Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
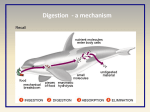
ON ESOPHAGEAL (FOOD PIPE) CANCER What is Esophagus? Where is it located? The esophagus is a muscular tube that transports saliva, liquid and food from the mouth to the stomach. When the patient is upright, the esophagus is usually between 25 to 30 muscular centimetres long. The layers from the esophagus is pinched together at both ends by sphincter muscles to prevent food or liquids leaking from the stomach back into the esophagus or mouth. When the patient swallows, the sphincters temporarily relax, to allow passage. The esophagus passes close to the trachea (berthing tube) and the left atrium (a section of the heart). This means the problem with the esophagus, such as eating something too hot, can sometimes feel like a pain close to or in the heart or throat. Like any other part of the body, the esophagus can be damaged. Heartburn and cancer are both problems affecting the esophagus. What is esophageal cancer? The wall of an esophagus is made up of several layers and the esophageal cancer generally starts from the inner wall and spreads both inwards and outwards. Very seldom the tumours and cancer arise from the middle muscular layer of the esophagus. Why have I developed esophageal cancer? The risk factors for squamous cells causes include smoking, tobacco and heavy use of alcohol. People who are infected with human papilloma virus are also at an increased risk. Those who suffer from achalasia cardia (a primary motor disorder of esophagus), chronic scarring of the esophagus due to prior corrosive injury, or Tylosis (a rare genetic disorder) are also at risk. The risk factors for adenocarcinoma are less understood. People who have Barrett’s Esophagus, an abnormal lining of the bottom part of the esophagus that is related to acid reflux problem, are at an increased risk compared to people who have long standing acid reflux problem. What are the symptoms of esophageal cancer? Early on, there may be no symptoms. In more advanced esophagus cancers, symptoms include: Difficulty or pain when swallowing | Weight loss | Pain in the chest, behind the breastbone | Coughing | Hoarseness | Indigestion and heartburn What investigations will I be subjected to? To diagnose esophagus cancer, your doctor will review your symptoms, medical history and examine you. In addition, he or she may order certain blood tests and X-Rays. Test for esophageal cancer may include: Barium swallow X-ray In which you drink a liquid that coats your esophagus. This makes the esophagus stand out on the X-ray so that your doctor can identify certain problems. Endoscopy The doctor passes an endoscope, a thin, lighted tube, down your throat into your esophagus to examine it. Endoscopic ultrasound uses sound waves to provide more information about the extent of tumour involvement in nearby tissues. Biopsy During an endoscopy, the doctor can take cells or tissues from your esophagus. The cells are examined under a microscope for the presence of cancer. Other tests, including computed tomography (CT) scans, positron emission tomography (PET) scan, thoracoscopy, and laparoscopy may be performed to determine if the cancer has spread, or metastasized, outside of the esophagus. This process is called “staging”. The doctor needs this information in order to plan your treatment. Are there different types of esophageal cancers? There are two main types of esophageal cancer. One type is squamous cell carcinoma. Squamous cells line the inner esophagus and cancer developing from squamous cells can occur along the entire esophagus. The other type is called adenocarcinoma. This is cancer that develops from gland cells. To develop adenocarcinoma of the esophagus, squamous cells that normally line the esophagus are replaced by gland cells. This typically occurs in lower esophagus near the stomach and is believed to be largely related to acid exposure to the lower esophagus. At what stage is the cancer? Accurate staging of cancer is based on histopathology & will be possible only after surgery. Based on clinical & radiological findings, esophageal cancer can be broadly classified into: Stage I: Cancer is detected only in top layers of cells lining the esophagus. Stage II: The Cancer involves deeper layers of lining of the esophgagus or it has spread to nearby lymph nodes. However, the cancer has not spread to other parts of the body. Stage III: The cancer has spread into the wall of esophagus or has spread to tissues or lymph nodes near the esophagus. However, it has not spread to other parts of body. Stage IV: The cancer has spread to other parts of the body, such as liver or lungs. Now that I have been diagnosed to have esophageal cancer, how will I be treated? The treatment of any cancer depends on the stage of cancer at the time it is diagnosed, other consideration include overall condition of the patient & specific symptoms the patient is having. In early stages, surgery to remove the majority of esophagus is the main form of therapy. Many patients also receive chemotherapy (intra venous drug therapy) & radiotherapy (X-Ray treatment). After surgery there is little information to prove that these additional treatments are useful. Many cancer centres are investigating the usefulness of giving chemotherapy or combined with radiotherapy prior to surgery for patients who are potentially curable. For patients who are found to have cancer spread to other organs or who, for some other reasons can’t undergo a surgery, combined chemotherapy & radiotherapy are the most common treatments. Since swallowing difficulty is not always relieved by this combined therapy, other means of improving swallowing are available like stenting (placement of flexible tube). Which kind of surgery is done for esophageal cancer? The type of surgery for Esophageal Cancer depends on the type & location of tumor. In squamous cell cancer, almost full length of esophagus along with nymph or lymph nodes are removed & anastomosis (joining of tube) is done in the neck. In Adenocarcinoma (which is located at lower part of esophagus in almost all cases), the upper part of esophagus is preserved and anastomosis is made inside the chest. There is not much role of surgery in case of esophageal cancer for the palliative purpose. To improve swallowing in non operative cases esophageal stenting (putting a tube in esophagus) is an option. Are there any alternatives besides surgery? To date, surgery is the only proven curative option for esophageal cancer. How do I prepare myself for surgery? The preparation is generally similar to any major surgery. If you are a smoker, then it is essential that you quit smoking. Breathing exercises using the incentive spirometer & football bladder should be started. Follow the anaesthetist’s advice regarding continuation of medications if you are on any. A high protein diet is preferred to improve nutrition. How major is surgery? What are possible complications? Esophagectomy with lymphadenectomy & other esophagus surgeries are considered as major surgeries and risk of complications are involved (up to 20%) and a very small risk of death (<4%). This means that if 100 people are operated, less than 4 of them have a chance of death. The complications of esophagectomy (removal of food pipe & lymph nodes) & joining back (anastomosis) the healthy stomach tube include: • Leak of anastomosis • Bleeding from anastomosis • Prolonged vomiting • Horsiness of voice. For how long do I stay in the hospital? In an uncomplicated case, hospital stay after surgery is 9-14 days. This may be longer when there are complications. Will I need any further treatment after surgery? The decision about adjuvant treatment is based on the final histopathology report which will be available approximately 7-10 days following surgery. If any of the lymph nodes are positive and your general condition is good enough then you may be referred to the medical (GI) oncologist for consideration for chemotherapy or in some cases. What will be my survival rate after surgery? Are there any chances of the cancer coming back? The survival depends on the stage of the disease. The average 5 year survival after curative surgery for esophagus cancer is 25 - 35%. This means that 25 - 35 out of a 100 people with esophageal cancer will survive and be disease-free at the end of 5 years. As of date, there is no fool proof way of predicting which patients will have recurrence and which patients will not. Are there any special precautions I need to take to prevent cancer from coming back? There are no proven precautions, but it is logical to exercise regularly, avoid using tobacco, drink alcohol in moderation and maintain a good diet. Following esophagectomy, since the size of the stomach is now reduced, you should eat smaller meals at regular intervals. How frequently should I follow up after surgery? After completion of treatment you will be advised to follow-up once in 3-4 months in the first 2 years. Then the frequency will be reduced to once in 6 months for the next 2-3 years. Subsequent follow up will be once a year. During each follow-up you will be asked to do certain blood tests. You may also be advised to get an ultrasound or CT scan of the abdomen and chest done. THE MEDICAL & SURGICAL CENTRE LTD HEAD OFFICE: Georges Guibert Street, Floréal 74111, Mauritius Tel: (230) 601 2300 Fax: (230) 696 3612 (Administration) / (230) 696 1209 (Medical) FCD NORTH: Office C, C0 – 05A & C2 – 204, La Croisette Mall, Grand Bay, Mauritius Tel: (230) 601 2300 | Fax: (230) 269 6224 Email: [email protected] | www.fortiscliniquedarne.com www.facebook.com/fortiscliniquedarne 24/7 Emergency and Ambulance Services: Dial 118