Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Impact of CDC’s HIV Preexposure Prophylaxis
Guidelines among MSM in the United States
Samuel M. Jenness,1 Steven M. Goodreau,2 Eli Rosenberg,1
Emily N. Beylerian,2 Karen W. Hoover,3 Dawn K. Smith,3 Patrick Sullivan1
1
Department of Epidemiology, Emory University
2
Center for Studies in Demography & Ecology, University of Washington
3
Division of HIV/AIDS Prevention, Centers for Disease Control and Prevention
Using EpiModel for HIV Prevention Science:
A Motivating Example
Network Modeling for Epidemics Course
August 2016 | Seattle
Samuel M. Jenness, PhD MPH
Department of Epidemiology, Emory University
samueljenness.orgsmjenness@SamuelJenness
Background
PrEP is More Effective When Adherence is Better
•
Efficacy of daily oral
PrEP established in
several RCTs
- iPrex trial among MSM
and TG women: 44%
incidence reduction in
intent-to-treat analyses
- Secondary iPrEx analyses
suggest non-linear doseresponse effect
Grant, 2014, Lancet Infect Dis
Adherence is Better When Effectiveness is Known
CDC PrEP Guidelines for Clinical Practice
•
US PHS/CDC released clinical practice guidelines indicating
PrEP for those at “substantial risk” in 2014
•
For MSM, prescription indications were:
- Unprotected anal intercourse (UAI) in monogamous partnership with
person not recently tested for HIV
- UAI outside of a monogamous partnership
- AI (including with condoms) in a known serodiscordant partnership
- Any non-HIV STI diagnosis
•
Clinicians recommended to screen for conditions in past 6
months, reevaluate risk every 12 months
Results
Results by CDC Guideline Indication
Percent of Infections Averted in Joint Scenario
Linear growth with asymptotic
uptake and downstream
prevention effects
Rapid growth with PrEP scale-up
at HIV testing events
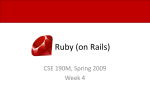
Interaction of Adherence and Coverage
Adherence
% of MSM who were
highly adherent (4+ pills /
week)
Coverage
% of CDC-indicated MSM
who initiate PrEP
Interaction of Adherence and Coverage
Adherence
% of MSM who were
highly adherent (4+ pills /
week)
Coverage
% of CDC-indicated MSM
who initiate PrEP
Web-Based Modeling Tool for Public Health Practice
http://prism.shinyapps.io/cdc-prep-guidelines/
Why did we use a mathematical/mechanistic model?
What makes this a network model?
Why did we use a network model?
How did we use EpiModel to do this?
Why Model?
Clinical trials
establish efficacy
at individual level
Population
Models
Models predict
effectiveness (and
other things) at
population level
Administrative
Studies
Scope
Demonstration
Studies
Individual
Clinical Trials
Past
Time Frame
Future
Models also allow
studying
unmeasurable
outcomes and
empirically
infeasible
counterfactuals
Study Aims
•
Model HIV transmission dynamics among MSM in the US
after implementation of PrEP according to CDC guidelines
- Use a robust mathematical framework to represent complex MSM biobehavioral population evolution
•
Quantify reduction in HIV incidence associated with:
- Individual behavioral criteria in the guidelines, separately and
jointly
- Varying levels of PrEP coverage, adherence
Why did we use a mathematical/mechanistic model?
What makes this a network model?
Why did we use a network model?
How did we use EpiModel to do this?
Methods Overview
•
Stochastic network-based mathematical model
•
Model parameters based on robust, partnership-based HIV
incidence studies of MSM in Atlanta and national-level data
on clinical care engagement
•
Epidemiological, demographic, and intervention modules
designed in EpiModel software (www.epimodel.org)
•
Simulates open population of MSM, aged 18 to 40, in the US
over a 10-year time span
HIV Transmission over Dynamic Sexual Networks
•
•
•
Temporal exponential random graph
models (ERGMs) define partnership
formation and dissolution
-
Sexual network types: main, casual, one-off
-
Men form partnerships according to model terms
based on numbers of each partner type, mixing on
race and age, sexual role segregation
HIV epidemiology
-
Natural history (disease stages, continuous VL, HIV-related mortality)
-
ART initiation and adherence
-
HIV transmission dynamics within serodiscordant partnerships
Demographic processes
Why did we use a mathematical/mechanistic model?
What makes this a network model?
Why did we use a network model?
How did we use EpiModel to do this?
Linking Behavior to Biomedical Prevention
•
US PHS/CDC released clinical practice guidelines indicating
PrEP for those at “substantial risk” in 2014
•
For MSM, prescription indications were:
- Unprotected anal intercourse (UAI) in monogamous partnership
with person not recently tested for HIV
- UAI outside of a monogamous partnership
- AI (including with condoms) in a known serodiscordant partnership
- Any non-HIV STI diagnosis
•
Clinicians recommended to screen for conditions in past
6 months, reevaluate risk every 12 months
Representing Complexities in PrEP
Initiation
•
•
-
HIV-uninfected men encounter diagnostic HIV testing
-
Risk assessment for PrEP over past 6-month window based on CDC
behavioral indications
-
Indicated men start PrEP if the % of already initiated men is less than a
fixed coverage threshold (40% in base models)
Adherence
-
Men assigned a fixed adherence profile following PrEP demonstration
project data (62% high, 10% moderate, 7% low, and 21% null
adherence)
-
Adherence translates into a 95%, 81%, 31%, and 0% reduction in
transmission risk
-
Men discontinued from PrEP if, at yearly follow-up visit, no longer
behavioral indications
Why did we use a mathematical/mechanistic model?
What makes this a network model?
Why did we use a network model?
How did we use EpiModel to do this?
EpiModel is Modular
Most of this week (Mon to Thurs)
•
•
-
We will focus on generic epidemics (SI/SIS/SIR) in basic population
structures
-
While learning the theory and math of modeling dynamic networks
-
The “out of the box” models in EpiModel are not intended to address
complex research questions
Then on Friday (and thereafter)
-
We teach you about how to translate your modeling questions to
EpiModel code
-
This involves adding and replacing modules within EpiModel
-
This is exactly what we do in our modeling research
Translating Concept to Code
Diagnosis
Viral Load
Transmission
Treatment
Behavior
CD4 Count
Mortality
Monday to Thursday
Susceptible
Infected
Recovered
Friday
Diagnosis
Viral Load
Transmission
Treatment
Behavior
CD4 Count
Mortality
After the Course
sti_recov<-function(dat,at){
recovRGC<-c(recovRGC_asympt,recovRGC_tx,recovRGC_ntx)
recovUGC<-c(recovUGC_asympt,recovUGC_tx,recovUGC_ntx)
#Parameters
rgc.dur.asympt<-dat$param$rgc.dur.asympt
ugc.dur.asympt<-dat$param$ugc.dur.asympt
gc.dur.tx<-dat$param$gc.dur.tx
gc.dur.ntx<-dat$param$gc.dur.ntx
dat$attr$rGC[recovRGC]<-0
dat$attr$rGC.sympt[recovRGC]<-NA
dat$attr$rGC.infTime[recovRGC]<-NA
dat$attr$rGC.tx[recovRGC]<-NA
rct.dur.asympt<-dat$param$rct.dur.asympt
uct.dur.asympt<-dat$param$uct.dur.asympt
ct.dur.tx<-dat$param$ct.dur.tx
ct.dur.ntx<-dat$param$ct.dur.ntx
dat$attr$uGC[recovUGC]<-0
dat$attr$uGC.sympt[recovUGC]<-NA
dat$attr$uGC.infTime[recovUGC]<-NA
dat$attr$uGC.tx[recovUGC]<-NA
dat$attr$GC.cease[c(recovRGC,recovUGC)]<-NA
#GCrecovery
idsRGC_asympt<-which(dat$attr$rGC==1&dat$attr$rGC.infTime<at&
dat$attr$rGC.sympt==0)
idsUGC_asympt<-which(dat$attr$uGC==1&dat$attr$uGC.infTime<at&
dat$attr$uGC.sympt==0)
idsRGC_tx<-which(dat$attr$rGC==1&dat$attr$rGC.infTime<at&
dat$attr$rGC.sympt==1&dat$attr$rGC.tx==1)
idsUGC_tx<-which(dat$attr$uGC==1&dat$attr$uGC.infTime<at&
dat$attr$uGC.sympt==1&dat$attr$uGC.tx==1)
idsRGC_ntx<-which(dat$attr$rGC==1&dat$attr$rGC.infTime<at&
dat$attr$rGC.sympt==1&dat$attr$rGC.tx==0)
idsUGC_ntx<-which(dat$attr$uGC==1&dat$attr$uGC.infTime<at&
dat$attr$uGC.sympt==1&dat$attr$uGC.tx==0)
#CTrecovery
idsRCT_asympt<-which(dat$attr$rCT==1&dat$attr$rCT.infTime<at&
dat$attr$rCT.sympt==0)
idsUCT_asympt<-which(dat$attr$uCT==1&dat$attr$uCT.infTime<at&
dat$attr$uCT.sympt==0)
idsRCT_tx<-which(dat$attr$rCT==1&dat$attr$rCT.infTime<at&
dat$attr$rCT.sympt==1&dat$attr$rCT.tx==1)
idsUCT_tx<-which(dat$attr$uCT==1&dat$attr$uCT.infTime<at&
dat$attr$uCT.sympt==1&dat$attr$uCT.tx==1)
idsRCT_ntx<-which(dat$attr$rCT==1&dat$attr$rCT.infTime<at&
dat$attr$rCT.sympt==1&dat$attr$rCT.tx==0)
idsUCT_ntx<-which(dat$attr$uCT==1&dat$attr$uCT.infTime<at&
dat$attr$uCT.sympt==1&dat$attr$uCT.tx==0)
recovRGC_asympt<-idsRGC_asympt[which(rbinom(length(idsRGC_asympt),1,
1/rgc.dur.asympt)==1)] recovRCT_asympt<-idsRCT_asympt[which(rbinom(length(idsRCT_asympt),
recovUGC_asympt<-idsUGC_asympt[which(rbinom(length(idsUGC_asympt),1, 1,1/rct.dur.asympt)==1)]
1/ugc.dur.asympt)==1)] recovUCT_asympt<-idsUCT_asympt[which(rbinom(length(idsUCT_asympt),
1,1/uct.dur.asympt)==1)]
recovRGC_tx<-idsRGC_tx[which(rbinom(length(idsRGC_tx),1,
1/gc.dur.tx)==1)]
recovRCT_tx<-idsRCT_tx[which(rbinom(length(idsRCT_tx),
recovUGC_tx<-idsUGC_tx[which(rbinom(length(idsUGC_tx),1,
1,1/ct.dur.tx)==1)]
1/gc.dur.tx)==1)]
recovUCT_tx<-idsUCT_tx[which(rbinom(length(idsUCT_tx),
1,1/ct.dur.tx)==1)]
if(!is.null(gc.dur.ntx)){
recovRGC_ntx<-idsRGC_ntx[which(rbinom(length(idsRGC_ntx),1,
if(!is.null(ct.dur.ntx)){
1/gc.dur.ntx)==1)]
recovRCT_ntx<-idsRCT_ntx[which(rbinom(length(idsRCT_ntx),
recovUGC_ntx<-idsUGC_ntx[which(rbinom(length(idsUGC_ntx),1,
1,1/ct.dur.ntx)==1)]
1/gc.dur.ntx)==1)]
recovUCT_ntx<-idsUCT_ntx[which(rbinom(length(idsUCT_ntx),
}else{
1,1/ct.dur.ntx)==1)]
recovRGC_ntx<-idsRGC_ntx[which(rbinom(length(idsRGC_ntx),1,
}else{
1/rgc.dur.asympt)==1)]
recovRCT_ntx<-idsRCT_ntx[which(rbinom(length(idsRCT_ntx),
recovUGC_ntx<-idsUGC_ntx[which(rbinom(length(idsUGC_ntx),1,
1,1/rct.dur.asympt)==1)]
1/ugc.dur.asympt)==1)]
recovUCT_ntx<-idsUCT_ntx[which(rbinom(length(idsUCT_ntx),
}
1,1/uct.dur.asympt)==1)]
}
After the Course
After the Course
The Journal of Infectious Diseases
MAJOR ARTICLE
Impact of the Centers for Disease Control’s HIV
Preexposure Prophylaxis Guidelines for Men Who Have
Sex With Men in the United States
Samuel M. Jenness,1 Steven M. Goodreau,4 Eli Rosenberg,1 Emily N. Beylerian,5 Karen W. Hoover,3 Dawn K. Smith,3 and Patrick Sullivan1,2
Departments of 1Epidemiology, and 2Global Health, Emory University, and 3Division of HIV/AIDS Prevention, Centers for Disease Control and Prevention, Atlanta, Georgia; 4Department of Anthropology,
and 5Center for Studies in Demography and Ecology, University of Washington, Seattle
Background. Preexposure prophylaxis (PrEP) is effective for preventing human immunodeficiency virus (HIV) infection among
men who have sex with men (MSM) within trial settings. Population impact will depend on clinical indications for PrEP initiation,
coverage levels, and drug adherence. No modeling studies have estimated the impact of clinical practice guidelines for PrEP issued by
the Centers for Disease Control and Prevention (CDC).
Methods. Mathematical models of HIV transmission among MSM were used to estimate the percentage of infections averted
(PIA) and the number needed to treat (NNT) under behavioral indications of the CDC’s PrEP guidelines. We modeled the contribution of these indications while varying treatment coverage and adherence.
Results. At 40% coverage of indicated MSM over the next decade, application of CDC guidelines would avert 1162 infections per
100 000 person-years, 33.0% of expected infections. The predicted NNT for the guidelines would be 25. Increasing coverage and
adherence jointly raise the PIA, but reductions to the NNT were associated with better adherence only.
Conclusions. Implementation of CDC PrEP guidelines would result in strong and sustained reductions in HIV incidence among
MSM in the United States. The guidelines strike a good balance between epidemiological impact (PIA) and efficiency (NNT) at
plausible scale-up levels. Adherence counseling could maximize public health investment in PrEP by decreasing the NNT.
Keywords. HIV; men who have sex with men; preexposure prophylaxis; clinical guidelines; mathematical model; sexual
network.
The efficacy of daily oral antiretroviral preexposure prophylaxis
(PrEP) for the prevention of human immunodeficiency virus
(HIV) infection was established in several randomized controlled trials (RCTs), including the iPrEx study that tested the
tenofovir disoproxil fumarate and emtricitabine formulation
among men who have sex with men (MSM) [1]. Intent-totreat analyses estimated a prevention benefit of 44%, with efficacy at 73% among those with high self-reported adherence and
92% among those with serum-detectable drug levels [2]. Poor
adherence had been a problem in establishing efficacy of
PrEP in some RCTs [3], but subsequent demonstration studies
have found stronger adherence in open-label settings [4, 5].
In response to these trial results, the US Food and Drug Administration approved a label indication for the prescription of
Truvada for PrEP among uninfected persons at high risk of infection [6], and the Centers for Disease Control and Prevention
(CDC) subsequently released guidelines for its use in clinical
Received 18 February 2016; accepted 14 April 2016.
Correspondence: S. M. Jenness, Department of Epidemiology, Emory University, 1518 Clifton
Rd, Atlanta, GA 30322 ([email protected]).
The Journal of Infectious Diseases®
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of
America. All rights reserved. For permissions, e-mail [email protected].
DOI: 10.1093/infdis/jiw223
practice [7]. In these guidelines, PrEP is indicated for MSM
who are at “substantial risk” of infection, defined primarily by
3 behavioral criteria: unprotected (ie, condomless) anal intercourse (UAI) in HIV status–unknown monogamous partnerships, UAI outside a monogamous partnership, and anal
intercourse (AI) in a known-serodiscordant partnership. Sexually transmitted infection diagnoses, another criterion, are considered biological indications of risky sexual activity. For each
criterion, clinicians should query these indications over the
prior 6 months; any events during that “risk window” trigger
a possible indication for PrEP. The CDC supports PrEP use
as part of a comprehensive prevention plan that includes
other biomedical and behavioral prevention strategies.
The guidelines’ criteria were devised based on analyses of
RCT data [8]. However, persons eligible for and willing to participate in RCTs may not represent the broader target population for interventions [9]. Public PrEP programs also may not
replicate the extensive ancillary risk reduction and adherence
counseling components within research settings [10]. It is therefore critical to understand the impact of different schemes for
targeting PrEP on population-level HIV incidence. Mathematical models provide one approach to estimating PrEP impact
[11, 12], but PrEP models of MSM to date have modeled uptake
schemes that differ from the CDC guidelines [13] or use static
Impact of CDC HIV PrEP Guidelines for MSM
•
JID
•
1