Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
© Hepatitis C Online
PDF created May 2, 2017, 9:53 pm
Treatment of Hepatitis C in Patients with HIV
Coinfection
This is a PDF version of the following document:
Module 6:
Treatment of Special Populations and Special Situations
Lesson 2:
Treatment of Hepatitis C in Patients with HIV Coinfection
You can always find the most up to date version of this document at
http://www.hepatitisc.uw.edu/go/special-populations-situations/treatment-hiv-coinfection/coreconcept/all.
Background of HCV-HIV Coinfection
Impact of HIV Coinfection in Persons with Chronic Hepatitis C Infection: In the United
States, approximately 5 to 10 percent of patients with chronic hepatitis C (HCV) infection are
coinfected with HIV. Coinfection with HIV accelerates the progression of hepatic fibrosis and results
in a more aggressive course of liver disease (Figure 1). Cirrhosis has been observed to occur 12 to
16 years earlier in those coinfected with HCV and HIV compared with those who have HCV
monoinfection. For HIV-infected patients with HCV coinfection, liver-related morbidity and mortality
is a prominent non-AIDS-defining complication—up to 90% of liver-related deaths in HIV-infected
patients are attributable to HCV. Unfortunately, patients coinfected with HCV and HIV have
decreased access to liver transplantation compared with HCV monoinfected patients. For all of these
reasons, treatment of HCV in this patient population should have a high priority. Historically,
treatment of HCV in patients coinfected with HIV had limited uptake, largely due to a low response
rate with interferon-based therapy, a high rate of adverse effects, concerns for interactions with
antiretroviral medications, and high prevalence of comorbidities, such as psychiatric conditions and
chemical dependency. The recent availability of highly effective all-oral HCV regimens has generated
major enthusiasm and interest for the treatment of HCV in persons coinfected with HIV.
Historic Approach to Treatment: For patients coinfected with HCV and HIV, initial trials with
interferon monotherapy or dual therapy with standard interferon plus ribavirin were associated with
very low SVR rates and significant toxicity. Response rates were higher with peginterferon and
ribavirin in coinfected patients, but still suboptimal, as summarized in a table format (Figure 2) and a
graph illustration (Figure 3). The peginterferon and ribavirin combination regimen had particularly
low SVR rates among those with genotype 1 HCV (typically less than 30%). Further, the SVR rates
with peginterferon and ribavirin was 15 to 25% lower in coinfected patients than in HCV
monoinfected patients. In 2011, the addition of a first-generation HCV protease inhibitor (telaprevir
or boceprevir) to peginterferon and ribavirin improved SVR rates with GT1 to approximately 60% and
narrowed the gap in treatment response between coinfected and monoinfected patients to
approximately 15%. This triple therapy regimen, however, proved to be quite complex and
challenging due to interactions with antiretroviral medications, greater pill burden, food
requirements, and additional adverse effects. With the advent of all-oral regimens that include new
direct acting antiviral agents (DAAs) that are safe, highly effective, and have fewer drug interactions,
the older regimens of peginterferon and ribavirin or peginterferon and ribavirin plus a firstgeneration protease inhibitor are no longer recommended for treatment of HCV in coinfected
patients.
1 / 20
Key Studies for Treatment of HCV with HIV Coinfection
Changing Landscape of Treatment in Coinfected Patients: The introduction of direct-acting
antiviral agents (DAAs), and in particular, interferon-free combination therapy, has changed the
landscape of therapy for patients coinfected with HCV and HIV. Several studies using DAA-based
therapy have demonstrated comparable rates of sustained virologic response in coinfected and
monoinfected patients (Figure 4), providing convincing evidence that coinfected patients may no
longer require the designation of a special or “treatment refractory” population. It should be noted
that these trial participants included primarily individuals without cirrhosis and those with high CD4
cell counts, usually well above the threshold of 200 cells/mm3. Ultimately, clinical efficacy in more
heterogeneous cohorts of coinfected patients will need to be demonstrated. The following provides a
summary of key studies (in alphabetical order) that have involved treatment of hepatitis C infection
in patients who have HIV coinfection. Click on the study name to see more details and summary
PowerPoint slides.
ALLY-2: In the phase 3, randomized, multi-center ALLY-2 trial, investigators enrolled 203 HIVHCV coinfected patients to receive HCV treatment with daclatasvir plus sofosbuvir.
Treatment-naive patients were randomized to receive either an 8-week or 12-week treatment
course, whereas all treatment-experienced patients received a 12-week course. Patients with
HCV genotype 1, 2, 3, or 4 were eligible. The HIV entry criteria required a CD4 count greater
than 350 cells/mm3 if the patient was not taking antiretroviral therapy or at least 100
cells/mm3 if on antiretroviral therapy and an HIV RNA less than 50 copies/ml. The SVR 12
rates were excellent with the 12-week regimens (96% in treatment-naive and 98% in
treatment-experienced patients) but only 76% in the 8-week regimen for treatment-naive
patients.
C212: This open-label phase 3 trial evaluated the effectiveness of simeprevir with
peginterferon and ribavirin (weight-based dosing) in both treatment-naïve (n=53) and
treatment-experienced (n=63) HIV/HCV coinfected patients with chronic HCV genotype 1.
The overall SVR12 rate was 74% to 79% among treatment-naïve patients and 57% among
prior null responders.
C-EDGE Coinfection: In this prospective single-arm, open-label clinical trial, investigators
enrolled 218 patients with chronic hepatitis C genotype 1, 4, or 6 and HIV coinfection for
treatment with a 12-week course of elbasvir-grazoprevir once daily for 12 weeks. Among
those enrolled, 86% had genotype 1a or 1b infection and 35 (16%) had compensated
cirrhosis. The overall SVR12 rate was 96% by primary analysis, with the breakdown by
genotype showing 96.5% for genotype 1a, 95.5% for genotype 1b, and 96.4% for genotype 4.
All cirrhotic patients achieved an SVR12.
NIAID ERADICATE: This phase 2 trial investigated the open-label use of ledipasvir-sofosbuvir
for 12 weeks in 50 treatment-naïve patients with genotype 1 chronic HCV and HIV
coinfection. Among the 50 patients enrolled, 13 were not on antiretroviral therapy and 37
were receiving antiretroviral therapy (medications allowed included tenofovir-emtricitabine,
efavirenz, and rilpivirine). Overall, 49 (98%) of patients in the study achieved an SVR12.
ION-4: In this phase 3, open-label, multicenter study, investigators enrolled 335 patients with
hepatitis C genotype 1 or 4 who were coinfected with HIV to receive a 12-week course of
ledipasvir-sofosbuvir. Enrollment included HCV treatment-naive and experienced patients
and those without cirrhosis and those with compensated cirrhosis. The HIV enrollment criteria
consisted of HIV RNA less than 50 copies/ml, CD4 count greater than 100 cells/mm3;
antiretroviral regimens could include tenofovir-emtricitabine plus either efavirenz, rilpivirine,
or raltegravir. Overall, 321 (96%) of 335 treated patients achieved an SVR12. The results
were similar regardless of prior treatment status or presence of cirrhosis.
PHOTON-1: This open label, nonrandomized, uncontrolled, phase 3 trial evaluated 223
patients with chronic hepatitis C genotypes 1, 2, or 3 and HIV coinfection. This trial examined
the efficacy of the all-oral regimen of sofosbuvir plus ribavirin (weight-based) in treatmentnaive and treatment-experienced patients. Patients in the trial were required to be on stable
antiretroviral therapy with an undetectable HIV RNA level and CD4 count greater than 200
2 / 20
cells/mm3, or if untreated, they had CD4 count greater than 500 cells/mm3. The trial included
treatment-naive patients with genotype 1, 2, or 3 and treatment-experienced patients with
genotype 2 or 3. A 24-week treatment course was given to all patients with HCV genotype 1
and to treatment-experienced patients with HCV genotype 2 or 3; treatment-naive patients
with HCV genotype 2 or 3 received a 12-week treatment course. Patients with cirrhosis were
included in the trial, but could not comprise more than 20% of the total number of subjects
enrolled. For treatment-naive patients, the SVR12 rates were 76% with genotype 1, 88% with
genotype 2, and 67% with genotype 3. Treatment-experienced patients with genotype 2 had
a 92% SVR12 rate and those with genotype 3 had a 94% SVR12 rate.
PHOTON-2: In this open-label, phase 3 trial, 274 HIV-infected patients coinfected with HCV
genotype 1,2,3, or 4 received treatment with the all-oral regimen of sofosbuvir plus weightbased ribavirin. The study enrolled treatment-naive patients with genotypes 1, 2, 3, or 4 and
treatment-experienced with genotype 2 or 3. A 24-week treatment course was given to all
patients with HCV genotype 1, 3, or 4 and treatment-experienced patients with genotype 2,
whereas treatment-naïve with HCV genotype 2 received 12 weeks. Among those enrolled,
81% of the patients were HCV treatment naïve and 20% had cirrhosis. The mean CD4 count
was 588 cells/mm3 and 97% were on antiretroviral therapy (tenofovir-emtricitabine plus one
of the following: efavirenz, atazanavir plus ritonavir, darunavir plus ritonavir, rilpivirine, or
raltegravir). The SVR 12 rates were high with all HCV genotypes: GT1 (85%), GT2 (88%), GT3
(89%), and GT4 (84%). In addition, the treatment responses were similar in the treatmentnaïve and treatment-experienced patients.
Sofosbuvir for Genotype 1-4 in HIV Coinfection: In this single-arm, single-site, open-label trial,
23 HCV/HIV coinfected treatment-naïve patients with genotype 1-4 received the 12-week
triple therapy of peginterferon alfa-2a, ribavirin (weight-based), and sofosbuvir. Mean CD4
count was 562 cells/mm3 and all were on antiretroviral therapy (tenofovir-emtricitabine plus
one of the following: efavirenz, atazanavir plus ritonavir, darunavir plus ritonavir, rilpivirine,
or raltegravir). The overall SVR12 rate was 91%; of the 19 patients with genotype 1, 89%
achieved an SVR12.
TURQUOISE-I This open-label study randomized treatment-naïve and experienced patients
with chronic HCV genotype 1 patients with HIV coinfection to receive a 12- or 24-week course
of ombitasvir-paritaprevir-ritonavir and dasabuvir plus ribavirin. Patients were required to
have a CD4 count of at least 200 cells/mm3 (or CD4% greater than 13) and an HIV RNA level
less than 40 copies while receiving an atazanavir- or raltegravir-based regimen. Enrollment
included patients with compensated cirrhosis (Child-Pugh class A) and patients with prior
treatment with peginterferon plus ribavirin. The SVR12 rates were 29 (93.5%) of 31 in the
12-week group and 29 (90.6%) of 32 in the 24-week group.
3 / 20
Recommended HCV Treatment in Patients with HIV Coinfection
Timing of Antiretroviral Therapy in Context of HCV Therapy: The 2015 HIV Department of
Health and Human Services (DHHS) Guidelines on the use of antiretroviral therapy emphasizes the
following key points regarding antiretroviral therapy for persons coinfected with HIV and HCV:
Antiretroviral therapy should be considered for most patients with HIV and HCV coinfection,
regardless of their CD4 cell count. This recommendation is supported by observational
studies that suggest antiretroviral therapy may slow liver disease progression and reduce the
risk of liver-related morbidity.
In antiretroviral-naive patients with a CD4 count greater than 500 cells/mm3, antiretroviral
therapy could be deferred until after treatment of HCV.
For those patients whose CD4 counts are less than 200 cells/mm3 it may be advisable to first
initiate antiretroviral therapy and defer HCV therapy until the patient is stable on
antiretroviral therapy.
Factors to Consider Prior to Choosing HCV Treatment Regimen: In persons coinfected with
HIV, the major factors in selecting a regimen to treat HCV include HCV genotype, prior treatment
experience, presence of cirrhosis, and potential drug interactions with the HIV antiretroviral
medications. Of note, the preponderance of clinical trial data on the efficacy of HCV therapy derive
from patients on antiretroviral therapy with suppressed HIV RNA levels and CD4 counts greater than
200 cells/mm3.
AASLD/IDSA Guidance: The guidance from the American Association for the Study of Liver
Diseases (AASLD) and the Infectious Diseases Society of America addresses the treatment of
patients with HIV/HCV coinfection in detail (see Unique Patient Populations: Patients with HIV/HCV
Coinfection). For a summary of the recommendations for the treatment of HCV in persons coinfected
with HIV, including recommendations related to HCV medication interactions with antiretroviral
medications, see the Summary Box. The AASLD/IDSA guidance recommends using the same
approach for HCV treatment in persons coinfected with HIV as those with HCV monoinfection, but
noting that important drug-drug interactions between HCV medications and HIV antiretroviral
medications need to be recognized and managed. In the HCV guidance, older regimens, such as
peginterferon plus ribavirin or peginterferon plus ribavirin plus either boceprevir, telaprevir, or
simeprevir are not recommended for use in any circumstance, due to suboptimal SVR rates, long
duration of therapy, and poor tolerance.
4 / 20
Drug-Drug Interactions with HIV-HCV Coinfection Treatment
Most persons coinfected with HCV and HIV are taking multi-drug antiretroviral therapy, which may
pose a problem with drug-drug interactions when initiating therapy with HCV medications. See the
summary table (Figure 5) from the drug interactions section in the HHS Guidelines for the Use of
Antiretroviral Agents in HIV-1 Infected Adults and Adolescents. Note that daclatasvir was not FDA
approved for use in the United States at the time these tables were last updated. The following
provides key points related to drug-drug interaction for each HCV medication listed below.
Daclatasvir: The NS5A inhibitor daclatasvir is a substrate of CYP3A. When daclatasvir is
given with a CYP3A inhibitor, the levels of daclatasvir can increase, particularly with strong
inhibitors of CYP3A. The dose of daclatasvir should therefore be reduced to 30 mg when used
with either ritonavir-boosted atazanavir or lopinavir. In contrast, when used with efavirenz, a
CYP3A inducer, the dose of daclatasvir should be increased to 90 mg daily.
Ledipasvir-Sofosbuvir: The NS5A inhibitor ledipasvir is not metabolized by the cytochrome
p450 system, but is a substrate of p-glycoprotein. Ledipasvir increases tenofovir levels by 1.3
to 2.6 fold when concomitantly given with either rilpivirine or efavirenz. Although ledipasvir
administered concomitantly with tenofovir and an HIV protease inhibitor has not been
studied, there is concern that tenofovir levels may increase substantially with this
combination. Because of this concern and lack of data, the use of ledipasvir with ritonavirboosted HIV protease inhibitors should, if possible, be avoided. For similar reasons, ledipasvirsofosbuvir should not be used with cobicistat, elvitegravir, or tipranavir. Ledipasvir-sofosbuvir
should not be used in HIV-infected patients on tenofovir if the baseline creatinine clearance is
less than 60 ml/min.
Ombitasvir-Paritaprevir-Ritonavir: The major concern for drug interaction with this
regimen is the significant p450 inhibition generated by ritonavir. This combination regimen
should not be used with efavirenz, rilpivirine, darunavir, or lopinavir-ritonavir.
Ombitasvir-Paritaprevir-Ritonavir and Dasabuvir: The major concern for drug
interaction with this regimen is the significant p450 inhibition generated by ritonavir. This
combination regimen should not be used with efavirenz, rilpivirine, darunavir, or lopinavirritonavir.
Peginterferon alfa: The metabolism of peginterferon alfa occurs predominantly via CYP1A2.
No major drug-drug interactions exist with peginterferon and antiretroviral medications.
Ribavirin: Significant and serious toxic drug-drug interactions and severe toxicities can
occur with the simultaneous use of ribavirin and certain HIV nucleoside reverse transcriptase
inhibitors. The use of ribavirin with didanosine is strictly contraindicated due to a marked
increase in intracellular didanosine levels, which may cause hepatic failure, pancreatitis, and
lactic acidosis. This can also occur with stavudine or zidovudine. Thus, simultaneous use of
ribavirin with either didanosine, stavudine, or zidovudine should be avoided. Concurrent use
of ribavirin and zidovudine should also be avoided because of additive hematologic toxicity
and increased risk of severe anemia with this combination.
Simeprevir: This NS34A HCV protease inhibitor has complex interactions with antiretroviral
medications because it is a substrate and an inhibitor of CYP3A4 and p-glycoprotein. In
addition, simeprevir inhibits the OATP1B1/3 drug transporter. Simeprevir should not be used
concomitantly with any of the following medications: efavirenz, etravirine, nevirapine, any
HIV protease inhibitors, or any regimen that contains cobicistat. Simeprevir can be used with
reverse transcriptase inhibitors, rilpivirine, dolutegravir, and raltegravir; if used with
maraviroc, the dose of maraviroc should be decreased to 150 mg twice daily.
Sofosbuvir: This NS5B polymerase inhibitor is rapidly converted to a dominant circulating
metabolite (GS-331007). Sofosbuvir is not metabolized by the cytochrome p450 system, but
is a substrate of p-glycoprotein. The only significant interaction with antiretroviral
medications occurs with the p-glycoprotein inducer tipranavir, which may decrease levels of
sofosbuvir and the GS-331007 metabolite. Accordingly sofosbuvir should not be used
concomitantly with tipranavir, but it can be use with all other antiretrovirals.
5 / 20
Future HCV Treatment Options in Patients with HIV Coinfection
Several all-oral investigational regimens have shown promising preliminary results for the treatment
of HCV in persons coinfected with HIV.
Grazoprevir-Elbasvir: Grazoprevir is an NS3/4A protease inhibitor under study with
elbasvir, an NS5A replication complex inhibitor. In the phase 3, open label C-EDGE trial,
investigators treated 218 treatment-naive patients with genotype 1, 4, or 6 HCV (and HIV
coinfection) with a 12-week course of the once daily fixed-dose combination of grazoprevir
(100 mg) and elbasvir (50 mg). Patients were eligible to enroll if (a) they were on
antiretroviral therapy for at least 8 weeks, had an undetectable HIV RNA level, and had a CD4
count greater than 200 cells/mm3 or (b) they had a CD4 count greater than 500
cells/mm3 and an HIV RNA level less than 50,000 copies/ml. Overall, 210 (96%) of 218
patients achieved an SVR12. Analysis for all patients showed similar SVR rates with genotype
1a, 1b, and 4. The regimen was well tolerated, including patients with cirrhosis.
6 / 20
Summary Points
In patients with chronic hepatitis C, coinfection with HIV can accelerate the progression of
hepatic fibrosis. Therefore, treatment of HCV should have high priority in coinfected patients.
The introduction of direct-acting antiviral agents (DAAs), and in particular interferon-free
combination therapy, has changed the landscape of therapy for patients coinfected with HCV
and HIV, with multiple studies demonstrating comparable rates of sustained virologic
response in coinfected and monoinfected patients.
The AASLD/IDSA HCV Guidance recommends using the same HCV treatment approach for
patients coinfected with HIV as those with HCV monoinfection, except that in coinfected
patients special consideration should be given to monitoring and managing drug-drug
interactions.
The use of peginterferon and ribavirin alone or peginterferon and ribavirin plus either
boceprevir or telaprevir is no longer recommended for treatment of HCV in coinfected
patients (or HCV monoinfected patients) in HIV-infected patients (or HCV monoinfected
patients).
Antiretroviral therapy may slow liver disease progression in HIV/HCV coinfected patients and
should therefore be considered for all coinfected patients regardless of CD4 cell count.
For coinfected patients whose CD4 cell counts are less than 200 cells/mm3, it may be
advisable to wait for further immune reconstitution prior to initiating HCV therapy,
particularly since most HCV treatment trials have excluded such patients.
7 / 20
References
AASLD/IDSA. Recommendations for testing, management, and treating hepatitis C. Unique
patient populations: patients with HIV/HCV confection.
[AASLD/IDSA Hepatitis C Guidance] Avidan NU, Goldstein D, Rozenberg L, et al. Hepatitis C viral kinetics during treatment with
peg IFN-alpha-2b in HIV/HCV coinfected patients as a function of baseline CD4+ T-cell counts.
J Acquir Immune Defic Syndr. 2009;52:452-8.
[PubMed Abstract] Berenguer J, González-García J, López-Aldeguer J, et al. Pegylated interferon {alpha}2a plus
ribavirin versus pegylated interferon {alpha}2b plus ribavirin for the treatment of chronic
hepatitis C in HIV-infected patients. J Antimicrob Chemother. 2009;63:1256-63.
[PubMed Abstract] Bichoupan K, Dieterich DT, Martel-Laferrière V. HIV-hepatitis C virus co-infection in the era of
direct-acting antivirals. Curr HIV/AIDS Rep. 2014;11:241-9.
[PubMed Abstract] Cachay ER, Hill L, Wyles D, et al. The hepatitis C cascade of care among HIV infected
patients: a call to address ongoing barriers to care. PLoS One. 2014;9:e102883.
[PubMed Abstract] Carrat F, Bani-Sadr F, Pol S, et al. Pegylated interferon alfa-2b vs standard interferon alfa-2b,
plus ribavirin, for chronic hepatitis C in HIV-infected patients: a randomized controlled trial.
JAMA. 2004;292:2839-48.
[PubMed Abstract] Centers for Disease Control and Prevention (CDC). Sexual transmission of hepatitis C virus
among HIV-infected men who have sex with men--New York City, 2005-2010. MMWR Morb
Mortal Wkly Rep. 2011;60:945-50.
[CDC and MMWR] Chung RT, Andersen J, Volberding P, et al. Peginterferon Alfa-2a plus ribavirin versus
interferon alfa-2a plus ribavirin for chronic hepatitis C in HIV-coinfected persons. N Engl J
Med. 2004;351:451-9.
[PubMed Abstract] Di Martino V, Rufat P, Boyer N, et al. The influence of human immunodeficiency virus
coinfection on chronic hepatitis C in injection drug users: a long-term retrospective cohort
study. Hepatology. 2001;34:1193-9.
[PubMed Abstract] Dieterich D, Nelson M, Soriano V, et al. Faldaprevir and pegylated interferon α-2a/ribavirin in
individuals co-infected with hepatitis C virus genotype-1 and HIV. AIDS. 2015;29:571-81.
[PubMed Abstract] Dieterich D, Rockstroh JK, Orkin C, et al. Simeprevir (TMC435) with pegylated
interferon/ribavirin in patients coinfected with HCV genotype 1 and HIV-1: a phase 3 study.
Clin Infect Dis. 2014;59:1579-87.
[PubMed Abstract] European Association for the Study of the Liver. EASL recommendations on treatment of
hepatitis C 2015.
8 / 20
[EASL] Hagan LM, Sulkowski MS, Schinazi RF. Cost analysis of sofosbuvir/ribavirin versus
sofosbuvir/simeprevir for genotype 1 hepatitis C virus in interferon-ineligible/intolerant
individuals. Hepatology. 2014;60:37-45.
[PubMed Abstract] Joshi D, O'Grady J, Dieterich D, Gazzard B, Agarwal K. Increasing burden of liver disease in
patients with HIV infection. Lancet. 2011;377:1198-209.
[PubMed Abstract] Kirk GD, Mehta SH, Astemborski J, et al. HIV, age, and the severity of hepatitis C virus-related
liver disease: a cohort study. Ann Intern Med. 2013;158:658-66.
[PubMed Abstract] Kohli A, Osinusi A, Sims Z, et al. Virological response after 6 week triple-drug regimens for
hepatitis C: a proof-of-concept phase 2A cohort study. Lancet. 2015;385:1107-13.
[PubMed Abstract] Kowdley KV, Gordon SC, Reddy KR, et al. Ledipasvir and sofosbuvir for 8 or 12 weeks for
chronic HCV without cirrhosis. N Engl J Med. 2014;370:1879-88.
[PubMed Abstract] Laguno M, Cifuentes C, Murillas J, et al. Randomized trial comparing pegylated interferon
alpha-2b versus pegylated interferon alpha-2a, both plus ribavirin, to treat chronic hepatitis C
in human immunodeficiency virus patients. Hepatology. 2009;49:22-31.
[PubMed Abstract] Laguno M, Murillas J, Blanco JL, et al. Peginterferon alfa-2b plus ribavirin compared with
interferon alfa-2b plus ribavirin for treatment of HIV/HCV co-infected patients. AIDS.
2004;18:F27-36.
[PubMed Abstract] Martel-Laferrière V, Brinkley S, Bichoupan K, et al. Virological response rates for telaprevirbased hepatitis C triple therapy in patients with and without HIV coinfection. HIV Med.
2013;15:108-15.
[PubMed Abstract] Molina JM, Orkin C, Iser DM, et al. Sofosbuvir plus ribavirin for treatment of hepatitis C virus in
patients co-infected with HIV (PHOTON-2): a multicentre, open-label, non-randomised, phase
3 study. Lancet. 2015;385:1098-106.
[PubMed Abstract] Naggie S, Cooper C, Saag M, et al. Ledipasvir and sofosbuvir for HCV in patients coinfected
with HIV-1. N Engl J Med. 2015;373:705-13.
[PubMed Abstract] Núñez M, Miralles C, Berdún MA, et al. Role of weight-based ribavirin dosing and extended
duration of therapy in chronic hepatitis C in HIV-infected patients: the PRESCO trial. AIDS Res
Hum Retroviruses. 2007;23:972-82.
[PubMed Abstract] Osinusi A, Meissner EG, Lee YJ, et al. Sofosbuvir and ribavirin for hepatitis C genotype 1 in
patients with unfavorable treatment characteristics: a randomized clinical trial. JAMA.
2013;310:804-11.
9 / 20
[PubMed Abstract] Osinusi A, Townsend K, Kohli A, et al. Virologic response following combined ledipasvir and
sofosbuvir administration in patients with HCV genotype 1 and HIV co-infection. JAMA.
2015;313:1232-9.
[PubMed Abstract] Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of
antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and
Human Services. Considerations for antiretroviral use in patients with confections: hepatitis C
(HCV)/HIV confection. April 8, 2015.
[AIDSinfo] Panel on Opportunistic Infections in HIV-Infected Adults and Adolescents. Guidelines for the
prevention and treatment of opportunistic infections in HIV-infected adults and adolescents:
recommendations from the Centers for Disease Control and Prevention, the National
Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of
America. Hepatitis C virus infection. October 28, 2014.
[AIDSinfo] Piroth L, Paniez H, Taburet AM, et al. High Cure Rate With 24 Weeks of Daclatasvir-Based
Quadruple Therapy in Treatment-Experienced, Null-Responder Patients With HIV/Hepatitis C
Virus Genotype 1/4 Coinfection: The ANRS HC30 QUADRIH Study. Clin Infect Dis.
2015;61:817-25.
[PubMed Abstract] Rockstroh JK, Nelson M, Katlama C, et al. Efficacy and safety of grazoprevir (MK-5172) and
elbasvir (MK-8742) in patients with hepatitis C virus and HIV co-infection (C-EDGE COINFECTION): a non-randomised, open-label trial. Lancet HIV. 2015;2:e319-27.
[PubMed Abstract] Rockstroh JK, Spengler U. HIV and hepatitis C virus co-infection. Lancet Infect Dis.
2004;4:437-44.
[PubMed Abstract] Rodriguez-Torres M, Gaggar A, Shen G, et al. Sofosbuvir for chronic hepatitis C virus infection
genotype 1-4 in patients coinfected with HIV. J Acquir Immune Defic Syndr. 2015;68:543-9.
[PubMed Abstract] Sulkowski M, Hezode C, Gerstoft J, et al. Efficacy and safety of 8 weeks versus 12 weeks of
treatment with grazoprevir (MK-5172) and elbasvir (MK-8742) with or without ribavirin in
patients with hepatitis C virus genotype 1 mono-infection and HIV/hepatitis C virus coinfection (C-WORTHY): a randomised, open-label phase 2 trial. Lancet. 2015;385:1087-97.
[PubMed Abstract] Sulkowski M, Pol S, Mallolas J, et al. Boceprevir versus placebo with pegylated interferon
alfa-2b and ribavirin for treatment of hepatitis C virus genotype 1 in patients with HIV: a
randomised, double-blind, controlled phase 2 trial. Lancet Infect Dis. 2013;13:597-605.
[PubMed Abstract] Sulkowski MS, Eron JJ, Wyles D, et al. Ombitasvir, paritaprevir co-dosed with ritonavir,
dasabuvir, and ribavirin for hepatitis C in patients co-infected with HIV-1: a randomized trial.
JAMA. 2015;313:1223-31.
[PubMed Abstract] -
10 / 20
Sulkowski MS, Naggie S, Lalezari J, et al. Sofosbuvir and ribavirin for hepatitis C in patients
with HIV coinfection. JAMA. 2014;312:353-61.
[PubMed Abstract] Sulkowski MS, Poordad F, Manns MP, et al. Anemia during treatment with peginterferon
Alfa-2b/ribavirin and boceprevir: Analysis from the serine protease inhibitor therapy 2
(SPRINT-2) trial. Hepatology. 2013;57:974-84.
[PubMed Abstract] Sulkowski MS, Sherman KE, Dieterich DT, et al. Combination therapy with telaprevir for
chronic hepatitis C virus genotype 1 infection in patients with HIV: a randomized trial. Ann
Intern Med. 2013;159:86-96.
[PubMed Abstract] Thomas DL, Bartlett JG, Peters MG, Sherman KE, Sulkowski MS, Pham PA. Provisional
guidance on the use of hepatitis C virus protease inhibitors for treatment of hepatitis C in HIVinfected persons. Clin Infect Dis. 2012;54:979-83.
[PubMed Abstract] Thomas DL. The challenge of hepatitis C in the HIV-infected person. Annu Rev Med.
2008;59:473-85.
[PubMed Abstract] Torriani FJ, Rodriguez-Torres M, Rockstroh JK, et al. Peginterferon alfa-2a plus ribavirin for
chronic hepatitis C virus infection in HIV-infected patients. N Engl J Med. 2004;351:438-50.
[PubMed Abstract] Wyles DL, Ruane PJ, Sulkowski MS, et al. Daclatasvir plus sofosbuvir for HCV in patients
coinfected with HIV-1. N Engl J Med. 2015;373:714-25.
[PubMed Abstract] -
11 / 20
Figures
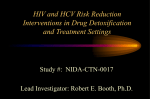
Figure 1 Progression to Cirrhosis in Patients with HCV Monoinfection and HCV-HIV
Coinfection
This graph shows accelerated progression to cirrhosis in patients with HIV-HCV coinfection when
compared with those with HCV monoinfection.
Source: Di Martino V, Rufat P, Boyer N, et al. The influence of human immunodeficiency virus
coinfection on chronic hepatitis C in injection drug users: a long-term retrospective cohort study.
Hepatology. 2001;34:1193-9.
12 / 20
Figure 2 Summary Table of HCV-HIV Coinfection Studies using Peginterferon plus
Ribavirin
1. Chung RT, Andersen J, Volberding P, et al. Peginterferon Alfa-2a plus ribavirin versus interferon
alfa-2a plus ribavirin for chronic hepatitis C in HIV-coinfected persons. N Engl J Med.
2004;351:451-9.
2.Torriani FJ, Rodriguez-Torres M, Rockstroh JK, et al. Peginterferon Alfa-2a plus ribavirin for chronic
hepatitis C virus infection in HIV-infected patients. N Engl J Med. 2004;351:438-50.
3. Laguno M, Murillas J, Blanco JL, et al. Peginterferon alfa-2b plus ribavirin compared with interferon
alfa-2b plus ribavirin for treatment of HIV/HCV co-infected patients. AIDS. 2004;18:F27-36.
4. Carrat F, Bani-Sadr F, Pol S, et al. Pegylated interferon alfa-2b vs standard interferon alfa-2b, plus
ribavirin, for chronic hepatitis C in HIV-infected patients: a randomized controlled trial. JAMA.
2004;292:2839-48.
5.Núñez M, Miralles C, Berdún MA, et al. Role of weight-based ribavirin dosing and extended
duration of therapy in chronic hepatitis C in HIV-infected patients: the PRESCO trial. AIDS Res Hum
Retroviruses. 2007;23:972-82.
5.Núñez M, Miralles C, Berdún MA, et al. Role of weight-based ribavirin dosing and extended
duration of therapy in chronic hepatitis C in HIV-infected patients: the PRESCO trial. AIDS Res Hum
Retroviruses. 2007;23:972-82.
13 / 20
Figure 3 Key HCV-HIV Coinfection Studies using Peginterferon plus Ribavirin
Source
1. Chung RT, Andersen J, Volberding P, et al. Peginterferon Alfa-2a plus ribavirin versus interferon
alfa-2a plus ribavirin for chronic hepatitis C in HIV-coinfected persons. N Engl J Med.
2004;351:451-9.
2.Torriani FJ, Rodriguez-Torres M, Rockstroh JK, et al. Peginterferon Alfa-2a plus ribavirin for chronic
hepatitis C virus infection in HIV-infected patients. N Engl J Med. 2004;351:438-50.
3. Laguno M, Murillas J, Blanco JL, et al. Peginterferon alfa-2b plus ribavirin compared with interferon
alfa-2b plus ribavirin for treatment of HIV/HCV co-infected patients. AIDS. 2004;18:F27-36.
4. Carrat F, Bani-Sadr F, Pol S, et al. Pegylated interferon alfa-2b vs standard interferon alfa-2b, plus
ribavirin, for chronic hepatitis C in HIV-infected patients: a randomized controlled trial. JAMA.
2004;292:2839-48.
5.Núñez M, Miralles C, Berdún MA, et al. Role of weight-based ribavirin dosing and extended
duration of therapy in chronic hepatitis C in HIV-infected patients: the PRESCO trial. AIDS Res Hum
Retroviruses. 2007;23:972-82.
14 / 20
Figure 4 SVR Rates in Treatment-Naive Patients with HCV-HIV Coinfection versus HCV
Monoinfection
1. Wyles DL, Ruane PJ, Sulkowski MS, et al. Daclatasvir plus sofosbuvir for HCV in patients
coinfected with HIV-1. N Engl J Med. 2015;373:714-25.
2. Sulkowski MS, Gardiner DF, Rodriguez-Torres M, et al. Daclatasvir plus sofosbuvir for previously
treated or untreated chronic HCV infection. N Engl J Med. 2014;370:211-21.
3. Naggie S, Cooper C, Saag M, et al. Ledipasvir and sofosbuvir for HCV in patients coinfected with
HIV-1. N Engl J Med. 2015;373:705-13.
4. Afdhal N, Zeuzem S, Kwo P, et al. Ledipasvir and sofosbuvir for untreated HCV genotype 1
infection. N Engl J Med. 2014;370:1889-98.
5. Sulkowski MS, Eron JJ, Wyles D, et al. Ombitasvir, paritaprevir co-dosed with ritonavir, dasabuvir,
and ribavirin for hepatitis C in patients co-infected with HIV-1: a randomized trial. JAMA.
2015;313:1223-31.
6. Ferenci P, Bernstein D, Lalezari J, et al. ABT-450/r-ombitasvir and dasabuvir with or without
ribavirin for HCV. N Engl J Med. 2014;370:1983-92.1. Dieterich D, Rockstroh JK, Orkin C, et al.
7. Rockstroh JK, Nelson M, Katlama C, et al. Efficacy and safety of grazoprevir (MK-5172) and
elbasvir (MK-8742) in patients with hepatitis C virus and HIV co-infection (C-EDGE CO-INFECTION): a
non-randomised, open-label trial. Lancet HIV. 2015;2:e319-27.
8. Zeuzem S, Ghalib R, Reddy KR, et al. Grazoprevir-Elbasvir Combination Therapy for TreatmentNaive Cirrhotic and Noncirrhotic Patients With Chronic Hepatitis C Virus Genotype 1, 4, or 6
Infection: A Randomized Trial. Ann Intern Med. 2015;163:1-13.
15 / 20
Figure 5 (Image Series) - Interactions with HIV Antiretroviral and HCV Medications
(Image Series) - Figure 5 (Image Series) - Interactions with HIV Antiretroviral and HCV
Medications
Image 5A: HCV DAAs and HIV Nucleoside Reverse Transcriptase Inhibitors
Source: Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of
antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human
Services. Drug interactions: drug interactions between nucleoside reverse transcriptase inhibitors
and other drugs. April 8, 2015.
16 / 20
Figure 5 (Image Series) - Interactions with HIV Antiretroviral and HCV Medications
Image 5B: HCV DAAs and HIV Non-nucleoside Reverse Transcriptase Inhibitors
Source: Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of
antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human
Services. Drug interactions: drug interactions between non-nucleoside reverse transcriptase
inhibitors and other drugs. April 8, 2015.
17 / 20
Figure 5 (Image Series) - Interactions with HIV Antiretroviral and HCV Medications
Image 5C: HCV DAAs and HIV Protease Inhibitors
Source: Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of
antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human
Services. Drug interactions: drug interactions between protease inhibitors and other drugs. April 8,
2015.
18 / 20
Figure 5 (Image Series) - Interactions with HIV Antiretroviral and HCV Medications
Image 5D: HCV DAAs and HIV Integrase Strand Transfer Inhibitors
Source: Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of
antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human
Services. Drug interactions: drug interactions between integrase inhibitors and other drugs. April 8,
2015.
19 / 20
Figure 5 (Image Series) - Interactions with HIV Antiretroviral and HCV Medications
Image 5E: HCV DAAs and HIV CCR5 Antagonist
Source: Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of
antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human
Services. Drug interactions: drug interactions between CCR5 antagonist and other drugs. April 8,
2015.
20 / 20
Powered by TCPDF (www.tcpdf.org)