Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
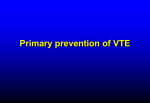
ORIGINAL ARTICLE Venous thromboembolism in patients with head and neck cancer after surgery Leo Thai, BS, Kate McCarn, MD, William Stott, BS, Tammara Watts, MD, Mark K. Wax, MD, Peter E. Andersen, MD, Neil D. Gross, MD* Department of Otolaryngology–Head and Neck Surgery, Oregon Health and Science University, Portland, Oregon. Accepted 3 November 2011 Published online 2 February 2012 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/hed.22920 ABSTRACT: Background. The purpose of this study was to report the incidence of venous thromboembolism (VTE) in patients with head and neck cancer after surgery. Methods. This was a single-institution, retrospective cohort: 134 patients underwent resection and simultaneous microvascular reconstruction. The primary endpoint was identification of confirmed or suspicious VTE within 30 days of surgery. Results. Two subjects (1.4%) with confirmed VTE (1 pulmonary embolism, 1 deep venous thrombosis) and 6 subjects (4.4%) with suspicious VTE (1 acute respiratory failure, 1 sudden cardiac arrest, and 4 cases of leg edema without imaging) were identified. The strongest predictors of possible VTE were prior VTE (p ¼ .004; odds ratio [OR], Venous thromboembolism (VTE) is a potentially lifethreatening condition that includes both deep venous thrombosis (DVT) and pulmonary embolism (PE). Patients with cancer are at increased risk of developing a VTE. Cancer increases the risk of VTE by 4- to 6-fold.1,2 A prothrombic state is also augmented in the surgical setting. Therefore, patients with cancer undergoing major surgery are considered particularly high risk for VTE. Patients with cancer undergoing surgery have a 2-fold risk of developing postoperative VTE compared with patients without cancer undergoing similar procedures.1,3 The morbidity associated with VTE is substantial, ranging from chronic leg swelling to pulmonary embolism. In some cases, VTE can be fatal. In fact, VTE was recently reported to be the most common cause of death in the postoperative period among patients with cancer.4 In accord with current criteria, most patients with head and neck cancer who have surgery are presumed to be high risk for developing VTE.3,5 This is especially true for patients undergoing simultaneous microvascular free tissue transfer reconstruction after resection. The majority of patients with head and neck cancer presenting for oncologic resection and free tissue transfer reconstruction have commonly identified risk factors for VTE, notably *Corresponding author: N. D. Gross, Department of Otolaryngology–Head and Neck Surgery, Oregon Health and Science University, Portland, Oregon. E-mail: [email protected] This work was presented at the 2010 American Head and Neck Society Research Workshop in Washington, DC, October 30, 2010. 4 HEAD & NECK—DOI 10.1002/HED JANUARY 2013 25.11; 95% confidence interval [CI], 1.13–556.40), red cell transfusion (p ¼ .009; OR, 1.80; 95% CI, 1.16–2.80), high body mass index (p ¼ .015, OR, 1.29, 95% CI, 1.05–1.58), and older age (p ¼ .046; OR, 1.10; 95% CI, 1.00–1.19). Conclusion. The incidence of VTE in patients with head and neck cancer after resection and microvascular reconstruction ranged from 1.4% to C 2012 Wiley Periodicals, Inc. Head Neck 35: 4–9, 2013 5.8%. V KEY WORDS: venous thromboembolism, deep venous thrombosis, pulmonary embolism, squamous cell carcinoma, surgery advanced cancer stage, older age, and prolonged surgery time. Surprisingly, there have been few data to quantify the risk of VTE among patients with head and neck cancer undergoing surgery. The primary purpose of our study was to report the incidence of VTE in patients with head and neck cancer after resection and microvascular reconstruction. In addition, we aimed to identify potential risk factors for developing VTE for patients with head and neck cancer and to explore the impact of VTE on survival. MATERIALS AND METHODS Subjects This retrospective study included patients with head and neck cancer treated at Oregon Health and Science University (OHSU) between 2007 and 2009. The study was designed to include patients at highest risk for VTE according to current guidelines for patients with cancer.5,6 Therefore, the study was restricted to patients with malignant disease undergoing a surgical procedure lasting >4 hours. These patients are automatically considered high risk for VTE regardless of other factors including age and comorbidities. The study was further restricted to patients whose surgery included microvascular free-tissue transfer reconstruction to maximize the period for detection of VTE in a high-acuity setting. All patients who undergo microvascular reconstruction at our institution are hospitalized for a minimum of 5 days. All patients included in the study were treated in accord with our institution’s standard of care, including intraoperative VTE sequential compression devices (SCDs) and early ambulation. The conduct of this study was approved by the Institutional Review Board at OHSU. It was hypothesized that the risk of VTE could vary by the timing of cancer treatment.7–9 Therefore, study patients were separated into 2 groups: (1) active head and neck cancer cases (active cancer group) and (2) patients previously treated for head and neck cancer (prior cancer group). The active cancer group included previously untreated patients as well as patients with recurrent or second primary disease. All active patients with cancer were treated surgically with curative intent and planned microvascular reconstruction. The prior cancer group included previously treated patients with head and neck cancer, with no evidence of disease, undergoing secondary reconstruction. This group included patients treated for failed primary reconstruction or for complications from prior treatments (eg, osteoradionecrosis of the mandible). Exposure Potential risk factors for VTE were identified by a thorough review of the current literature prior to abstracting the electronic medical record (Table 1). All established risk factors for VTE were included, such as advanced age, estrogen therapy, prior VTE, comorbidity, chemoradiation, prolonged operative time, and postoperative immobilization.7,10–12 The comorbid conditions specifically analyzed in our study were diabetes mellitus, atrial fibrillation, chronic obstructive pulmonary disease, and peripheral vascular disease. In addition, we also examined obesity (body mass index [BMI]), red cell transfusion, free tissue transfer donor site tourniquet time, and infection, all of which have been reported as potential risk factors for VTE.11,13 Finally, a Caprini risk assessment was performed retrospectively for all cases, to allow for comparison of results to a validated risk stratification tool.14 Data collection We systematically reviewed relevant notes within the electronic medical record to fulfill all desired data fields. Demographic and clinicopathologic data were retrieved from documents including: history and physical examination notes, anesthesia notes, pathology reports, imaging reports, cancer staging forms, operative reports, hospital progress notes, discharge summaries, and outpatient clinic notes. Ambulation time was defined as the first postoperative day the patient was noted to be ambulating by the healthcare team (physician, medical student, nurse, or physical therapist). Ambulation was defined as the independent or assisted ambulatory movement of the patient beyond the bedside or the first nonevaluative day of physical therapy. Daily hospital progress notes were reviewed to identify any reports of leg swelling. All imaging reports were reviewed to determine which patients had a lower extremity ultrasound Doppler and/or spiral CT examination. Discharge summary notes were reviewed for evidence of anticoagulation prescriptions and for orders for outpatient physical therapy. Follow-up data were collected at the dates closest to a 2-week and 1-month follow-up period. AFTER HEAD AND NECK CANCER SURGERY TABLE 1. Patient characteristics. Active cancer group Variable Total patients, N 134 Total cases, n 139 Age, y Mean 65.4 SD 15.9 Sex Male 82 (59%) Female 57 (41%) Smoking status Never 44 (32%) Active 43 (31%) Quit 52 (37%) Body mass index Mean 25.6 SD 5.3 VTE: prior VTE history 7 (5%) Comorbidities DM 21 (15%) Atrial fibrillation 17 (12%) COPD 22 (16%) PVD 14 (10%) Histology Squamous cell carcinoma 106 (76%) Basal cell carcinoma 6 (4%) Melanoma 5 (4%) Adenocarcinoma 5 (4%) Adenoid cystic carcinoma 3 (2%) Other 13 (9%) Medication use ASA 32 (23%) Estrogen 1 (1%) Prior therapy Chemotherapy 13 (9%) Radiation therapy 51 (37%) Prior cancer group p value 26 32 — .78 64.5 15.2 .60 21 (66%) 11 (34%) .005 5 (16%) 5 (16%) 22 (68%) .07 23.6 4.9 0 .42 0 2 (6%) 3 (9%) 3 (9%) .04 .51 .51 1.00 .88 23 (72%) 1 (3%) 1 (3%) 0 2 (6%) 5 (16%) 9 (28%) 3 (9%) .70 .02 9 (28%) 28 (88%) .10 <.001 Abbreviations: SD, standard deviation; VTE, venous thromboembolism; DM, diabetes mellitus; COPD, chronic obstructive pulmonary disease; PVD, peripheral vascular disease; ASA, aspirin. Progress notes were reviewed for findings suggestive of VTE, including postoperative leg edema, leg pain, and respiratory distress. Disease status at last follow-up was confirmed for all patients, including cause of death as applicable. All deaths were confirmed by cross-referencing with the Social Security Death Index database. Endpoints The primary endpoint of the study was possible VTE, which included patients with confirmed VTE or findings suspicious for VTE. Confirmed VTE was defined as either a deep venous thrombosis (DVT) or pulmonary embolism (PE), confirmed by diagnostic imaging. Lower extremity venous duplex ultrasound was used to confirm DVT. Spiral CT and or pulmonary angiography were used to confirm PE. Suspicious VTE was defined as history or examination findings suspicious for VTE but without conclusive diagnostic imaging. Statistical analysis VTE incidence was assessed for the period between the date of the surgery and 30 days after hospital discharge. HEAD & NECK—DOI 10.1002/HED JANUARY 2013 5 THAI ET AL. The risk models were constructed using only data from the active cancer group since these patients are at greatest risk of VTE. Univariate analyses were performed for the active group using risk factors as the time-independent covariant (ie, preoperative and postoperative patient variables) and possible VTE as the time-dependent outcome. Categorical variables were analyzed using the chi-square test for independence and assessing for association with the Spearman correlation coefficient. Continuous variables were analyzed using univariate logistic regression analysis. Covariates in the analysis with a value of p < .3 were considered candidates for subsequent multivariate analysis. In the multivariate analysis, we used stepwise backward logistic regression analysis to determine the odds ratio (OR) of VTE 30 days of surgery for each qualified covariant. To assess for the strength of the multivariate model, we performed the Omnibus Tests of Model Coefficients. All analyses were performed in SPSS version 15 (SPSS Inc., Chicago, IL). A 2-tailed value of p < .05 was considered statistically significant for all analyses. RESULTS Patient characteristics, procedures, and perioperative findings There were 134 patients with head and neck cancer in the study who underwent a total of 139 procedures (prior cancer group had 26 patients in 32 cases). At the time of surgery, the average patient age was 65.4 years, and 59% were male. As shown in Table 1, the active cancer and prior cancer groups were similar in several important ways. There was no significant difference between groups with respect to age (p ¼ .78), sex (p ¼ .60), or histology (p ¼ .88). There was no difference between groups for comorbidities. There were some notable differences between the active cancer and prior cancer groups. For example, active patients with cancer were more likely to be smokers (p ¼ .14) and have diabetes mellitus (p ¼ .04). Prior patients with cancer were more likely to be on estrogen replacement therapy (p ¼ .02) and to have a prior history of radiation therapy (p .001) (Table 1). Procedures and perioperative events are summarized in Table 2. Overall operative time and free tissue transfer tourniquet time were similar between groups. The distribution of free tissue transfer donor sites was also similar. It is worthwhile to note that there were substantially more fibular osteocutaneous free tissue transfer reconstructions for the prior cancer group compared with the active cancer group (28% vs 0%). There was no significant difference in the use of intraoperative (p ¼ 1.00) or postoperative (p ¼ .76) heparin between groups. However, active patients with cancer were more likely to receive postoperative aspirin compared with prior patients with cancer (43% vs 19%, p ¼ .02). The overall complication rate, ambulation time, and length of stay were similar between the 2 groups (Table 2). The median followup for active patients with cancer was 8.4 months (range, 0.4–23.5 months). 6 HEAD & NECK—DOI 10.1002/HED JANUARY 2013 TABLE 2. Procedures and perioperative findings. Outcome Total cases, n Operative time, h Mean SD Free-tissue donor site Radial forearm Anterolateral thigh Fibula osteocutaneous Rectus musculocutaneous Latissimus dorsi musculocutaneous Jejunum Other Tourniquet time, min Mean SD Anticoagulation Intraoperative heparin Postoperative heparin Postoperative aspirin Complications Pulmonary embolism Respiratory failure Cardiac arrest Anoxic brain injury Recipient site infection Other Ambulation time, d Mean SD Length of stay, d Mean SD Active cancer Prior group cancer group p value 139 32 8.2 2.3 7.2 3.0 — .57 .61 60 (43%) 26 (19%) 15 (11%) 13 (9%) 12 (9%) 12 (38%) 5 (16%) 9 (28%) 2 (6%) 1 (3%) 6 (4%) 7 (6%) 0 3 (9%) 15.0 20.0 22.0 23.0 .12 11 (8%) 24 (17%) 60 (43%) 2 (6%) 4 (13%) 6 (19%) 1 (0.72%) 1 (0.72%) 1 (0.72%) 1 (0.72%) 7 (5%) 4 (3%) 0 0 0 0 4 (13%) 2 (6%) 15.0 20.0 22.0 23.0 10.1 10.0 10.6 7.9 1.00 .76 .02 .85 .07 .20 Abbreviation: SD, standard deviation. Possible (confirmed and suspicious) venous thromboembolism During a follow-up of 30 days, there were 2 cases of confirmed VTE, yielding a minimum incidence of 1.4% (Table 3). One patient was confirmed to have a fatal PE 2 days after discharge from the hospital. Another active patient with cancer was discovered to have a DVT; that patient was successfully treated without further sequelae. Given that a retrospective study design is likely to underestimate the true incidence of VTE, we also included suspicious cases. There were 6 cases suspicious for VTE during the 30-day follow-up period. One patient suffered from fatal sudden respiratory failure and another patient suffered from fatal sudden cardiac arrest, although an autopsy was not performed in either case. Therefore, VTE could not be excluded as the cause of death. In addition, 4 patients presented to the clinic in follow-up with unilateral lower extremity swelling reported in the electronic medical record. No further workup was ordered in these cases. Likewise, no known sequelae were documented. Two of the patients with leg swelling had received a fibula free-transfer reconstruction. However, in each of these cases the leg swelling was documented in the nonoperative leg. Therefore, a total of 8 possible VTE AFTER HEAD AND NECK CANCER SURGERY TABLE 3. VTE outcomes. Outcome Total cases, n Confirmed PE DVT Suspicious Respiratory failure Cardiac arrest Leg edema Possible total Active cancer group Prior cancer group 139 32 1 1 0 0 1 1 4 8 (5.8%) 0 0 2 2 (6.3%) Abbreviations: VTE, venous thromboembolism; PE, pulmonary embolism; DVT, deep venous thrombosis. cases (5.8%) of VTE were documented from the active cancer group (Table 3). In comparison, the prior cancer group did not have any cases of confirmed VTE (Table 3). However, 2 cases (6.3%) were identified during the 30-day follow-up periods that were suspicious for VTE. In each of these cases, new-onset unilateral leg edema was noted during the postoperative clinic visit in the nonoperative leg. These patients did not undergo further workup or empiric treatment for DVT. The rationale for this was not documented in the medical record. A Caprini risk assessment was performed retrospectively for all active cancer cases (Figure 1). The 2 patients with confirmed VTE had a mean Caprini score of 13.0 (PE patient ¼ 16, DVT patient ¼ 10). The 6 patients with suspicious VTE had a mean Caprini score of 12.8. The remaining patients with no history suggestive of VTE had a mean Caprini score of 10.5. All groups had mean scores well above the threshold to be considered at highest risk for DVT (Caprini score 5). There was no statistically significant difference in Caprini scores between groups. Univariable and multivariable analyses for active cancer group Using univariable analyses, a prior history of VTE (phi ¼ 0.40, p ¼ .0005), increased BMI (OR ¼ 1.19, p ¼ .006), and red cell transfusion (OR ¼ 1.31, p ¼ .004) were positively associated with possible (confirmed and suspicious) VTE. For patients that received anticoagulation in the postoperative period, univariable analysis showed a significant protection against possible VTE with heparin (p ¼ .041), but not with aspirin (ASA, p ¼ 1.00). However, in the multivariable analysis the protective advantage of heparin did not reach significance (p ¼ .85). Of note, the use of SCDs after surgery was not associated with reduced risk of possible VTE. The final multivariate model included length of hospital stay, age, BMI, red cell transfusion, and a prior history of VTE (Table 4). Short length of stay was associated with a slightly decreased risk of possible VTE, but this did not reach statistical significance (OR ¼ 0.89, p ¼ .15). Conversely, increased age and BMI were associated with an increased risk of possible VTE by 10% and 29%, respectively. Increased red cell transfusion was associated with an 80% increased relative risk of possible VTE (p ¼ FIGURE 1. Comparison of Caprini risk assessment scores between patients with confirmed, suspicious, and no venous thromboembolism (VTE). There was no statistically significant difference between groups. Patients with a Caprini score 5 (represented by the dotted line) are considered to be at highest risk for deep venous thrombosis (DVT). .009). The factor most strongly associated with possible VTE was a prior history of VTE, which increased the relative risk 25-fold (p ¼ .041). DISCUSSION Risk factors for VTE are well known and include primary site of tumor, comorbid conditions (obesity, infection, pulmonary disease, renal disease), older age, immobilization, previous history of VTE, active chemotherapy or hormonal therapy, and recent major surgical intervention.6,15 Patients with cancer undergoing surgery are considered to be at greatest risk of VTE and a significant proportion of patients with cancer undergoing surgery are affected by VTE. It has been estimated that patients with cancer undergoing surgery have a 2-fold increase in postoperative DVT and a 3-fold increase in fatal PE compared with patients without cancer who undergo similar operations.16,17 The most effective methods for preventing VTE are also well known and include early ambulation, mechanical compression devices, and pharmacologic thromboprophylaxis. There is an increasing national imperative to better address the risk of VTE among patients with cancer undergoing surgery. This is reflected in recent guidelines from the American College of Chest Physicians (ACCP) and the American Society of Clinical Oncology (ASCO), recommending that patients with cancer undergoing surgery receive medical prophylaxis for up to 1 month after surgery.5,6,15 For patients with cancer who are undergoing major surgery, ACCP recommendations include routine TABLE 4. Multivariant analysis for active cancer group Variable Odds ratio Length of stay Age BMI Red cell transfusion VTE (prior) 0.89 1.10 1.29 1.80 25.11 95% CI p value 0.75–1.04 1.00–1.19 1.05–1.58 1.16–2.79 1.13–556.39 .15 .046 .015 .009 .041 Abbreviations: CI, confidence interval; BMI, body mass index; VTE, venous thromboembolism. HEAD & NECK—DOI 10.1002/HED JANUARY 2013 7 THAI ET AL. thromboprophylaxis with low-molecular-weight heparin (LMWH) or fondaparinux. For patients with cancer with additional risk for VTE (eg, history of VTE, advanced age) the recommendation is to use LMWH or fondaparinux in combination with mechanical methods such as SCDs. Aspirin alone is not recommended for thromboprophylaxis in any patient groups. Similarly, ASCO recommendations suggest that all patients with cancer undergoing major surgical intervention for malignant disease be considered for thromboprophylaxis with pharmacologic and optional mechanical methods, reserving the former only if there is risk of active bleeding. There are many studies that investigate the risk of VTE after surgery for patients with colon, prostate, and breast cancer.1,4,6,8 Yet, there are scant data regarding the risk of VTE for patients with head and neck cancer undergoing surgery. A prior large retrospective study that included all otolaryngologic procedures performed at a single institution showed a very low incidence of VTE (0.3%). The incidence of VTE in that study was 0.6% for patients with head and neck cancer.18 Another similar retrospective study of general otolaryngology patients showed an incidence of 0.15%.19 It is speculated by some that patients with head and neck cancer may be at low risk of VTE after surgery because of the relatively superficial nature of dissection and postoperative early ambulation compared with other oncologic procedures. There is also a concern that routine prophylactic anticoagulation will increase the risk of postoperative hematoma, which can compromise flap viability. Thus, currently few head and neck surgeons routinely prescribe anticoagulation after resection and microvascular reconstruction despite national guidelines for patients with general oncologic surgery. The most robust data to date regarding the risk of VTE among patients with head and neck cancer undergoing extensive resection and reconstruction were presented by Chen and colleagues.20 In that study, the authors compared symptomatic VTE and PE incidence after oncologic surgery with reconstruction for patients with head and neck cancer to patients with non–head and neck cancer. They found that the incidence of symptomatic VTE or PE was low (0.75%). Interestingly, they reported that the incidence of symptomatic VTE was greater for patients with head and neck cancer (0.31% DVT, 0.44% PE) than that for patients with non–head and neck cancer (0.008% DVT, 0.09% PE). It is worth noting that all patients in the study received routine LMWH for VTE prophylaxis. Current methods to risk-stratify patients with head and neck cancer for possible VTE are imperfect. The most widely used risk assessment tool was developed by Caprini.14 The Caprini risk assessment tool was first used nearly 30 years ago and has been updated periodically since then. With this model, approximately 40 risk factors are listed, with weights of 1 to 5 points each. The total risk factor score is then used to group patients into 1 of 4 categories (low, moderate, high, and highest risk), each with a recommended prophylactic regimen. The Caprini risk assessment tool has been validated in retrospective studies for use in patients needing elective general surgery and modified for use in patients needing plastic surgery.21 Most recently, it has been correlated with proven 30-day VTE incidence in a prospective study of 1470 8 HEAD & NECK—DOI 10.1002/HED JANUARY 2013 general surgery patients.22 In our study, a Caprini risk assessment was performed retrospectively for all active cancer cases. In accord with our inclusion criteria, all patients included in this study were classified at highest risk of DVT by a Caprini risk assessment (score 5). We found no significant difference in mean Caprini scores between patients classified as confirmed, suspicious, or no VTE (Figure 1). Therefore, the Caprini risk assessment tool was unable to accurately risk-stratify our patients. To our knowledge this is the only study to evaluate the use of the Caprini risk assessment tool specifically in patients with head and neck cancer after resection and microvascular reconstruction. It is possible that our sample size was too small for the model to discriminate between VTE and non-VTE patients. Therefore, the clinical utility of the Caprini risk assessment tool for patients with head and neck cancer having surgery has yet to be fully elucidated. In this study, we aimed to better define the incidence of VTE in patients with head and neck cancer after resection and microvascular reconstruction. It was postulated that these patients would be at greatest risk of VTE because of the increased length of surgery and hospitalization and the lack of routine anticoagulation. We found that 5.8% of our patients with active cancer developed a possible (confirmed and suspicious) VTE. It is important to note that only 2 cases (1.4%) with active cancer were proven radiographically, and therefore classified as confirmed VTE. The majority of possible VTE cases were classified as suspicious because imaging confirmation was not available. For example, 2 patients died outside of the hospital from sudden respiratory failure or sudden cardiac arrest within 30 days of surgery and were classified as suspicious VTE. We speculated that there could be a difference between patients with active cancer and patients with prior cancer with respect to risk of VTE. Therefore, we compared the groups for baseline differences and VTE outcome. Despite differences between groups, including baseline smoking status, estrogen use, and postoperative aspirin use, the rate of possible VTE was similar for patients with active cancer and prior cancer. Three patients in our study died as a direct result of a possible VTE. It is interesting that all of these cases occurred in the active cancer group. Our findings suggest that the incidence of VTE among patients with head and neck cancer after resection and microvascular reconstruction may be higher than previously reported. Even if we excluded suspicious cases, our confirmed VTE incidence of 1.4% is still above the range of incidences previously reported for head and neck cancer.18–20 The clinical significance of this finding is yet to be determined, especially since the patients included in our study did not receive routine anticoagulation. Our confirmed VTE incidence is lower than the incidence reported for most patients who had non–head and neck oncologic surgery, where prophylaxis is routinely used. For example, the incidence of VTE has been reported to be 2.8% in general surgery, 2.0% in gynecologic surgery, and 0.87% in urologic surgery.4 These relatively low VTE incidences were achieved in the setting of routine use of perioperative LMWH, including nearly a third of study patients receiving postdischarge prophylaxis. VTE In this study we also aimed to identify potential risk factors for developing VTE for patients with head and neck cancer. We found increased age, increased BMI, red cell transfusion, and prior history of VTE to be significant predictors of possible VTE on multivariate analyses. Of these, a prior history of VTE showed the greatest risk (25-fold). Our results appear in line with the identified risk factors identified in other studies.4,6,11 For example, prior history of VTE is a well-known risk factor for subsequent VTE because many of the factors that contribute to VTE are chronic in nature. Recurrence of VTE is greatest within the first few months after a thrombotic episode, but has been reported to be as high as 22% over 5 years.23 Patients with VTE are at increased risk of recurrence and death after treatment.24 Therefore, the importance of prior VTE in risk-stratifying patients cannot be overstated. Interestingly, we found red cell transfusion to be associated with possible VTE for patients with head and neck cancer undergoing surgery. Although red cell transfusion is not included in many VTE risk factor assessments, it has been associated with increased risk of VTE after resection of colorectal cancer.25 There are limitations to the current study. We took great effort to carefully review the medical record notes to identify classic symptoms of DVT in our patients in the perioperative period. However, our results depend on the accuracy of the medical records. Thus, there is the potential for recall bias. Patients with subclinical DVT were not identified. Only patients who were symptomatic and hospitalized were investigated with imaging. Therefore, it is possible that our results are an underestimation of the true VTE incidence. Autopsy studies have demonstrated that the incidence of VTE in patients with cancer can be as high as 50%, with clinically confirmed cases ranging between 4% and 20%.26 We included suspicious VTE cases into our analysis to partially account for this possibility. It is possible that our decision to include suspicious cases overestimates the true incidence. Therefore, we have presented the data as a range, to provide the best estimate of the true incidence of VTE in our cohort. There are 2 possible interpretations of our findings: (1) the true incidence of VTE among patients with head and neck cancer surgery is low even without prophylactic anticoagulation or (2) the true incidence of VTE among patients with head and neck cancer surgery is underestimated. Our findings suggest that a retrospective study design is inadequate to accurately define the true incidence of VTE among patients with head and neck cancer having surgery. We report an incidence that ranges from a minimum of 1.4% (confirmed VTE) to a maximum of 5.8% (confirmed and suspicious VTE). Thus, our data are not compelling enough at this point to modify our current VTE prophylaxis strategies. We cannot recommend routine VTE prophylaxis with LWMH without further investigation to characterize the risk:benefit ratio, especially in the context of microvascular reconstruction. AFTER HEAD AND NECK CANCER SURGERY Therefore, we have initiated a prospective observational study to elucidate a more accurate VTE incidence among patients with head and neck cancer after surgery. REFERENCES 1. Behranwala KA, Williamson RC. Cancer-associated venous thrombosis in the surgical setting. Ann Surg 2009;249:366–375. 2. Lee AY. Epidemiology and management of venous thromboembolism in patients with cancer. Thromb Res 2003;110:167–172. 3. Prandoni P, Piccioli A, Girolami A. Cancer and venous thromboembolism: an overview. Haematologica 1999;84:437–445. 4. Agnelli G, Bolis G, Capussotti L, et al. A clinical outcome-based prospective study on venous thromboembolism after cancer surgery: the @RISTOS Project. Ann Surg 2006;243:89–95. 5. Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008;133:381S–453S. 6. Lyman GH, Khorana AA, Falanga A, et al. American Society of Clinical Oncology guideline: recommendations for venous thromboembolism prophylaxis and treatment in patients with cancer. J Clin Oncol 2007;25: 5490–5505. 7. Blom JW, Doggen CJ, Osanto S, Rosendaal FR. Malignancies, prothrombotic mutations, and the risk of venous thrombosis. J Am Med Assoc 2005; 293:715–722. 8. Chew HK, Wun T, Harvey D, Zhou H, White RH. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med 2006;166:458–464. 9. Sallah S, Wan JY, Nguyen NP. Venous thrombosis in patients with solid tumors: determination of frequency and characteristics. Thromb Haemost 2002;87:575–579. 10. Reeves D, Liu CY. Retrospective evaluation of venous thromboembolism prophylaxis in the adult cancer population. J Oncol Pharm Pract 2010;16: 27–31. 11. Sousou T, Khorana AA. New insights into cancer-associated thrombosis. Arterioscler Thromb Vasc Biol 2009;29:316–320. 12. Sud R, Khorana AA. Cancer-associated thrombosis: risk factors, candidate biomarkers and a risk model. Thromb Res 2009;123 (Suppl 4):S18–S21. 13. White RH, Zhou H, Gage BF. Effect of age on the incidence of venous thromboembolism after major surgery. J Thromb Haemost 2004;2: 1327–1333. 14. Caprini JA. Risk assessment as a guide for the prevention of the many faces of venous thromboembolism. Am J Surg 2010;199:S3–S10. 15. Mandala M, Falanga A, Roila F. Venous thromboembolism in cancer patients: ESMO Clinical Practice Guidelines for the management. Ann Oncol 2010;21 (Suppl 5):v274–v276. 16. Gallus AS. Prevention of post-operative deep leg vein thrombosis in patients with cancer. Thromb Haemost 1997;78:126–132. 17. Huber O, Bounameaux H, Borst F, Rohner A. Postoperative pulmonary embolism after hospital discharge. An underestimated risk. Arch Surg 1992;127:310–313. 18. Moreano EH, Hutchison JL, McCulloch TM, et al. Incidence of deep venous thrombosis and pulmonary embolism in otolaryngology–head and neck surgery. Otolaryngol Head Neck Surg 1998;118:777–784. 19. Lee J, Alexander A, Higgins K, Geerts W. The Sunnybrook experience: review of deep vein thrombosis and pulmonary embolism in otolaryngology. J Otolaryngol Head Neck Surg 2008;37:547–551. 20. Chen CM, Disa JJ, Cordeiro PG, et al. The incidence of venous thromboembolism after oncologic head and neck reconstruction. Ann Plast Surg 2008;60:476–479. 21. Davison SP, Venturi ML, Attinger CE, Baker SB, Spear SL. Prevention of venous thromboembolism in the plastic surgery patient. Plast Reconstr Surg 2004;114:43E–51E. 22. Bahl V, Hu HM, Henke PK, et al. A validation study of a retrospective venous thromboembolism risk scoring method. Ann Surg 2010;251:344–350. 23. Hansson PO, Sorbo J, Eriksson H. Recurrent venous thromboembolism after deep vein thrombosis: incidence and risk factors. Arch Intern Med 2000;160:769–774. 24. Andresen MS, Sandven I, Brunborg C, et al. Mortality and recurrence after treatment of VTE: long term follow-up of patients with good life-expectancy. Thrombosis Res 2011;127:540–546. 25. Nilsson KR, Berenholtz SM, Garrett-Mayer E, et al. Association between venous thromboembolism and perioperative allogeneic transfusion. Arch Surg 2007;142:126–132. 26. Gomes MP, Deitcher SR. Diagnosis of venous thromboembolic disease in cancer patients. Oncology (Williston Park) 2003;17: 126–135, 139. HEAD & NECK—DOI 10.1002/HED JANUARY 2013 9