Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
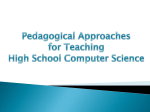
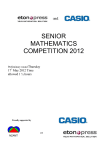
Renal lecture 2 • • • • Regulation of plasma ionic composition Regulation of plasma osmolarity Regulation of plasma hydrogen ion concentration Removal of metabolic waste and foreign substances • Regulation of salt and water balance • Anti-diuretic hormone • Renin- angiotension-aldosterone Dr Alice Witney Classification of Body Fluids Dr Alice Witney Ionic Composition of the Major Body-Fluid Compartments Dr Alice Witney Concept of Balance Input+production= utilization+output • If there is a positive balance, substances are entering faster than they are exiting • If there is a negative balance, substances are exiting faster than they are entering Dr Alice Witney Water Steady State • Amount Ingested = Amount Eliminated • Pathological losses vascular bleeding (H20, Na+) vomiting (H20, H+) diarrhea (H20, HCO3-). Dr Alice Witney Daily Salt Balance Dr Alice Witney Salt Balance • Very important in regulating ECF volume • Salt input occurs by ingestion – Often not well controlled • Salt balance maintained by outputs in urine – Salt also lost in perspiration and in feces • Kidneys keep salt constant in ECF – Glomerular filtration rate (GFR) – Tubular reabsorption of sodium Dr Alice Witney Osmolarity • Hypertonicity – Cells shrink – Causes • Insufficient water intake • Excessive water loss • Diabetes insipidus – Symptoms and effects • Shrinking of neurons – Confusion, irritability, delirium, convulsions, coma • Circulatory disturbances – Reduction in plasma volume, lowering of blood pressure, circulatory shock • Dry skin, sunken eyeballs, dry tongue Dr Alice Witney Osmolarity • Hypotonicity – Cells swell – Causes • Inability to excrete a dilute urine (renal failure) • when water is rapidly ingested • When excess water is retained in body due to inappropriate secretion of vasopressin – Symptoms and effects • Swelling of neurons – Confusion, irritability, lethargy, headache, dizziness, vomiting, drowsiness, convulsions, coma, death • Weakness (due to swelling of muscle cells) • Circulatory disturbances (hypertension and edema) Dr Alice Witney Water Reabsorption: Vasopressin (Anti-Diuretic Hormone; ADH) • ADH is synthesised within the Paraventricular Nucleus of the hypothalamus. hypothalamus Paraventricular nucleus pituitary • ADH is stored in the posterior pituitary. • ADH exerts a pressor effect (i.e., ↑BP) Dr Alice Witney Control of Vasopressin/ADH release • Left atrial receptors Monitor pressure of blood flowing through (reflects ECF volume) Upon detection of major reduction in arterial pressure, receptors stimulate vasopressin secretion and thirst • Osmoreceptors Monitor osmolarity of plasma in CNS and stimulates vasopressin secretion • Angiotensin II Stimulates vasopressin secretion and thirst when renin angiotensinaldosterone mechanism is activated to conserve Na+ Dr Alice Witney Vasopressin (Anti-Diuretic Hormone; ADH) hypothalamus 1. Dehydration or salt ingestion 2. ↑ Blood osmolarity 3. Stimulates osmoreceptors in the hypothalamus pituitary ↓ BP 5a. Causes vasoconstriction 4. Triggers ADH release from the pituitary ↑ TPR 5b. Promotes water retention by the kidney Dr Alice Witney ↑ BP ↑ Blood Volume Dr Alice Witney How does ADH work? (1) ADH binds to receptor on membrane of principal cell (2) Activation of a G protein activates enzyme to catalyse cAMP (3) Activates protein kinase A (4) Stimulates insertion of new water channels Dr Alice Witney DIABETES INSIPIDUS Kidneys stop conserving water Thirst Dehydration Damage to hypothalamus Low ADH Dr Alice Witney Urine Excretion • Depending on the body’s state of hydration, the kidneys secrete urine of varying concentrations. • • Too much water in the ECF establishes a hypotonic ECF. A water deficit establishes a hypertonic ECF. • A large, vertical osmotic gradient is established in the interstitial fluid of the medulla (from 100 to 1200 mOsm/liter to 1200 mOsm/liter). This increase follows the hairpin loop of Henle deeper into the medulla. • This osmotic gradient exists between the tubular lumen and the surrounding interstitial fluid. Dr Alice Witney Counter-current Multiplier Figure 19.7 Pg 542 (3rd Edition Germann & Stanfield) Dr Alice Witney 18:02:09 Dr Alice Witney 18:02:09 Dr Alice Witney Na+ Reabsorption • An active Na+ - K+ ATPase pump in basolateral membrane is essential for Na+ reabsorption • Of total energy spent by kidneys, 80% is used for Na+ transport • • Na+ is not reabsorbed in the descending limb of the loop of Henle Tubule area % of Na+ Role of Na+ reabsorbed reabsorption Proximal tubule 67% Plays role in reabsorbing glucose, amino acids, H2O, Cl-, and urea Ascending limb of the loop of Henle 25% Plays critical role in kidneys’ ability to produce urine of varying concentrations 8% Variable and subject to hormonal control; plays role in regulating ECF volume Distal and Water follows reabsorbed sodium collecting tubules by osmosis which has a main effect on blood volume and blood pressure Dr Alice Witney Sodium Reabsorption: Aldosterone • Sodium is the primary solute in ECF • Critical to the function of excitable cells • Regulation of sodium through reabsorption • Always actively reabsorbed Dr Alice Witney Regulation of Sodium Reabsorption and Balance • Na+ reabsorption in the proximal tubule is unregulated Therefore, regulation of GFR can contribute to Na+ regulation • Na+ reabsorption in the distal tubule is under hormonal control Aldosterone (increases Na+ reabsorption) Atrial Natriuretic Peptide (decreases Na+ reabsorption) Dr Alice Witney RAAS • Renin-angiotensin-aldosterone system • Most import and best known hormonal system involved in regulating Na+ Dr Alice Witney Factors Stimulating Renin Release afferent arteriole macula densa distal tubule JG cells (stretch sensitive) Dr Alice Witney 1 RAAS 2,3 4 5 1. Angiotensinogen produced by liver 2. Low BP and High sympathetic activity stimulate renin secretion 3. Decreased Na+ stimulate renin 4. Angiotensin I produced 5. Angiotensin II produced Dr Alice Witney steroid Aldosterone distal tubule adrenal gland Na+ K+ adrenal medulla adrenal cortex Dr Alice Witney Aldosterone renin angiotensin system collecting duct How does aldosterone work? Aldosterone: 1a) Stimulates the opening of sodium channels and potassium channels 1b) Stimulates synthesis and insertion of sodium/potassium pumps Dr Alice Witney Roles of Angiotensin II: 4 mechanisms Increase Blood Pressure Dr Alice Witney RAAS Dr Alice Witney • At the end of this lecture you should: • Understand the role of ADH in the control of water balance/plasma volume and thus blood pressure • Be familiar with the RAAS • Understand the role of aldosterone in salt balance • Know the actions of angiotensin II Dr Alice Witney Dr Alice Witney