pauses
may be seen during Holter monitoring, along with episodes of atrial tachycardias.
An EPS (intracardiac electrophysiology study) is a very specific test for this
disorder, although it is often unable to confirm the diagnosis. It is not often needed.
Exercise testing has not proven particularly effective as a screening tool
xpectations (prognosis)
The syndrome is progresssive, which means it slowly gets worse.
The long-term outlook is excellent for those who have a permanent pacemaker
implanted.
Complications:
Angina
Decreased exercised capacity
Falls or injury caused by fainting
Heart failure
Inadequate heart pumping
Bradycardia-tachycardia syndrome is a variant of sick sinus syndrome in which
slow arrhythmias and fast arrhythmias alternate.
Mitral valve Prolapse Syndrome
Mitral valve prolapse syndrome (MVP) is a valvular heart disease characterized
by the displacement of an abnormally thickened mitral valve leaflet into the left
atrium during systole. There are various types of MVP, broadly classified as classic and
nonclassic. In its nonclassic form, MVP carries a low risk of complications. In severe
cases of classic MVP, complications include mitral regurgitation, infective
endocarditis, congestive heart failure, and—in rare circumstances—cardiac arrest, usually
resulting in sudden death.
The diagnosis of MVP depends upon echocardiography, which uses ultrasound to
visualize the mitral valve. Early studies estimated a prevalence of 38% among healthy
teenagers; with improved echocardiographic techniques and clear diagnostic criteria, the
true prevalence of MVP is estimated at 2-3% of the population.
Subtypes
Diagnosis of mitral valve prolapse is based on
modern echocardiographictechniques which can pinpoint abnormal leaflet thickening and
other related pathology.
Prolapsed mitral valves are classified into several subtypes, based on leaflet
thickness, concavity, and type of connection to the mitral annulus. Subtypes can be
described as classic, nonclassic, symmetric, asymmetric, flail, or non-flail
All measurements below refer to adult patients; applying them to children may be
misleading.
Classic versus nonclassic
Prolapse occurs when the mitral valve leaflets are displaced more than
2 mm above the mitral annulus high points. The condition can be further divided into
classic and nonclassic subtypes based on the thickness of the mitral valve leaflets: up to
5 mm is considered nonclassic, while anything beyond 5 mm is considered classic MVP.
Symmetric versus asymmetric
Classical prolapse may be subdivided into symmetric and asymmetric, referring to
the point at which leaflet tips join the mitral annulus. In symmetric coaptation, leaflet tips
meet at a common point on the annulus. Asymmetric coaptation is marked by one leaflet
displaced toward the atrium with respect to the other. Patients with asymmetric prolapse
are susceptible to severe deterioration of the mitral valve, with the possible rupture of the
chordae tendineae and the development of a flail leaflet.
Flail versus non-flail
Asymmetric prolapse is further subdivided into flail and non-flail. Flail prolapse
occurs when a leaflet tip turns outward, becoming concave toward the left atrium,
causing the deterioration of the mitral valve. The severity of flail leaflet varies, ranging
from tip eversion to chordal rupture. Dissociation of leaflet and chordae tendineae
provides for unrestricted motion of the leaflet (hence "flail leaflet"). Thus patients with
flail leaflets have a higher prevalence of mitral regurgitation than those with the non-flail
subtype.
Diagnosis:
Transesophageal echocardiogram of mitral valve prolapse.
Signs and symptoms:
Some patients with MVP experience heart palpitations, atrial fibrillation,
or syncope, though the prevalence of these symptoms does not differ significantly from
the general population. Between 11 and 15% of patients experience moderate chest
pain and shortness of breath. These symptoms are most likely not caused directly by the
prolapsing mitral valve, but rather by the mitral regurgitation that often results from
prolapse. A correlation has been reported between bipolar disorder and mitral valve
prolapse.
For unknown reasons, MVP patients tend to have a low body mass index (BMI)
and are typically leaner than individuals without MVP.[4][7]
Murmur
Upon auscultation of an individual with mitral valve prolapse, a mid-systolic
click, followed by a late systolic murmur heard best at the apex is common.
In contrast to most other heart murmurs, the murmur of mitral valve prolapse is
accentuated by standing and valsalva maneuver (earlier systolic click and longer murmur)
and diminished with squatting (later systolic click and shorter murmur). The only other
heart murmur that follows this pattern is the murmur of hypertrophic cardiomyopathy. A
MVP murmur can be distinguished from a hypertrophic cardiomyopathymurmur by 1)
the presence of a mid-systolic click which is virtually diagnostic of MVP, and 2) the fact
that hand grip maneuver intensifies the murmur of MVP[citation needed] and diminishes
the murmur of hypertrophic cardiomyopathy. The hand grip maneuver also diminishes
the duration of the murmur and delays the timing of the mid-systolic click.[14]
Both valsalva maneuver and standing decrease venous return to the heart thereby
decreasing left ventricular diastolic filling (preload) and causing more laxity on
the chordae tendineae. This allows the mitral valve to prolapse earlier in systole, leading
to an earlier systolic click (i.e. closer to S1), and a longer murmur. Hand grip maneuver
increases total peripheral resistance (afterload) and therefore increases back pressure on
the mitral valve resulting in a more intense murmur without changing the timing of the
systolic click.
Complications:
Mitral regurgitation
Mitral valve prolapse can result inmitral regurgitation, shown here, in which
blood abnormally flows from the left ventricle into the left atrium.
Mitral valve prolapse is frequently associated with mild mitral
regurgitation,[16] where blood aberrantly flows from the left ventricle into the left atrium
during systole. In the United States, MVP is the most common cause of severe, nonischemic mitral regurgitation. This is occasionally due to rupture of the chordae
tendineae that support the mitral valve.
Sudden death
The MVP complications mitral regurgitation and congestive heart failure may, in
turn, causearrhythmias and atrial fibrillation that may progress and lead to sudden death.
However, there is no evidence that a prolapsed valve itself contributes to such arrythmias.
Prognosis:
Generally, MVP is a benign disorder. However, MVP patients with a murmur, not
just an isolated click, have a general mortality rate that is increased by 15-20%.[8] The
major predictors of mortalityare the severity of mitral regurgitation and the ejection
fraction.
Down syndrome
Trisomy 21
Down syndrome is a genetic condition in which a person has
47 chromosomes instead of the usual 46.
Causes, incidence, and risk factors
In most cases, Down syndrome occurs when there is an extra copy of
chromosome 21. This form of Down syndrome is called Trisomy 21. The extra
chromosome causes problems with the way the body and brain develop.
Down syndrome is the most common single cause of human birth defects.
Symptoms:
Down syndrome symptoms vary from person to person and can range from mild
to severe. However, children with Down syndrome have a widely recognized appearance.
The head may be smaller than normal and abnormally shaped. For example, the
head may be round with a flat area on the back. The inner corner of the eyes may be
rounded instead of pointed.
Common physical signs include:
Decreased muscle tone at birth
Excess skin at the nape of the neck
Flattened nose
Separated joints between the bones of the skull (sutures)
Single crease in the palm of the hand
Small ears
Small mouth
Upward slanting eyes
Wide, short hands with short fingers
White spots on the colored part of the eye (Brushfield spots)
Physical development is often slower than normal. Most children with Down
syndrome never reach their average adult height.
Children may also have delayed mental and social development. Common
problems may include:
Impulsive behavior
Poor judgment
Short attention span
Slow learning
As children with Down syndrome grow and become aware of their limitations,
they may also feel frustration and anger.
Many different medical conditions are seen in people with Down syndrome,
including:
Birth defects involving the heart, such as an atrial septal defect or ventricular
septal defect
Dementia may be seen
Eye problems, such as cataracts (most children with Down syndrome need
glasses)
Early and massive vomiting, which may be a sign of a gastrointestinal blockage,
such as esophageal atresia and duodenal atresia
Hearing problems, probably caused by regular ear infections
Hip problems and risk of dislocation
Long-term (chronic) constipation problems
Sleep apnea (because the mouth, throat, and airway are narrowed in children with
Down syndrome)
Teeth that appear later than normal and in a location that may cause problems
with chewing
Underactive thyroid (hypothyroidism)
Signs and tests:
A doctor can often make an initial diagnosis of Down syndrome at birth based on
how the baby looks. The doctor may hear a heart murmur when listening to the baby's
chest with a stethoscope.
A blood test can be done to check for the extra chromosome and confirm the
diagnosis. Other tests that may be done include:
Echocardiogram to check for heart defects (usually done soon after birth)
ECG
X-rays of the chest and gastrointestinal tract
Persons with Down syndrome need to be closely screened for certain medical
conditions. They should have:
Eye exam every year during infancy
Hearing tests every 6 - 12 months, depending on age
Dental exams every 6 months
X-rays of the upper or cervical spine between ages 3 - 5 years
Pap smears and pelvic exams beginning during puberty or by age 21
Thyroid testing every 12 months
Expectations (prognosis)
Persons with Down syndrome are living longer than ever before. Although many
children have physical and mental limitations, they can live independent and productive
lives well into adulthood.
About half of children with Down syndrome are born with heart problems,
including atrial septal defect, ventricular septal defect, and endocardial cushion defects.
Severe heart problems may lead to early death.
Persons with Down syndrome have an increased risk for certain types of
leukemia, which can also cause early death.
The level of mental retardation varies from patient to patient, but is usually
moderate. Adults with Down syndrome have an increased risk for dementia.
Complications:
Airway blockage during sleep
Compression injury of the spinal cord
Endocarditis
Eye problems
Frequent ear infections and increased risk of other infections
Hearing loss
Heart problems
Gastrointestinal blockage
Weakness of the back bones at the top of the neck
Turner syndrome
Turner syndrome or Ullrich-Turner syndrome (also known as "Gonadal
dysgenesis"[1]:550) encompasses several conditions, of which monosomy X (absence of
an entire sex chromosome, the Barr body) is most common. It is a chromosomal
abnormality in which all or part of one of the sex chromosomes is absent (unaffected
humans have 46 chromosomes, of which two are sex chromosomes). Typical females
have two X chromosomes, but in Turner syndrome, one of those sex chromosomes is
missing or has other abnormalities. In some cases, the chromosome is missing in some
cells but not others, a condition referred to as mosaicism[2] or 'Turner mosaicism'.
Occurring in 1 in 2000[3] – 1 in 5000 phenotypic females,[4] the syndrome
manifests itself in a number of ways. There are characteristic physical abnormalities, such
as short stature,swelling, broad chest, low hairline, low-set ears, and webbed
necks.[5] Girls with Turner syndrome typically experience gonadal dysfunction (nonworking ovaries), which results inamenorrhea (absence of menstrual cycle) and sterility.
Concurrent health concerns are also frequently present, including congenital heart
disease, hypothyroidism (reduced hormonesecretion by
the thyroid), diabetes, vision problems, hearing concerns, and many autoimmune
diseases.[6] Finally, a specific pattern of cognitive deficits is often observed, with
particular difficulties in visuospatial, mathematical, and memory areas.[7]
In 1938, Henry Turner first described Turner syndrome, which is one of the most
common chromosomal abnormalities.1 More than 95% of adult women with Turner
syndrome exhibit short stature andinfertility.
Lymphedema of the feet in an infant is shown. The toes have the characteristic
sausagelike appearance.
Hyperconvex nails in Turner syndrome. Note U-shaped cross section.
Signs and symptoms:
Lymphedema, puffy legs of a newborn with Turner syndrome
Common symptoms of Turner syndrome include:
Short stature
Lymphedema (swelling) of the hands and feet
Broad chest (shield chest) and widely spaced nipples
Low hairline
Low-set ears
Reproductive sterility
Rudimentary ovaries gonadal streak (underdeveloped gonadal structures)
Amenorrhoea, or the absence of a menstrual period
Increased weight, obesity
Shield shaped thorax of heart
Shortened metacarpal IV
Small fingernails
Characteristic facial features
Webbed neck from cystic hygroma in infancy
Coarctation of the aorta
Bicuspid aortic valve
Poor breast development
Horseshoe kidney
Visual impairments sclera, cornea, glaucoma, etc.
Ear infections and hearing loss
High waist-to-hip ratio (the hips are not much bigger than the waist)
Attention Deficit/Hyperactivity Disorder (problems with concentration, memory
and attention)
Nonverbal Learning Disability (problems with math, social skills and spatial
relations)
Other symptoms may include a small lower jaw (micrognathia), cubitus
valgus (turned-in elbows), soft upturned nails, palmar crease, anddrooping eyelids. Less
common are pigmented moles, hearing loss, and a high-arch palate (narrow maxilla).
Turner syndrome manifests itself differently in each female affected by the condition, and
no two individuals will share the same symptoms.
Cause
Risk factors for Turner syndrome are not well known.
Genetic mosaicism (46XX/45XO) is most often implicated,
alongside nondisjunction(45XO) and partial monosomy (46XX). Nondisjunctions
increase with maternal age, such as for Down syndrome, but that effect is not clear for
Turner syndrome. It is also unknown if there is a genetic predisposition present that
causes the abnormality, though most researchers and doctors treating Turners women
agree that this is highly unlikely. In 75% of cases inactivated X chromosome is paternal
origin. There is currently no known cause for Turner syndrome, though there are several
theories surrounding the subject. The only solid fact that is known today is that during
conception part or all of the second sex chromosome is not transferred to the fetus.[8] In
other words, these females do not have Barr bodies, which are those X chromosomes
inactivated by the cell.
Diagnosis
45,X karyotype, showing an unpaired X at the lower right
Turner syndrome may be diagnosed by amniocentesis during pregnancy.
Sometimes, fetuses with Turner syndrome are identified by abnormal ultrasound findings
(i.e. heart defect, kidney abnormality, cystic hygroma, ascites). Although the recurrence
risk is not increased, genetic counseling is often recommended for families who have had
a pregnancy or child with Turner syndrome.
A test, called a karyotype or a chromosome analysis, analyzes the chromosomal
composition of the individual. This is the test of choice to diagnose Turner syndrome.
Prognosis:
While most of the physical findings are harmless, there can be significant medical
problems associated with the syndrome.
Cardiovascular
Price et al. (1986 study of 156 female patients with Turner syndrome) showed a
significantly greater number of deaths from diseases of the circulatory system than
expected, half of them due to congenital heart defects—mostly preductal coarctation of
the aorta. When patients with congenital heart disease were omitted from the sample of
the study, the mortality from circulatory disorders was not significantly increased.[9]
Cardiovascular malformations are a serious concern as it is the most common
cause of death in adults with Turner syndrome. It takes an important part in the 3-fold
increase in overall mortality and the reduced life expectancy (up to 13 years) associated
with Turner syndrome.
Epidemiology:
Approximately 99 percent of all fetuses with Turner syndrome result in
spontaneous termination during the first trimester.[29] Turner syndrome accounts for
about 10 percent of the total number of spontaneous abortions in the United
States.[citation needed] The incidence of Turner syndrome in live female births is
believed to be around 1 in 2000.
Noonan syndrome
Noonan syndrome is a genetic disorder that causes abnormal development of
multiple parts of the body. It used to be called Turner-like syndrome because certain
symptoms (webbing of neck and abnormally shaped chest) resembled those seen
in Turner syndrome.
Causes, incidence, and risk factors:
Defects in four genes (KRAS, PTPN11, RAF1, SOS1) can cause Noonan
syndrome. About half of those affected by Noonan syndrome have a PTPN11 mutation.
Persons with a defect in the KRAS gene have a more severe form of Noonan syndrome.
Those with defects in the RAF1 gene tend to have a particular heart problem
(hypertrophic cardiomyopathy). Problems with these genes cause certain proteins
involved in growth and development to become overactive.
Noonan syndrome is inherited, which means it is passed down through families. It
is an autosomal dominantcondition. This means that only one parent has to provide the
faulty gene for the baby to have the syndrome. However, the fact that some children do
not have a parent with Noonan syndrome likely means that some cases are not inherited.
Symptoms:
Delayed puberty
Down-slanting or wide-set eyes
Hearing loss (varies)
Low-set or abnormally shaped ears
Mild mental retardation (only in about 25% of cases)
Sagging eyelids (ptosis)
Short stature
Small penis
Undescended testicles
Unusual chest shape (usually a sunken chest called pectus excavatum)
Webbed and short-appearing neck
Signs and tests:
Examination may show an extra fold of skin above the eyes near the nose
(epicanthal folds) and arms that may be held at an unusual angle.
There may be signs of congenital heart disease (especially pulmonary stenosis,
occasionally ASD).
Blood tests to look at platelet count and blood factors may reveal signs of a
bleeding tendency.
Specific tests depend on what the symptoms are. For example, if there are signs of
heart disease, an EKG,chest x-ray, or echocardiogram may be recommended. Hearing
tests are recommended for those who have signs of decreased hearing.
Genetic testing can identify the mutations in the four genes which cause Noonan
syndrome.
Management:
There is no single treatment for Noonan syndrome. Treatment focuses on the
individual symptoms. Growth hormone has been used successfully to treat short stature in
some persons with Noonan syndrome.
Prognosis:
The expected outcome depends on the extent and severity of symptoms. Patients
can lead normal lives.
Complications:
Accumulation of fluid in tissues of body (lymphedema, cystic hygroma)
Failure to thrive in infants
Low self-esteem
Male infertility in those with both testes undescended
Problems with the structure of the heart
Short stature
Social difficulties related to physical problems
Williams syndrome
Williams syndrome (WS or WMS; also Williams–Beuren syndrome or WBS) is a
rareneurodevelopmental disorder caused by a deletion of about 26 genes from the long
arm ofchromosome 7.[1] It is characterized by a distinctive, "elfin" facial appearance,
along with a lownasal bridge; an unusually cheerful demeanor and ease with
strangers; developmental delaycoupled with strong language skills; and cardiovascular
problems, such as supravalvular aortic stenosis and transient hypercalcaemia.
Causes, incidence, and risk factors:
Williams syndrome is a rare condition caused by missing genes. Parents may not
have any family history of the condition. However, a person with Williams syndrome has
a 50% chance of passing the disorder on to each of his or her children. The cause usually
occurs randomly.
Williams syndrome occurs in about 1 in 8,000 births.
One of the 25 missing genes is the gene that produces elastin, a protein that allows
blood vessels and other tissues in the body to stretch. It is likely that having only one
copy of this gene results in the narrowing of blood vessels seen in this condition.
Symptoms:
Delayed speech that may later turn into strong speaking ability and strong
learning by hearing
Developmental delay
Easily distracted, attention deficit disorder (ADD)
Feeding problems including colic, reflux, and vomiting
Inward bend of the small finger (clinodactyly)
Learning disorders
Mild to moderate mental retardation
Personality traits including being very friendly, trusting strangers, fearing loud
sounds or physical contact, and being interested in music
Short compared to the rest of the person's family
Sunken chest (pectus excavatum)
Unusual appearance of the face
Flattened nasal bridge with small upturned nose
Long ridges in the skin that run from the nose to the upper lip (philtrum)
Prominent lips with an open mouth
Skin that covers the inner corner of the eye (epicanthal folds)
Partially missing teeth, defective tooth enamel, or small, widely spaced teeth
Signs and tests:
Blood vessel narrowing including supravalvular aortic stenosis, pulmonary
stenosis, and pulmonary artery stenosis
Farsightedness
High blood calcium level (hypercalcemia) that may cause seizures and rigid
muscles
High blood pressure
Slack joints that may change to stiffness as patient gets older
Unusual pattern ("stellate" or star-like) in iris of the eye
Leopard Syndrome
Leopard syndrome (also known as Cardiocutaneous syndrome, Gorlin syndrome
II, Lentiginosis profusa syndrome, Progressive cardiomyopathic lentiginosis,:550 CaputeRimoin-Konigsmark-Esterly-Richardson syndrome, or Moynahan syndrome) - is part of a
group called Ras/MAPK pathway syndromes - is a rare autosomal dominant, multisystem
disease caused by a mutation in the protein tyrosine phosphatase, non-receptor type 11
gene (PTPN11). The disease is a complex of features, mostly involving the skin, skeletal
and cardiovascular systems, they may or may not be present in all patients. The nature of
how the mutation causes each of the condition's symptoms is not well known, however
research is ongoing.
Related to Noonan syndrome, LEOPARD syndrome is caused by a
different missense mutationof the same gene. Noonan syndrome is fairly common
(1:1000 to 1:2500 live births), andneurofibromatosis 1 (which was once thought to be
related to LEOPARD syndrome) is also common (1:3500), however no epidemiologic
data exists for LEOPARD syndrome.
Signs and symptoms:
The name of the condition is a mnemonic, originally coined in 1969,[5] as the
condition is characterized by some of the following seven conditions, the first letters of
which spell LEOPARD, along with the characteristic "freckling" of the skin, caused by
the lentigines that is reminiscent of the large cat.
Lentigines - Reddish-brown to dark brown macules (surface skin lesion) generally
occurring in a high number (10,000+) over a large portion of the skin, at times higher
than 80% coverage. These can even appear inside the mouth (buccal), or on the surface of
the eye (scleral). These have irregular borders and range in size from 1 mm in diameter
to café-au-lait spots, several centimetres in diameter. Also, some areas of vitiligolike hypopigmentation may be observed.
Electrocardiographic conduction abnormalities: Generally observed on
an electrocardiograph as a bundle branch block.
Ocular hypertelorism: Wideset eyes, which lead to a similar facial resemblance
between patients. Facial abnormalities are the second highest occurring symptom after
the lentigines. Abnormalities also include: broad nasal root, prognathism (protruding
lower jaw), or low-set, possibly rotated, ears.
Pulmonary stenosis: Narrowing of the pulmonary artery as it exits the heart. Other
cardiac abnormalities may be present, including aortic stenosis, or mitral valve prolapse.
Abnormal genitalia: (usually cryptorchidism (retention of testicles in body)
or monorchism (single testicle). In female patients, this presents as missing or single
ovaries, much harder by nature to detect. Ultrasound imaging is performed at regular
intervals, from the age of 1 year, to determine if ovaries are present.
Retarded growth: Slow, or stunted growth. Most newborns with this syndrome are
of normal birth weight and length, but will often slow within the first year.
Deafness: Sensorineural (nerve deafness).
The presence of all of these hallmarks is not needed for a diagnosis. A
clinical diagnosis is considered made when, with lentigines present there are 2 other
symptoms observed, such as ECG abnormalities and ocular hypertelorism, or without
lentigines, 3 of the above conditions are present, with a first-degree relative (i.e. parent,
child, sibling) with a clinical diagnosis.
Additional dermatologic abnormalities (axillary freckling,
localized hypopigmentation, interdigital webbing, hyperelastic skin)
Mild mental retardation is observed in about 30% of those affected with the
syndrome
Nystagmus (involuntary eye movements), seizures, or hyposmia (reduced ability
to smell) has been documented in a few patients
Due to the rarity of the syndrome itself, it is hard to determine whether certain
additional diseases are actually a threat of the syndrome. With a base population of
possibly less than one thousand individuals, one or two outlying cases can skew the
statistical population very quickly.
Diagnosis:
The presence of the disease can be confirmed with a genetic test. In a study of 10
infants with clinical indications of LEOPARD syndrome prior to their first birthday, 8
(80%) patients were confirmed to have the suspected mutation. An additional patient,
with the suspected mutation was subsequently found to have NF1, following evaluation
of the mother.
There are 5 identified allelic variants responsible for LEOPARD
syndrome. Y279C, T468M, A461T, G464A, and Q510P which seems to be a unique
familial mutation, in that all other variants are caused by transition errors, rather
than transversion.
Pathophysiology:
LEOPARD syndrome is inherited in anautosomal dominant fashion, although it
can also arise due to spontaneous mutation.
In the two predominant mutations of LEOPARD syndrome (Y279C and T468M)
the mutations cause a loss of catalytic activity of the SHP2 protein(the gene product of
the PTPN11 gene), which is a previously unrecognized behavior for this class of
mutations.[10] This interferes with growth factor and related signalling. While further
research confirms this mechanism,[11][12]additional research is needed to determine
how this relates to all of the observed effects of LEOPARD syndrome.
Prognosis:
In itself, LEOPARD syndrome is not a life threatening diagnosis, most people
diagnosed with the condition live normal lives. Obstructive cardiomyopathy and other
pathologic findings involving the cardiovascular system may be a cause of death in those
whose cardiac deformities are profound.
Holt-Oram Syndrome
Holt-Oram syndrome, also called heart-hand syndrome, is an inherited disorder
characterized by abnormalities of the upper limbs and heart. Holt and Oram first
described this condition in 1960 in a 4-generation family with atrial septal defects and
thumb abnormalities.1
Pathophysiology:
The syndrome is inherited as an autosomal dominant trait that is completely
penetrant. The disease is due to mutations in the transcription factor TBX5, which is
important in the development of both the heart and upper limbs. The pathophysiologic
sequelae are a direct result of malformations of the heart and upper limbs. No
contributory environmental factors are known.
Upper limb involvement
Although the clinical manifestations are variable, upper limb abnormalities are
always present. Abnormalities may be unilateral or bilateral and asymmetric and may
involve the radial, carpal, and thenar bones. Aplasia, hypoplasia, fusion, or anomalous
development of these bones produces a spectrum of phenotypes, including triphalangeal
or absent thumbs. Occasionally, upper limb malformation can be sufficiently severe to
produce phocomelia (a malformation in which the hands are attached close to the body);
this has been termed pseudothalidomide syndrome. The most prevalent findings in
persons with Holt-Oram syndrome are malformations or fusions of the carpal bones.
Carpal bone abnormalities are the only findings present in every affected individual,
although these anomalies may be evident only radiographically in some patients.
Cardiac involvement:
Approximately 75% of patients have some cardiac abnormality. In most patients,
the abnormality is either an atrial septal defect (ASD) or a ventricular septal
defect (VSD), which varies in number, size, and location. ASDs are usually of the
secundum variety, while VSDs tend to occur in the muscular trabeculated septum.
Cardiac anomalies also may include cardiac conduction defects such as progressive
atrioventricular block and atrial fibrillation.3,4 These anomalies are frequently present
even in the absence of septal defects.
Clinical Features:
Patients may have a family history of cardiac and/or limb malformation.
Patients may present in infancy with obvious limb malformations and/or signs of
cardiac failure secondary to ASD, VSD, or cardiac conduction disease.
Upper limb deformity
Always present but may be unilateral or bilateral
Left-sided abnormalities often more severe than right arm or hand abnormalities
Unequal arm lengths due to aplasia, hypoplasia, fusion, or anomalous
development of the radial, carpal, and thenar bones
Abnormal forearm pronation and supination
Triphalangeal or absent thumbs
Possible abnormal opposition of thumb
Possible sloping shoulders and restriction of shoulder joint movement
Phocomelia
Cardiac involvement
Bradycardia
Irregular pulse (ectopy)
Irregular pulse that occurs irregularly (atrial fibrillation)
Wide, fixed splitting of the second heart sound
Pulmonary systolic flow murmur
Holosystolic murmur (should raise consideration for a VSD)
Anomalies involving any of the following are indicators that a diagnosis of HoltOram syndrome can be excluded:
Ulnar bone
Lower limbs
Kidneys
Eyes
Auditory
Craniofacial
Vertebrae (may or may not occur in Holt-Oram syndrome)
Causes
Holt-Oram syndrome is a genetic disorder that is autosomal dominant and highly
penetrant.
Initial linkage studies demonstrate that the gene defect resides on the long arm of
chromosome 12.5,6
Molecular genetic studies reveal that the disease is caused by mutations that
inactivate the transcription factor TBX5.7
Sporadic disease may represent a de novo germline mutation in TBX5.
Recognizing that individuals who present with sporadic disease may transmit the
disease to offspring is important.
The identification of the role of TBX5 in Holt-Oram syndrome suggests an
important but as yet undefined role for TBX5 in human cardiac septation, isomerization,
and upper limb development.
Management:
Medical Care
Evaluation can usually be performed in an outpatient setting, but inpatient studies
and surgical treatment may be necessary.
Patients with advanced heart block may require a permanent pacemaker.
Surgical therapy can be used to correct cardiac defects or to possibly improve
limb function.
Surgical Care
Most cardiac lesions such as ASD and VSD are amenable to complete surgical
correction if pulmonary hypertension or ventricular failure has not developed. Several
percutaneous transcatheter devices that can be placed to occlude the septum are in US
Food and Drug Administration–approved clinical trials and may be nonsurgical options
in the future.
Septal defects without hemodynamically significant shunts do not require
correction.
Children with severe limb anomalies can be referred to orthopedic surgeons for
consideration of procedures such as pollicization of the fifth digit (to improve upper limb
function).
Children with severe limb shortening may benefit from prostheses.
Kartagener Syndrome
Kartagener syndrome (KS) is inherited via an autosomal recessive pattern.
Symptoms result from defective cilia motility.
Camner and coworkers2 first suggested ciliary dyskinesia as the cause of Kartagener
syndrome in 1975. They described 2 patients with Kartagener syndrome who had
immotile cilia and immotile spermatozoa. These patients had poor mucociliary clearance
because the cilia that lined their upper airways were not functioning.
Later, Afzelius3 discovered that bronchial mucosal biopsy specimens from
patients with similar respiratory complaints showed cilia that appeared abnormal, were
poorly mobile, and were missing dynein arms. In 1977, Eliasson and coworkers4 used the
descriptive phrase immotile cilia syndrome to characterize male patients with sterility and
chronic respiratory infections.
In 1981, Rossman and coworkers5 coined the term primary ciliary dyskinesia
(PCD) because some patients with Kartagener syndrome had cilia that were not immobile
but exhibited an uncoordinated and inefficient movement pattern. Current nomenclature
classifies all congenital ciliary disorders as primary ciliary dyskinesias in order to
differentiate them from acquired types. Kartagener syndrome is part of the larger group
of disorders referred to as primary ciliary dyskinesias. Approximately one half of patients
with primary ciliary dyskinesia have situs inversus and, thus, are classified as having
Kartagener syndrome. Afzelius proposed that normal ciliary beating is necessary for
visceral rotation during embryonic development. In patients with primary ciliary
dyskinesia, organ rotation occurs as a random event; therefore, half the patients have situs
inversus and the other half have normal situs.
Ciliated epithelium covers most areas of the upper respiratory tract, including the
nasal mucosa, paranasal sinuses, middle ear, eustachian tube, and pharynx. The lower
respiratory tract contains ciliated epithelium from the trachea to the respiratory
bronchioles. Each ciliated cell gives rise to approximately 200 cilia that vary in length
from 5-6 μm and decrease in size as the airway becomes smaller.
The typical ciliary axoneme consists of 2 central microtubules surrounded by 9
microtubular doublets. Each doublet has an A subunit and a B subunit attached as a
semicircle. A central sheath envelops the 2 central microtubules, which attach to the outer
doublets by radial spokes.
The outer doublets are interconnected by nexin links, and each A subunit is
attached to 2 dynein arms that contain adenosine triphosphatase; one inner arm and one
outer arm. The primary function of the central sheath, radial spokes, and nexin links is to
maintain the structural integrity of the cilium, whereas the dynein arms are responsible
for ciliary motion.
The cilium is anchored at its base by cytoplasmic microtubules and a basal body
comprised of a basal foot and rootlet. The orientation of the basal foot indicates the
direction of the effective cilial stroke. Just above the base, the cilium is composed of
microtubular triplets (previously doublets) without associated structures, but at the tip,
only the B subunits remain.
Cilia propel overlying mucus via a 2-part ciliary beat cycle. First, the power
stroke occurs when a fully extended cilium moves perpendicular to the cell surface in an
arclike manner. Then, the recovery stroke follows, in which the entire cilium bends and
returns to its starting point near the cell surface. Once a cilium starts to move, the
complete beat cycle is obligatory.
The cycle is mediated by dynein arms from the A subunit that attach to the B
subunit of the adjacent microtubule. Adenosine triphosphate is hydrolyzed by the dynein
arms and the 9 microtubule doublets as they slide against each other.
Patients with primary ciliary dyskinesia exhibit a wide range of defects in ciliary
ultrastructure and motility, which ultimately impairs ciliary beating and mucociliary
clearance. The most common defect, first described by Afzelius, is a reduction in the
number of dynein arms, which decreases the ciliary beat frequency.
Sturgess et al6 described how the radial spoke, which serves to translate outer
microtubular sliding into cilial bending, was absent in some patients with primary ciliary
dyskinesia. Cilia in other patients lacked central tubules; however, instead of the central
tubules, an outer microtubular doublet transposed to the cell of the axoneme was present
that displayed an abnormal 8+1 doublet-to-tubule pattern. Both the radial spoke and the
transposed doublet defects impaired mucociliary clearance.
Other ciliary defects include an abnormal basal cell apparatus with giant roots and
double feet, cilia lacking all internal microtubular structures, and even cilia twice the
normal length that beat in an uncoordinated undulating fashion. Pedersen7 compared the
type of ultrastructural defect to ciliary motility and found that dynein defects caused
hypomotility and microtubular defects (ie, caused asynchrony). He also found that
normal ciliary ultrastructure occasionally was associated with hypermotility or inefficient
ciliary trembling.
Some patients with clinical features of primary ciliary dyskinesia have a ciliary
ultrastructure that appears normal, but their arrangement and beat direction is disoriented,
which causes inefficient mucociliary transport. These findings illustrate the importance of
analyzing ciliary motility and ultrastructure when considering a diagnosis of primary
ciliary dyskinesia.
linical
History:
Patients present with chronic upper and lower respiratory tract disease resulting
from ineffective mucociliary clearance. A typical presentation is that of rhinorrhea and/or
mucopurulent discharge since birth. Immotile spermatozoa result in male sterility.
Clinical Features:
Kartagener syndrome is characterized by the clinical triad of chronic sinusitis,
bronchiectasis, and situs inversus.
Upper airway
Patients may exhibit chronic, thick, mucoid rhinorrhea from early in childhood.
Examination usually reveals pale and swollen nasal mucosa, mucopurulent secretions,
and an impaired sense of smell. Nasal polyps are recognized in 30% of affected
individuals.8
The recurrent chronic sinusitis typically produces sinus pressure headaches in the
maxillary and periorbital region. Symptoms usually improve with antibiotic therapy but
have a propensity for rapid recurrence.8
Recurrent otitis media is a common manifestation of primary ciliary dyskinesia.
Examination may reveal a retracted tympanic membrane with poor or absent mobility and
a middle-ear effusion. Other associated otologic disorders may include tympanosclerosis,
cholesteatoma, and keratosis obturans.8
Lower respiratory tract
Chronic bronchitis and recurrent pneumonia are common conditions in patients with
primary ciliary dyskinesia. Thus, upon physical examination of the patient's chest,
increased tactile fremitus, rhonchi, crackles, and, occasionally, wheezes may be present.
Obstructive lung disease may be another component of Kartagener syndrome
symptomatology. It probably results from elevated levels of local inflammatory
mediators in a chronically irritated airway. Therefore, wheezing may occur. The lung
examination may be normal during intercurrent periods when the airway is not actively
inflamed.
Other features :
Cardiovascular examination of a patient with KS demonstrates a point of maximal
impulse, and the heart sounds are heard best on the right side of the chest.
Extremities may exhibit digital clubbing.
Kussmaul's Sign
In healthy individuals, breathing in (inspiring) increases venous return to the right
heart. Any evident neck vein distension, therefore, should diminish during inspiration.
In patients with conditions that impair venous return to the right heart inspiration may be
associated with an absence of jugular vein collapse or a paradoxical rise in the jugular
column (video). This is called Kussmaul's sign.
Cardiac conditions that may be associated with a positive Kussmaul's sign include
right atrial myxoma, tricuspid stenosis, constrictive pericarditis, pericardial effusion,
restrictive myocardopathy, and severe pulmonary hypertension. Overall, the commonest
cause is severe right-sided congestive heart failure. Superior vena cava obstruction can
also result in a positive Kussmaul's sign.
Kussmaul's breathing is seen in diabetic ketoacidosis (acetone breath).
While Kussmaul's sign is an elevated Jugular Venous Pressure seen during inspiration in
constrictive pericarditis or improper filling of the heart. (It's not seen in cardiac
temponade though).
Also seen in constrictive cardiomyopathy, severe right sided heart failure, and tricuspid
valve stenosis all of these leads to the same pathophysiology of improper heart filling
during inspiration.
Lighthouse sign
Lighthouse sign (blanching & flushing of forehead) Peripheral physical signs of
aortic insufficiency.
Landolfi's sign
In aortic insufficiency, systolic contraction and diastolic dilation of the pupil is
Landolfi's sign (alternating constriction & dilatation of pupil)
Becker's sign
Becker's sign, or Becker's phenomenon, is the presence of visible pulsation
of retinal arteries found in patients with aortic insufficiency orGraves' disease.
De Musset's sign
De Musset's sign is a human health condition that results in a rhythmic nodding or
bobbing of the head in synchrony with the beating of theheart, in general as a result
of aortic insufficiency caused by aortic regurgitation due to aortic valve deficiency.
Musset's sign rhythmical jerking of the head in aortic aneurysm and aortic
insufficiency
Müller's sign
Müller's sign is the pulsation or bobbing of the uvula that occurs during systole. It
can be seen in patients with severe aortic insufficiency. Müller's sign is caused by an
increased stroke volume. In aortic insufficiency, rhythmical pulsatory movements of
the uvula, synchronous with the heart'saction; accompanied by swelling and redness of
the velum palati and tonsils.
Quincke's sign
Quincke's sign (pulsation of the capillary bed in the nail)
Quincke's pulse alternate blanching and flushing of the nail bed due to pulsation
of subpapillary arteriolar and venous plexuses; seen in aortic insufficiency and other
conditions and occasionally in normal persons.
The capillary pulse as appreciated in the finger and toenails during aortic
regurgitation; ebb and flow is seen.
Quincke's sign.
Quincke's pulse alternate blanching and flushing of the nail bed due to pulsation
of subpapillary arteriolar and venous plexuses; seen in aortic insufficiency and other
conditions and occasionally in normal persons.
Corrigan's sign
Corrigan's sign is the rapid rise and fall of pulse of the carotid artery on inspection
which is consistent with the wide pulse pressure of aortic regurgitation.
Corrigan's pulse jerky pulse with full expansion and sudden collapse.
A full hard pulse followed by a sudden collapse easily palpated and occurring
in aortic regurgitation.
Traube's sign
A double sound or murmur heard in auscultation over arteries (particularly
the femoral arteries) insignificant aortic regurgitation.
Traube's sign (a 'pistol shot' systolic sound heard over the femoral artery )
Duroziez's sign
Duroziez's sign is a sign of Aortic insufficiency.[1] It consists of an audible
diastolic murmur which can be heard over the femoral artery when it is compressed.
Duroziez's sign (systolic and diastolic murmurs heard over the femoral artery
when it is gradually compressed with the stethescope)
Hill's sign
An indication of aortic insufficiency in which systolic blood pressure is higher in
the legs than in the arms.
Hill's sign - a ≥ 20 mmHg difference in popliteal and brachial systolic cuff
pressures, seen in chronic severe AI. Considered to be an artefact of sphygmomanometric
lower limb pressure measurement