Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
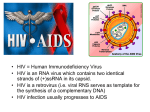
HIV Drugs and the HIV Lifecycle by Liz Highleyman July 2003 The Basics HIV drugs cannot cure HIV but they can prevent the virus from replicating (reproducing or making copies of itself). When HIV cannot reproduce, it cannot infect new cells in your body. So basically, all HIV drugs work by interrupting HIV’s lifecycle to stop it from reproducing, and thereby to “stop it in its tracks.” HIV’s lifecycle is complex, and different classes of HIV drugs target different stages or steps. There are currently four approved classes of HIV drugs: Entry inhibitors Nucleoside and nucleotide reverse transcriptase inhibitors Non-nucleoside reverse transcriptase inhibitors Protease inhibitors The HIV Lifecycle in Brief Once HIV is in the body, it targets and infects a certain type of white blood cell called a CD4 cell. HIV then takes over or “hijacks” these cells and turns them into virus factories that can produce thousands of viral copies. The steps HIV goes through to complete this process are as follows: 1. Entry HIV enters a cell by binding (or attaching) itself to specific points, called receptors, on the cell’s surface. Once HIV gets inside a cell, it releases its own genetic material and enzymes. 2. Reverse Transcription HIV’s genetic material comes in a form known as RNA. The RNA contains the “instructions" that will reprogram the CD4 cell’s machinery to produce more viruses. In order to be effective, HIV’s RNA must be converted into DNA. This conversion process depends on an HIV enzyme called reverse transcriptase. (You’ll notice that the words “reverse transcriptase” are part of many HIV drug names.) 3. Integration Next, the newly copied DNA is inserted into the genetic material of the CD4 cell. This is done with the help of another HIV enzyme called integrase. 4. Cleavage Once the virus has become part of (is integrated into) the CD4 cell, it can start making new HIV proteins. New HIV proteins are produced in the form of long chains. These chains have to be cut up into smaller pieces, and then reassembled (or put back together in a certain way) in order to become new HIV virus. This cutting process depends on a third HIV enzyme called protease. 5. Assembly and Budding Finally, the cut-up pieces are put together to form new virus particles, which then “bud” back out of the original CD4 cell. This new virus goes on to target and infect other cells. Types of HIV Drugs Entry Inhibitors These drugs stop (inhibit) HIV from entering a host cell. If HIV can’t get in, it can’t replicate and make new viruses. There are different types of entry inhibitors including chemokine blockers and fusion inhibitors. Entry inhibitors are the newest HIV drug class. There is currently just one fusion inhibitor available, Fuzeon (enfuvirtide, or T-20), but researchers are studying many others. Reverse Transcriptase Inhibitors These drugs interfere with the reverse transcriptase enzyme in order to prevent HIV from replicating. Reverse transcriptase inhibitors are the oldest class of HIV drugs. There are three different types of drugs in this class: 1. Nucleoside Reverse Transcriptase Inhibitors (NRTIs). Approved NRTIs include Retrovir (zidovudine or AZT), Videx (didanosine or ddI), Hivid (zalcitabine or ddC), Zerit (stavudine or d4T), Epivir (lamivudine or 3TC), Ziagen (abacavir), Combivir (Retrovir plus Epivir), Trizivir (Retrovir plus Epivir plus Ziagen), Emtriva (emtricitabine or FTC), Epzicom (Epivir plus Ziagen),Truvada (Emtriva plus Viread), and Atripla (Sustiva plus Emtriva and Viread). . 2. Nucleotide Reverse Transcriptase Inhibitors. There is only one approved nucleotide drug, Viread (tenofovir). 3. Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs). The approved NNRTIs are Viramune (nevirapine), Rescriptor (delavirdine), Sustiva (efavirenz), and Atripla (Sustiva plus Emtriva and Viread). Integrase Inhibitors These drugs interfere with HIV’s integrase enzyme. They prevent HIV from inserting its own genetic material into the host cell, so HIV cannot make new viruses. Currently there are no approved integrase inhibitor drugs, but several experimental ones are being studied. Protease Inhibitors (PIs) These drugs interfere with the action of HIV’s protease enzyme. Protease works as a scissor to cut up newly created protein chains into smaller pieces. These smaller pieces are then used to build new viruses. There are several approved protease inhibitors, including Agenerase (amprenavir), Crixivan (indinavir), Fortovase (saquinavir sgc), Invirase (saquinavir hgc), Viracept (nelfinavir), Norvir (ritonavir), Kaletra, which is actually a blend of lopinavir and ritonavir, Reyataz (atazanavir), Lexiva (fosamprenavir calcium), and Prezista (darunavir, TMC114). Assembly and Budding Inhibitors These experimental HIV drugs are designed to interfere with the final steps of putting together new virus particles (assembly). They also prevent the so-called budding of the new viruses out of the CD4 cell. There are no drugs of this type yet, but several candidates are in early studies. Combining Drug Classes Doctors often combine drugs from different classes in order to attack HIV at more than one point in its lifecycle. This is because HIV can mutate, or change forms, which makes it resistant to specific drugs. (This can cause your HIV drugs to quit working as well, or to “lose efficacy.”) If you take only one drug (monotherapy) or take a few drugs that all belong to one class of drugs, it is very easy for HIV to mutate around that one drug or class. However, HIV has a much harder time mutating in the presence of multiple drugs or drug classes. What does this mean to you? It means that combination therapy with drugs that interfere with HIV at different stages of its lifecycle can prevent most of the production of new HIV. This means slower disease progression and longer life for HIV+ people. The Bottom Line Currently four different classes of HIV drugs target three different stages of HIV’s lifecycle. Attacking HIV on multiple fronts by combining drugs from different classes is the best way to slow or stop HIV replication. It is also the best way to prevent the development of drug resistance. New classes of HIV drugs—and new drugs in the classes already available—will provide more treatment options for HIV+ people in the future.