Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
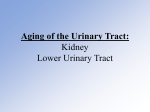
Am J Physiol Heart Circ Physiol 287: H2834 –H2839, 2004. First published August 19, 2004; doi:10.1152/ajpheart.00394.2004. Renal blood flow in heart failure patients during exercise Afsana Momen,1 Douglas Bower,1 John Boehmer,1 Allen R. Kunselman,2 Urs A. Leuenberger,1 and Lawrence I. Sinoway1,3 1 Division of Cardiology, Department of Medicine, and 2Department of Health Evaluation Sciences, Pennsylvania State University College of Medicine, Milton S. Hershey Medical Center, Hershey 17033; and 3Lebanon Veterans Administration Medical Center, Lebanon, Pennsylvania 17042 Submitted 27 April 2004; accepted in final form 16 August 2004 leads to increases in heart rate (HR), blood pressure (BP), ventilation, and peripheral vasoconstriction. Renal vasoconstriction occurs during exercise in humans (16, 19) as a result of increased sympathetic outflow. This reflex renal vasoconstriction acts to maintain BP as well as to redistribute blood flow toward metabolically active skeletal muscle. A recent study from this laboratory observed reflex renal vasoconstriction during forearm exercise. Furthermore, these experiments suggested that the renal vasoconstriction was due primarily to engagement of mechanically sensitive afferents in the contracting skeletal muscle (19). Reduced exercise capacity and sympathoexcitation are cardinal features of congestive heart failure (HF). Primary mechanisms responsible for early fatigability during exercise in HF patients are thought to be due to diminished perfusion in active skeletal muscle due to reduced blood flow and/or to abnormal muscle metabolism in HF patients (12, 17, 30, 31). This mismatch between metabolic demand and muscle perfusion can engage the muscle reflex evoking sympathoexcitation (25). Resting sympathetic activity is increased in HF patients (8). Although a wealth of information has been obtained regarding the sympathetic neural responses to exercise in HF, far fewer studies have been designed to determine the mechanisms responsible for sympathetically mediated vasoconstriction during exercise in this disease. Studies using a rhythmic handgrip (HG) protocol demonstrated increased BP (21, 27) and muscle sympathetic nerve activity (MSNA) in HF patients due to increased metaboreflex activation. In contrast, Sterns et al. (29), using a static exercise paradigm, found attenuated metaboreflex-mediated increases in MSNA in HF. In the latter study, it was speculated that the metaboreflex was desensitized in HF. It was also suggested in this report that some other neural mechanism was preferentially engaged during exercise in HF so that the “overall” sympathetic response to exercise was preserved. Later, in a study utilizing limb congestion to preferentially engage mechanically sensitive muscle afferents, McClain et al. (14) documented that enhanced MSNA during static HG exercise could be caused by increased muscle mechanoreflex stimulation. Two separate reports using different exercise paradigms found that renal blood flow falls to a greater extent in HF subjects than in controls (15, 23). Middlekauff et al. (15), using the positron emission tomography (PET) scan method, found that rhythmic HG led to a greater increase in renal vascular resistance (RVR) in HF than in controls. Because of the limited time resolution of this method, the investigators were unable to determine the neural mechanisms responsible for the greater vasoconstrictor response in HF. The lack of time resolution of the PET method prevents a careful evaluation of the time course of responses within the first few seconds after exercise is initiated. This is particularly important because central command and the muscle mechanoreflex become engaged within a few seconds of the onset and initiation of contraction (4, 9, 26). Middlekauff et al. (15) also found sustained increases in RVR in HF during a 2- to 3-min recovery period. The explanation for this finding was not clear, although activation of humoral systems could not be excluded. Accordingly, we designed a study in which renal blood flow velocity (RBV) in HF subjects and controls was evaluated with the Doppler ultrasound technique (Duplex ultrasound). We reasoned that because of its excellent temporal resolution, this technique would allow us to examine the role of these putative neural mechanisms in controlling renal blood flow during Address for reprint requests and other correspondence: L. I. Sinoway, Cardiology, H047, Pennsylvania State College of Medicine, PO Box 850, Hershey, PA 17033 (E-mail: [email protected]). The costs of publication of this article were defrayed in part by the payment of page charges. The article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. kidney; nervous system; sympathetic; vasoconstriction EXERCISE H2834 http://www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.32.247 on June 18, 2017 Momen, Afsana, Douglas Bower, John Boehmer, Allen R. Kunselman, Urs A. Leuenberger, and Lawrence I. Sinoway. Renal blood flow in heart failure patients during exercise. Am J Physiol Heart Circ Physiol 287: H2834 –H2839, 2004. First published August 19, 2004; doi:10.1152/ajpheart.00394.2004.—During exercise, reflex renal vasoconstriction maintains blood pressure and helps in redistributing blood flow to the contracting muscle. Exercise intolerance in heart failure (HF) is thought to involve diminished perfusion in active muscle. We studied the temporal relationship between static handgrip (HG) and renal blood flow velocity (RBV; duplex ultrasound) in 10 HF and in 9 matched controls during 3 muscle contraction paradigms. Fatiguing HG (protocol 1) at 40% of maximum voluntary contraction led to a greater reduction in RBV in HF compared with controls (group main effect: P ⬍ 0.05). The reduction in RBV early in HG tended to be more prominent during the early phases of protocol 1. Similar RBV was observed in the two groups during post-HG circulatory arrest (isolating muscle metaboreflex). Short bouts (15 s) of HG at graded intensities (protocol 2; engages muscle mechanoreflex and/or central command) led to greater reductions in RBV in HF than controls (P ⬍ 0.03). Protocol 3, voluntary and involuntary biceps contraction (eliminates central command), led to similar increases in renal vasoconstriction in HF (n ⫽ 4). Greater reductions in RBV were found in HF than in controls during the early phases of exercise. This effect was not likely due to a metaboreflex or central command. Thus our data suggest that muscle mechanoreflex activity is enhanced in HF and serves to vigorously vasoconstrict the kidney. We believe this compensatory mechanism helps preserve blood flow to exercising muscle in HF. H2835 HEART FAILURE, RENAL BLOOD FLOW, AND HANDGRIP Table 1. Resting data in HF and control groups Protocol 1 MVC, kg HR, beats/min MAP, mmHg Renal blood flow velocity, cm/s RVR, units Protocol 2 HF Control P value HF Control P value 27⫾3 73⫾5 87⫾4 42.9⫾4.3 2.2⫾0.3 36⫾3 57⫾3 94⫾2 47.4⫾2.9 2.0⫾0.1 ⬍0.036 ⬍0.010 NS NS NS 27⫾3 74⫾5 85⫾4 46.3⫾5.0 2.0⫾0.2 36⫾3 57⫾3 87⫾3 52.4⫾4.4 1.8⫾0.2 ⬍0.036 ⬍0.011 NS NS NS Data are expressed as means ⫾ SE. HF, heart failure; MVC, maximum voluntary contraction; HR, heart rate; MAP, mean arterial pressure; RVR, renal vascular resistance; NS, not significant. Protocol 1 is from 40% static to fatigue; protocol 2 is graded handgrip. Statistics reflect unpaired t-test comparing between HF and control groups. METHODS Study Population A group of 10 HF patients (7 men and 3 women, age 56 ⫾ 4 yr, mean body mass index 27 ⫾ 1 kg/m2) and 9 healthy volunteers (7 men and 2 women, age 56 ⫾ 5 yr, mean body mass index 24 ⫾ 1 kg/m2) were studied. Each subject signed an informed written consent, and a physical examination was performed. The study protocols were approved by the Institutional Review Board of the Milton S. Hershey Medical Center. The healthy volunteers previously studied in this laboratory were age and sex matched to the HF patients. The healthy control volunteers were normotensive nonsmokers who were not receiving medications (18). HF patients were recruited from the Cardiovascular Clinic at The Hershey Medical Center. Five were New York Heart Association class II, 4 were class III, and 1 was class IV. The causes of HF were either ischemic (n ⫽ 3) or idiopathic cardiomyopathy (n ⫽ 7). All HF patients were clinically stable. Medications include the following: -blockers (n ⫽ 9), digoxin (n ⫽ 7), angiotensin-converting enzyme inhibitors (n ⫽ 8), diuretics (n ⫽ 7), and nitrates (n ⫽ 3). Two of the HF patients had insulin-dependent diabetes. Medications were withheld on the morning of the study. Renal Blood Flow Velocity All subjects were studied in the post absorptive state. Duplex ultrasound (HDI 5000, ATL Ultrasound; Bothell, WA) was used to determine renal blood flow dynamics. The renal artery was scanned using the anterior abdominal approach while the subject was supine. A curved-array transducer (2–5 MHz) with a 2.5-MHz pulsed Doppler frequency was used. The probe insonation angle to the renal artery was ⬍60° with the focal zone set at the renal artery depth. To obtain optimum velocity tracings, the transducer was held in a constant position, and the data were obtained in the same phase of the respiratory cycle of the respective subject. Care was taken to ensure that the subject did not perform Valsalva maneuvers during HG. The Doppler tracings were analyzed using ATL software (HDI 5000) to obtain mean velocity. Each velocity measurement was normalized to a time constant of 1 s. Subsequently, the RVR index was calculated by dividing mean arterial pressure by RBV (in cm/s). RVR is expressed in arbitrary units. HR (electrocardiogram) and BP (Finapres, Ohmeda; Madison, WI) were also obtained continuously throughout the protocols. Resting BP was determined with an automated sphygmomanometer (Dinamap, Critikon; Tampa, FL). Study Protocols Protocol 1: fatiguing static exercise followed by post-HG circulatory arrest. The maximum voluntary contraction (MVC) of the nondominant arm was determined in each subject. Baseline HR, mean arterial pressure (MAP), and RBV were obtained over 5 min before each protocol. HG was performed at 40% MVC until fatigue. Immediately before the subject’s point of fatigue, a forearm cuff was inflated to 250 mmHg for 2 min [post-HG circulatory arrest (PHGCA)]. At the end of exercise, each subject rated their effort level as 20 (Borg scale) (1). Protocol 2: static HG exercise at graded intensity. Five minutes of baseline HR, MAP, and RBV were collected. Each subject then Fig. 1. A: percent change data in renal blood flow velocity (y-axis) as a function of percent time to fatigue (x-axis) during static handgrip at 40% maximum voluntary contraction. Data are presented as means ⫾ SE. B: comparison between baseline and posthandgrip circulatory arrest (PHG-CA) renal blood flow velocity in heart failure (HF) and control groups. P values reflect statistical analysis using two-way ANOVA comparing between HF (F, n ⫽ 10) and control subjects (E, n ⫽ 9). Note the significant greater reduction in renal blood flow velocity in HF than in controls during fatiguing handgrip exercise. AJP-Heart Circ Physiol • VOL 287 • DECEMBER 2004 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.32.247 on June 18, 2017 exercise. This method allows subjects to perform multiple exercise paradigms on the same day (19). Because technically it is presently impossible to obtain direct measurements of renal sympathetic nerve activity in humans during exercise, RBV and RVR index (calculated) are used as surrogate for renal sympathetic nerve activity. The results of these studies suggest that renal blood flow falls to a greater degree during exercise in HF than in controls. Moreover, this effect is seen within the first few seconds of exercise. The results of these studies indicate that muscle mechanoreflex activity is augmented in congestive HF. H2836 HEART FAILURE, RENAL BLOOD FLOW, AND HANDGRIP Table 2. Protocol 1 data for HR, MAP, and resistance 10% 20% 40% 60% 80% 100% HF Control HF Control HF Control HF Control HF Control HF Control Statistics P ⌬%HR 6.9⫾2.0 8.3⫾1.3 7.6⫾2.5 8.5⫾1.7 9.4⫾2.8 15.3⫾1.4 14.3⫾3.1 18.9⫾2.1 14.2⫾4.1 21.2⫾2.5 14.7⫾3.7 24.8⫾3.1 ⌬%MAP 7.9⫾3.1 5.2⫾1.8 6.7⫾2.6 11.4⫾2.4 9.4⫾2.8 17.6⫾2.5 14.2⫾3.5 25.1⫾3.4 15.4⫾3.9 33.7⫾4.6* 20.3⫾4.3 34.9⫾4.5* ⌬%RVR 34.7⫾9.1 13.6⫾5.3 33.7⫾5.2 25.2⫾5.0 35.6⫾6.1 29.0⫾7.3 48.5⫾5.7 46.4⫾10.1 50.2⫾6.7 60.7⫾15.6 65.1⫾9.4 77.3 ⫾14.8 Group Paradigm Interaction Group Paradigm Interaction Group Paradigm Interaction NS ⬍0.001 NS ⬍0.091 ⬍0.001 ⬍0.005 NS ⬍0.001 NS Data are expressed as means ⫾ SE. Data (%change from respective baseline) from fatiguing static handgrip protocol for HR, MAP, and RVR are shown. Statistics reflect two-way ANOVA comparing between HF (n ⫽ 10) and control groups (n ⫽ 9). *P ⬍ 0.05. Data Analysis and Statistics Values were averaged over a 5-min rest period before each paradigm. In the fatiguing static HG protocol, variables were measured at 10%, 20%, 40%, 60%, 80%, and 100% (peak) of the respective subject’s time to exhaustion. Data from the last 15 s of PHG-CA was used in the statistical analyses. In the second protocol, data were analyzed in 5-s time periods. Statistical analyses were performed separately on each 5-s period (i.e., 1–5, 6 –10, and 11–15 s). Data are presented as mean ⫾ SE. Resting values in HF and controls were compared with unpaired t-tests. For the voluntary and involuntary biceps contraction protocol, repeated-measures one-way ANOVA models, having a first-order autoregressive variance-covariance structure to account for the within-subject correlation, were fit to the data to compare response variables to baseline in the HF group using Dunnett’s test in the post hoc analysis to control type I error. Repeated-measures two-way ANOVA models, having a first-order autoregressive variance-covariance structure to account for the with- in-subject correlation, were fit to the data for each response variable to assess the two main effects of group (between HF and healthy subjects) and HG paradigm and the possible interaction of these two effects. A Bonferroni correction to control type I error for multiple comparisons was applied to the tests of simple effects at respective time periods during the contraction paradigms when HF was compared with healthy controls. P ⬍ 0.05 was considered significant. All analyses were performed with the SAS statistical software package (SAS Institute; Cary, NC). RESULTS At rest, HR was greater in HF than controls (P ⬍ 0.05; Table 1). MVC was lower in HF than in controls (P ⬍ 0.05; Table 2). However, no significant differences were found with regards to age, sex, and body mass index [P ⫽ not significant (NS)]. Protocol 1: Fatiguing Static HG Followed by PHG-CA The time to fatigue was not different in the two groups (HF, 103 ⫾ 3 s, n ⫽ 10, vs. controls, 134 ⫾ 12 s, n ⫽ 9; P ⫽ (NS). RBV fell more during fatiguing HG in the HF group than in the controls (group main effect, 0.037; Fig. 1A). The magnitude of increases in MAP tended to be smaller in HF than in controls. This effect seemed most pronounced toward the end of exercise (Table 2). Thus, despite a greater fall in RBV in HF, RVR was similar in the two groups (Table 2). During PHG-CA, resistances (paradigm effect, P ⬍ 0.002) and RBV responses were similar in the two groups (Table 3 and Fig. 1B). Table 3. Minute 2 of PHG-CA during protocol 1 HF Control Baseline PHG-CA Baseline PHG-CA Statistics P HR, beats/min 72.9⫾4.7 77.0⫾5.3 56.9⫾2.7* 58.7⫾2.9* MAP, mmHg 87.0⫾4.0 99.4⫾3.3 93.6⫾1.9 115.7⫾3.7* 2.2⫾0.3 3.0⫾0.5 2.0⫾0.1 2.9⫾0.4 Group Paradigm Interaction Group Paradigm Interaction Group Paradigm Interaction ⬍0.009 ⬍0.065 NS ⬍0.017 ⬍0.001 ⬍0.033 NS ⬍0.002 NS RVR, mmHg䡠cm⫺1䡠s⫺1 Data are expressed as means ⫾ SE. Posthandgrip circulatory arrest (PHG-CA) data (the last 15 s) for HR, MAP, and RVR responses are shown. Statistics reflect two-way ANOVA comparing between HF and control groups. *P ⬍ 0.05, comparison between HF and control groups using two-way ANOVA on corresponding HR, MAP, and RVR values. AJP-Heart Circ Physiol • VOL 287 • DECEMBER 2004 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.32.247 on June 18, 2017 performed 15 s bouts of static HG at 10%, 30%, 50%, and 70% MVC. The same sequence was maintained in all subjects with a 1-min period of rest between bouts. Protocol 3: involuntary and voluntary biceps contraction. Percutaneous electrical stimulation was utilized to induce involuntary biceps contraction. Electrical pads (5 ⫻ 5 cm2) were placed ⬃3 cm apart, and the biceps muscle was electrically stimulated (200 V; phase duration, 0.3 ms; phase interval, 0.1 ms). Electrical biceps contraction evoked ⬃15–30% of MVC and was sustained for ⬃15 s without eliciting pain. The subjects then performed 15 s of voluntary biceps contractions at the same tension that had been generated during involuntary contraction. H2837 HEART FAILURE, RENAL BLOOD FLOW, AND HANDGRIP Table 4. Data from Protocol 2 Graded Protocol in HF Group 10% Graded Protocol in Control Group 50% 70% 10% 30% 50% 70% 1.2⫾1.1 4.5⫾1.7 3.3⫾1.3 6.5⫾3.6 1.0⫾1.8 2.9⫾1.5 4.9⫾2.0 7.4⫾2.2 MAP 4.8⫾1.3 4.8⫾1.9 7.7⫾2.1 6.1⫾3.1 4.4⫾1.4 8.5⫾1.7 10.0⫾2.1 14.0⫾2.0* RVR 13.7⫾4.1 22.2⫾6.1 24.8⫾6.7 25.2⫾6.7 4.6⫾2.4 4.8⫾3.8 11.3⫾4.0 14.3⫾6.0 1.7⫾1.0 3.0⫾2.5 3.2⫾3.3 9.6⫾4.0 1.2⫾1.5 1.3⫾1.4 8.0⫾2.7 11.5⫾3.7 MAP 5.3⫾1.3 8.2⫾2.4 8.6⫾2.4 10.9⫾3.0 2.5⫾1.5 8.2⫾1.6 16.1⫾2.3 19.1⫾3.9 RVR 13.5⫾2.9 22.0⫾5.6 27.6⫾5.0 40.1⫾12.0 2.8⫾2.9 10.5⫾5.5 22.1⫾4.1 29.8⫾9.5 11–15 s HR ⫺1.2⫾2.8 4.7⫾2.0 1.0⫾4.3 10.3⫾4.2 2.4⫾1.7 3.1⫾1.9 12.1⫾3.2 15.4⫾3.9 MAP 3.9⫾1.1 7.6⫾2.1 6.8⫾2.8 10.6⫾2.7 2.0⫾1.7 7.9⫾1.4 15.8⫾2.5* 21.1⫾4.3* RVR 14.4⫾2.2 21.5⫾5.7 26.6⫾5.2 43.7⫾7.5 4.7⫾2.7 9.5⫾4.6 26.4⫾6.7 34.1⫾13.9 0–5 s HR 6–10 s HR P Value (2-way ANOVA) Group Paradigm Interaction Group Paradigm Interaction Group Paradigm Interaction NS ⬍0.020 NS NS ⬍0.039 ⬍0.064 ⬍0.015 NS NS Group Paradigm Interaction Group Paradigm Interaction Group Paradigm Interaction NS ⬍0.002 NS NS ⬍0.001 ⬍0.015 NS ⬍0.003 NS Group Paradigm Interaction Group Paradigm Interaction Group Paradigm Interaction NS ⬍0.002 ⬍0.043 NS ⬍0.001 ⬍0.012 NS ⬍0.001 NS Data are expressed as mean ⫾ SE. Graded handgrip protocol data (%change from respective baseline value) for HR, MAP and RVR are shown. *P ⬍ 0.05, comparison between HF (n ⫽ 10) and control groups (n ⫽ 9) using two-way ANOVA on HR, MAP, and RVR responses to handgrip. Protocol 2: Static HG Exercise at Graded Intensities The data for RVR, HR, and MAP are shown in Table 4. Increases in RVR were found in both HF (n ⫽ 10) and control (n ⫽ 9) groups during short bouts of hardgrip (Table 4). Larger RBV reductions were found in HF than in controls (Fig. 2). Although no group difference was observed in MAP responses, smaller MAP responses in HF were seen at the higher workloads during 0 –5 and 11–15 s of HG exercise (P ⬍ 0.05; Table 4). Protocol 3: Involuntary Versus Voluntary Biceps Contraction Involuntary and voluntary biceps contraction evoked RVR responses in HF (n ⫽ 4, one-way ANOVA, P ⫽ 0.036). Increases in RVR were similar, 19 ⫾ 5% and 25 ⫾ 6% (P ⫽ NS), during involuntary and voluntary biceps contraction, respectively. DISCUSSION The major finding in this report was that HF patients compared with healthy controls had greater renal blood flow reductions during the early phase of static exercise. These studies provide evidence that the muscle mechanoreflex plays a crucial role in regulating renal blood flow during exercise in HF. Resting RBV, RVR, and MAP were not different in the HF patients and control subjects. A prior report also suggests that baseline renal norepinephrine (NE) spillover is similar in HF Fig. 2. Percent change data in renal blood flow velocity (y-axis) during 15-s bouts of static handgrip at 10, 30, 50, and 70% maximum voluntary contraction (x-axis) in HF (F, n ⫽ 10) and control (E, n ⫽ 9) groups. Data are presented as means ⫾ SE. Data were examined separately for 0 –5 (A), 6 –10 (B), and 11–15 (C) s. P values reflect statistical analysis using two-way ANOVA (Bonferroni corrected) comparing between HF and control subjects. *Significant differences between HF and control subjects at a respective point. Note the significant greater reduction in renal blood flow velocity in HF than in controls in each 5-s time period of exercise. AJP-Heart Circ Physiol • VOL 287 • DECEMBER 2004 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.32.247 on June 18, 2017 30% H2838 HEART FAILURE, RENAL BLOOD FLOW, AND HANDGRIP AJP-Heart Circ Physiol • VOL in renal blood flow were seen at lower stimulus frequency in HF than were observed in normal control rats. These results suggest that vascular sensitivity may be heightened in HF. We doubt that this explains our results because if this were the explanation, we would have expected to see a greater reduction in renal blood flow during PHG-CA in HF. Clinical Implications We speculate that exaggerated renal blood flow reduction observed in HF patients in the present study represents a compensatory mechanism that maintains blood flow to exercising muscle in the face of diminished levels of cardiac output. Our data further suggest that this renal blood flow response was predominantly due to local factors within contracting muscles and not to local renal factors (20). Prior animal studies have documented that the muscle mechanoreflex can be sensitized by metabolic byproducts of muscle contraction such as ATP (10) and lactic acid (22, 28), etc. Enhanced lactate production due to abnormal skeletal muscle metabolism is found in HF patients during exercise (13, 25). Furthermore, in this laboratory, pilot studies using an animal model of HF have observed increased ATP production in HF rats during muscle stretch (unpublished observation). Because the response was seen early in the present study, and central command did not appear to be a major factor, we conclude that the early large reduction in renal blood flow in HF was due to an accentuated muscle mechanoreflex response in HF patients. ACKNOWLEDGMENTS The authors are grateful to Jennifer Stoner for expert manuscript preparation, Brian Handly, Shelly Silber, and Kristen Gray for technical support, and the staff of the General Clinical Research Center. GRANTS The study was supported by National Institutes of Health Grants R01 AG-012227 (to L. I. Sinoway), R01 HL-070222 (to L. I. Sinoway), K24 HL-004011 (to L. I. Sinoway), P01 HL-077670 (to L. I. Sinoway), R01 HL-068699 (to U. A. Leuenberger), M01 RR-010732, and C06 RR-016499. REFERENCES 1. Borg GAV. Psychophysical bases of perceived exertion. Med Sci Sports Exerc 14: 377–381, 1982. 2. DiBona GF and Sawin LL. Frequency response of the renal vasculature in congestive heart failure. Circulation 107: 2159 –2164, 2003. 3. Gullestad L, Manhenke C, Aarsland T, Skardal R, Fagertun H, Wikstrand J, and Kjekshus J. Effect of metoprolol CR/XL on exercise tolerance in chronic heart failure - a substudy to the MERIT-HF trial. Eur J Heart Fail 3: 463– 468, 2001. 4. Herr MD, Imadojemu V, Kunselman AR, and Sinoway LI. Characteristics of the muscle mechanoreflex during quadriceps contractions in humans. J Appl Physiol 86: 767–772, 1999. 5. Kukin ML, Kalman J, Charney RH, Levy DK, Buchholz-Varley C, Ocampo ON, and Eng C. Prospective, randomized comparison of effect of long-term treatment with metoprolol or carvedilol on symptoms, exercise, ejection fraction, and oxidative stress in heart failure. Circulation 99: 2645–2651, 1999. 6. Langton D, Way D, Trigg L, Blake D, and McGrath B. Vasoconstriction in the renal vascular bed during exercise: studies in control and heart failure rabbits. Clin Exp Pharmacol Physiol 17: 219 –223, 1990. 7. Laughlin MH, Korthuis RJ, Duncker DJ, and Bache RJ. Control of blood flow to cardiac and skeletal muscle during exercise. In: Handbook of Physiology. Exercise: Regulation and Integration of Multiple Systems. Bethesda, MD: Am. Physiol. Soc., 1996, sect. 12, chapt. 16, p. 705–769. 8. Leimbach WN Jr, Wallin BG, Victor RG, Aylward PE, Sundlöf G, and Mark AL. Direct evidence from intraneural recordings for increased 287 • DECEMBER 2004 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.32.247 on June 18, 2017 and in control subjects (23). These findings are at odds with those of Middlekauff et al. (15), who found lower baseline renal blood flows in HF than in controls. Whether this reduced resting renal blood flow was related to the severity of HF in the patients studied is not clear. It must be emphasized that with the methods used in the present report, we were unable to measure renal artery diameter and therefore were unable to compare resting levels of flow in the two groups. Thus comparisons of resting flow and vascular resistance reported in this study must be viewed with some caution. However, because renal diameter does not change during renal vasoconstriction with pharmacological compounds (11), we believe statements regarding flow velocity changes from resting velocity are valid. During short bouts of HG, renal blood flow fell more in HF patients than in controls. During fatiguing HG, we observed a group main effect (P ⬍ 0.04). Review of the data (Fig. 1) suggests that this effect was more prominent early in exercise than late in exercise, although a significant interaction was not noted. Similar observations were made by Langton et al. (6) using a doxorubicine-induced rabbit HF model. Compared with controls, HF rabbits had markedly reduced renal blood flows during submaximal exercise, whereas blood flow responses were similar in the two groups at the end of fatiguing exercise (6). In this report, the duration of HG to fatigue was not significantly different between groups. Because 9 of 10 HF subjects were receiving -blocker treatment, the question may arise regarding the effects of -blockers on exercise capacity in HF. Although -blockers generally cause a reduction in exercise capacity in healthy subjects, their effects in HF are not consistent. Studies in HF patients have reported either no effect (3) or little improvement (5, 24) in exercise capacity with -blocker treatment. Another important issue is the mode of exercise. In our report, all subjects performed isometric HG. Unlike dynamic exercise, blood flow to the contracting muscle becomes limited (7) during isometric exercise because muscle contraction itself occludes blood vessels. Thus we believe that the effects of -blocker treatment on skeletal muscle blood flow would be far less important than if we had examined renal blood flow during rhythmic exercise in HF. In the present study, it is unlikely that the muscle metaboreflex played an important role in eliciting the exaggerated renal vasoconstrictor response to exercise in HF. This is because the effect was seen early in exercise and the PHG-CA values for RBV reduction were not greater in HF patients than in controls. An argument can be made for greater central command in HF. However, if this had been the case, we would have expected a bigger HR response in HF patients than in controls. Moreover, voluntary and involuntary biceps contractions evoked similar increases in RVR in the HF patients and controls. If central command were an important mechanism responsible for renal vasoconstriction in humans, we would have expected no constrictor response during involuntary contraction. Thus these data suggest that the majority of the reduction in RBV during the initial periods of HG is due to augmented engagement of the muscle mechanoreflex in the HF patients. It should be noted that Rundqvist and colleagues (23) demonstrated similar relative changes in renal NE spillover during supine bicycle exercise in HF and in controls even though renal blood flow fell to a greater degree in HF patients than in controls. Moreover, DiBona et al. (2), using graded renal nerve stimulation in a rat model of HF, demonstrated that reductions HEART FAILURE, RENAL BLOOD FLOW, AND HANDGRIP 9. 10. 11. 12. 13. 15. 16. 17. 18. 19. AJP-Heart Circ Physiol • VOL 20. Muller AF, Batin P, Evans S, Hawkins M, and Cowley AJ. Regional blood flow in chronic heart failure: the reason for the lack of correlation between patients’ exercise tolerance and cardiac output? Br Heart J 67: 478 – 481, 1992. 21. Piepoli M, Clark AL, Volterrani M, Adamopoulos S, Sleight P, and Coats AJS. Contribution of muscle afferents to the hemodynamic, autonomic, and ventilatory responses to exercise in patients with chronic heart failure. Effects of physical training. Circulation 93: 940 –952, 1996. 22. Rotto DM and Kaufman MP. Effect of metabolic products of muscular contraction on discharge of group III and IV afferents. J Appl Physiol 64: 2306 –2313, 1988. 23. Rundqvist B, Eisenhofer G, Elam M, and Friberg P. Attenuated cardiac sympathetic responsiveness during dynamic exercise in patients with heart failure. Circulation 95: 940 –945, 1997. 24. Sanderson JE, Chan SK, Yip G, Yeung LY, Chan KW, Raymond K, and Woo KS. Beta-blockade in heart failure: a comparison of carvedilol with metoprolol. J Am Coll Cardiol 34: 1522–1528, 1999. 25. Shoemaker JK, Naylor HL, Hogeman CS, and Sinoway LI. Blood flow dynamics in heart failure. Circulation 99: 3002–3008, 1999. 26. Silber DH, Sinoway LI, Leuenberger UA, and Amassian VE. Magnetic stimulation of the human motor cortex evokes skin sympathetic nerve activity. J Appl Physiol 88: 126 –134, 2000. 27. Silber DH, Sutliff G, Yang QX, Smith MB, Sinoway LI, and Leuenberger UA. Altered mechanisms of sympathetic activation during rhythmic forearm exercise in heart failure. J Appl Physiol 84: 1551–1559, 1998. 28. Sinoway LI, Hill JM, Pickar JG, and Kaufman MP. Effects of contraction and lactic acid on the discharge of group III muscle afferents in cats. J Neurophysiol 69: 1053–1059, 1993. 29. Sterns DA, Ettinger SM, Gray KS, Whisler SK, Mosher TJ, Smith MB, and Sinoway LI. Skeletal muscle metaboreceptor exercise responses are attenuated in heart failure. Circulation 84: 2034 –2039, 1991. 30. Wilson JR, Martin JL, Schwartz D, and Ferraro N. Exercise intolerance in patients with chronic heart failure: role of impaired nutritive flow to skeletal muscle. Circulation 69: 1079 –1087, 1984. 31. Zelis R, Longhurst J, Capone RJ, and Mason DT. A comparison of regional blood flow and oxygen utilization during dynamic forearm exercise in normal subjects and patients with congestive heart failure. Circulation 50: 137–143, 1974. 287 • DECEMBER 2004 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.32.247 on June 18, 2017 14. central sympathetic outflow in patients with heart failure. Circulation 73: 913–919, 1986. Leuenberger UA, Mostoufi-Moab S, Herr M, Gray K, Kunselman A, and Sinoway LI. Control of skin sympathetic nerve activity during intermittent static handgrip exercise. Circulation 108: 2329 –2335, 2003. Li J and Sinoway LI. ATP stimulates chemically sensitive and sensitizes mechanically sensitive afferents. Am J Physiol Heart Circ Physiol 283: H2636 –H2643, 2002. Marraccini P, Fedele S, Marzilli M, Orsini E, Dukic G, Serasini L, and L’Abbate A. Adenosine-induced renal vasoconstriction in man. Cardiovasc Res 32: 949 –953, 1996. Massie B, Conway M, Yonge R, Frostick S, Ledingham J, Sleight P, Radda G, and Rajagopalan B. Skeletal muscle metabolism in patients with congestive heart failure: relation to clinical severity and blood flow. Circulation 76: 1009 –1019, 1987. Massie BM, Conway M, Rajagopalan B, Yonge R, Frostick S, Ledingham J, Sleight P, and Radda G. Skeletal muscle metabolism during exercise under ischemic conditions in congestive heart failure. Evidence for abnormalities unrelated to blood flow. Circulation 78: 320 –326, 1988. McClain J, Hardy C, Enders B, Smith M, and Sinoway L. Limb congestion and sympathoexcitation during exercise: implications for congestive heart failure. J Clin Invest 92: 2353–2359, 1993. Middlekauff HR, Nitzsche EU, Hoh CK, Hamilton MA, Fonarow GC, Hage A, and Moriguchi JD. Exaggerated muscle mechanoreflex control of reflex renal vasoconstriction in heart failure. J Appl Physiol 90: 1714 –1719, 2001. Middlekauff HR, Nitzsche EU, Nguyen AH, Hoh CK, and Gibbs GG. Modulation of renal cortical blood flow during static exercise in humans. Circ Res 80: 62– 68, 1997. Minotti JR, Christoph I, and Massie BM. Skeletal muscle function, morphology, and metabolism in patients with congestive heart failure. Chest 101: 333S–339S, 1992. Momen A, Leuenberger UA, Handly B, and Sinoway LI. Effect of aging on renal blood flow velocity during static exercise. Am J Physiol Heart Circ Physiol 287: H735–H740, 2004. Momen A, Leuenberger UA, Ray CA, Cha S, and Sinoway LI. Renal vascular responses to static handgrip: role of the muscle mechanoreflex. Am J Physiol Heart Circ Physiol 285: H1247–H1253, 2003. H2839