Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
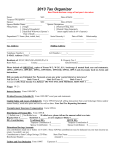
TAX YEAR 2016 CLIENT TAX ORGANIZER INSTRUCTIONS Dear Tax Client: Do not send your tax information until you have completed this organizer and have all of your tax info. to send. We will not accept or store partial information. Thank you for allowing us to prepare your tax returns for tax year 2016. Please read and follow these instructions carefully. Failure to do this will delay the completion of your tax return and result in an inaccurate result. If you are sending your child’s tax info., they must complete & sign their own organizer. WARNING: No signed organizer, No tax preparation!!! 1. Fill in only the areas that apply to you. 2. Fill in all personal information even if you are a previous client. 3. Include all tax documents that you received for the tax year (W2s, 1099 Misc., 1099 Int., 1099 Div., etc.) 4. For PA Clients Only - Include your local tax return forms that you receive in the mail. We have all federal and state forms in our office. 5. If you moved during the year we need your moving date as well as your old and new addresses. 6. Do not send all your receipts for expenses. Send us a list of your expenses and group them in categories. We need to know that you have receipts for your expenses and may ask to verify them; but we do not keep them on file in our offices. 7. If you have a ministerial housing allowance did you spend it all? If not, how much did you have left over above your housing costs? 8. For auto expenses be sure to include a description of the auto, business miles, commuting miles, personal miles, and purchase date of each vehicle for which you are claiming mileage. Please separate your mileage for each vehicle. Do not send us just one mileage figure for all vehicles! 9. If you have honoraria or other self employed income, list it separately. List your expenses incurred due to this self employment income separately from other employee expenses. 10. List your federal, state, and local estimated tax payments that you made for the tax year along with the dates that you made the payments. 11. Please sign the organizer (both husband & wife) at the signature lines to certify that the information that you are providing us is accurate and that you have receipts or other documentary evidence to support your income and expense information. 12. You must complete the Healthcare Worksheet page as completely as possible or your taxes will be delayed. We will not prepare your taxes without the info. required on that page. CERRAN ENTERPRISES CLIENT TAX ORGANIZER Tax Year 2016 Please complete this Questionnaire before your appointment and bring the following: All statements Last year’s tax return (new clients only) All statements (W-2s, 1099s, etc.) 1. Personal Information Name (First, Initial, Last) Soc. Sec. No. Date of Birth Occupation Work Phone Zip Home Phone Taxpayer Spouse Street Address City County State Boro or Township School District Taxpayer E-mail Address Spouse E-mail Address Blind Disabled Taxpayer ___ Yes ___ No ___ Yes ___ No Pres. Campaign Fund ___ Yes ___ No Spouse ___ Yes ___ No ___ Yes ___ No Marital Status ___ Married ___ Single ___ Yes ___ No ___ Widow(er) Will file jointly ___ Yes ___ No Date of divorce _________________ Date of Spouse’s Death __________ 2. Dependents (Children & Others) Name ( First, Initial, Last) Relationship Date of Birth Social Security Number Months Lived with You Disabled Full Time Student Dependent’s Gross Income 1. Did you receive rent from real estate or other property? __________________________________________________________ 2. Did you refinance your main home or other property? ____________________________________________________________ 3. Did you receive any correspondence from the IRS or State Department of Taxation? __________________________________ 4. Did you pay interest on a student loan for yourself, your spouse, or your dependent during the year? _____________________ 5. Did you pay expenses for yourself, your spouse, or your dependent to attend classes beyond high school? _________________ 6. Beginning Jan. 1, 2011 we must efile all tax returns unless you opt out. Do you wish to opt out of efiling? ___ Yes ___ No If yes, you must complete and ATTACH OPT OUT form. 7. Would you like your refund directly deposited into your bank? ____________________________________________________ Account Type: Your Account Number: Checking ____________ Bank Routing Number: Savings _____________ 3. Wage, Salary Income 7. Partnership, Trust, Estate Income ATTACH W-2s: Employer Taxpayer Spouse ____________________________ ______ ______ List payers of partnership, limited partnership, S-corporation, trust, or estate income – ATTACH K-1 __________________________________________________ ____________________________ ______ ______ __________________________________________________ ____________________________ ______ ______ __________________________________________________ ____________________________ ______ ______ ________________________________________________________ ____________________________ ______ ______ ____________________________ ______ ______ 8. Property Sold ATTACH 1099-S and closing statements 4. Interest Income ATTACH 1099-INT & broker statements Payer’s Name Taxpayer Spouse ____________________________ ______ ______ ____________________________ ______ ______ ____________________________ ______ ______ ____________________________ ______ ______ Tax Exempt ___________________________ ______ ______ ___________________________ ______ ______ ___________________________ ______ ______ Property Personal Residence* Vacation Home Date Acquired *Provide information on improvements, prior to sales of home, and cost of a new residence 9. I.R.A. (Individual Retirement Acct.) Contributions for tax year income – not listed on W2 Amount X for Date X for Roth IRA Taxpayer Spouse Amounts withdrawn – ATTACH 1099-R & 5498 Plan Trustee Reason for Withdrawal 5. Dividend Income From Mutual Funds & Stocks – ATTACH 1099-DIV Payer’s Name Taxpayer Spouse ___________________________ _______ ______ _______ ______ ___________________________ _______ ______ ___________________________ _______ ______ Reinvested? ___ Yes ___ ___ Yes ___ ___ Yes ___ ___ Yes ___ ____ Yes ____ No Did you receive: Taxpayer Spouse Social Security benefits __ Yes __ No __ Yes __ No Rail Road Retirement __ Yes __ No __ Yes __ No ATTACH 1099-R, SSA 1099, RRB 1099 6. Investment Sold Stocks, Bonds, Mutual Funds, Gold, Silver, Partnership interest – ATTACH 1099-B & confirmation slips Investment Date Acquired/Sold Cost . No No No No 10. Pension, Annuity Income Did you receive pension funds? ___________________________ Cost & Imp. Sale Price 11. Other Income List All Other Income (including non-Taxable) Alimony Received Child Support Scholarship (Grants) Unemployment Compensation (repaid) Prizes, Bonuses, Awards Gambling, Lottery (expenses _______) Unreported Tips and Gratuities Director / Executor’s Fee Commissions Jury Duty Pay Worker’s Compensation Disability Income Veteran’s Pension Payments from Prior Installment Sale State Income Tax Refund Clergy Honoraria Other __________ __________ __________ __________ __________ __________ __________ __________ __________ __________ __________ __________ __________ __________ __________ __________ __________ 16. Moving Information Did you move during 2016? Yes_____ No_____ Move Date ________________ If yes, previous address ______________________________ __________________________________________________ Previous County & School District _____________________ __________________________________________________ 12. Medical/Dental Expenses Long-term Care Premium Medical Insurance Premiums (paid by you) Prescription Medications Insulin Eyeglasses, Contact Lenses Hearing Aids, Batteries Braces Medical Equipment, Supplies Nursing Care Services Medical Therapy Hospital and Nursing Homes Doctor, Dentist, and other Healthcare Professionals Lodging Mileages (no. of miles) __________ __________ __________ __________ __________ __________ __________ __________ __________ __________ __________ Current address _____________________________________ __________________________________________________ __________ __________ __________ 18. Employment-Related Expenses That You Paid (Not self-employed) Current County & School District ______________________ __________________________________________________ 17. Job-Related Moving Expenses Date of move _________________ Move Household Goods Travel to New Home (no. of miles) Lodging During Move __________ __________ __________ (List and identify Taxpayer & Spouse expenses separately) 13. Taxes Paid Real Property Tax (attach bills) Personal Property Tax Other Taxes __________ __________ __________ 14. Charitable Contributions Church ____________________________ 15. Interest Expense Mortgage interest paid (ATTACH 1098) __________ Interest paid to individual for your home (include amortization schedule) __________ Paid to: Name ___________________________________ Address _________________________________ Social Security No . ________________________ Investment Interest __________ ___________ Other Charities (List name and give amounts) _______________________________ ___________ _______________________________ ___________ _______________________________ ___________ Non –Cash ________________________ ___________ Volunteer (no. of miles) ______________ ___________ *Provide detail if over $5000.00 is paid to any one organization. Dues – Union, Professional Books, Subscriptions, Supplies Licenses Tools, Equipment, Safety Equipment Uniforms (including cleaning) Sales Expense, Gifts Tuition, Books (work related) Entertainment __________ __________ __________ __________ __________ __________ __________ __________ Office in home: In a) Total Home ________________ Square b) Office ________________ Feet c) Storage ________________ Rent Insurance Utilities Maintenance ___________ ___________ ___________ ___________ 19. Child & Other Dependent Care Name of Care Provider Address Soc Sec No. or Employer ID Amount Paid Also complete this section if you receive dependent care benefits from your employer. 20. Business Mileage / Actual Cost Method Do you have written records? 23. Auto Mileage Record / Standard Deduction Method ___ Yes ___ No Did you sell or trade in a car used for Business? ___ Yes ___ No Make/Model Year Vehicle __________________________ Date Purchased ___________________________________ Total Miles (personal & business) __________ Business Miles (not to and from work) __________ From First to Second Job __________ Education (one way, work to school) __________ Job Seeking __________ Other Business __________ Round Trip commuting distance __________ Gas, Oil, Lubrication __________ Batteries, Tires, etc. __________ Repairs __________ Wash __________ Insurance __________ Interest __________ Lease Payments __________ Garage Rent __________ VEHICLE 1 Description: VEHICLE 2 Description: Date placed in service: Date placed in service: Total mileage Business mileage Commuting mileage Personal mileage 21. Investment-Related Expenses Tax Preparation Fee Safe Deposit Box Rental Mutual Fund Fee Investment Counselor Other __________ __________ __________ __________ __________ 24. Estimated Tax Payments /not W2 amounts Date Paid Federal State Local 22. Business Travel If you are not reimbursed for exact amount, give total expenses. Airfare, Train, etc. Lodging Meals (no. of days ___________) Taxi, Car Rental Other Reimbursement Received __________ __________ __________ __________ __________ __________ 25. Other Deductions Alimony Paid to __________________________________ Social Security No. _________________ Student Loan Interest Paid $___________ $_____________ 26. Education Expenses Student’s Name Type of Expense Amount __________________ ______________ ______________ _______________ ____________ ____________ _______________ ____________ ____________ SPECIAL NOTE: 27. For Ministers Only 1. Designated Housing Allowance $___________________ Amount of Housing Allowance Actually Spent $____________________________________ 2. If you lived in a Parsonage - Fair Rental Value (FRV) of the Church Parsonage $____________________ 3. Unreimbursed Professional Expenses (DO NOT SEND RECEIPTS / just give category totals) Professional Dues Travel Books Subscriptions Gifts ($25/personal/year limit) Supplies Religious Materials Entertainment Education Other ____________ ____________ ____________ ____________ ____________ ____________ ____________ ____________ ____________ ____________ *************************** HEATHCARE INSURANCE COVERAGE Enter the name, SSN/DOB and health insurance status for each person claimed on your return in the table below regarding the new health insurance reporting requirements beginning in 2014. (If not all 12 months, indicate which months each Name of covered individual(s) SSN/DOB Covered All Exchange Exemption person was covered by MEC*) 12 months Policy Received Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Use this worksheet to list the names of individuals listed on the income tax return and their health care insurance coverage status. It will help your tax preparer determine who has health insurance coverage, who may have an exemption, and who may be subject to the individual shared responsibility payment. Beginning in 2014, most individuals are required to have: Minimum Essential Coverage (MEC*), or An Exemption from the responsibility to have minimum essential coverage, or Make a Shared Reponsibility Payment. Minumum Essential Coverage includes employer-sponsored coverage, health insurance purchased through the Health Insurance marketplace (Exchange), Medicare, medicaid, certain VA coverage, Tricare, etc. If you purchased a health insurance policy from an exchange (or marketplace, check the Exchange Policy box above. You will receive Form 1095-A from the exchange that issued your policy. Please provide us with this form. Also if you received a 1095 B or C form, please include it with this organizer. We cannot begin to process your taxes without this necessary Healthcare information. *************************** To the best of my knowledge the enclosed information is correct and includes all income, deductions, and other information necessary for the preparation of this year’s income tax returns for which I have adequate records. Signature____________________________________________________________ Date _________________ Signature____________________________________________________________ Date _________________ Please Note: Your tax return will not be processed without the appropriate signatures On the lines above. Both persons whose names appear on a joint tax return must sign On the appropriate line above. E-FILING IS NOW MANDATORY FOR FIRMS PREPARING 10 OR MORE TAX RETURNS!!! If you wish to opt out of efiling, you must complete an opt out form and send it with your completed organizer. This form is available on our web site. ADDITIONAL NOTES AND INFO Please mail to: Cerran Enterprises 65 Willow Mill Park Rd Mechanicsburg, PA 17050 Please include your current email address on page 1