Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
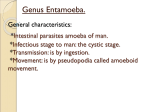
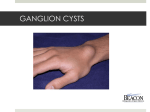
Review Article Pancreatic Cysts Preoperative Diagnosis and Clinical Management Martha Bishop Pitman, MD1; Kent Lewandrowski, MD1; Jian Shen, MD1; Dushyant Sahani, MD2; William Brugge, MD3; and Carlos Fernandez-del Castillo, MD4 Preoperative diagnosis of pancreatic cysts benefits from integrating the clinical, radiological, and cytological features. As patient management algorithms evolve to increasingly nonsurgical options, accuracy in distinguishing mucinous from nonmucinous and benign from malignant mucinous cysts is important. This review focuses on pseudocysts, serous cystadenomas, intraductal papillary mucinous neoplasms (IPMNs), and mucinous cystic neoplasms. Patients with pseudocysts almost always present with pancreatitis and are usually medically managed. Radiological studies reveal a unilocular cyst mostly in the pancreatic tail. Cyst fluid is thin, with high amylase but low carcinoembryonic antigen (CEA) levels. DNA mutations are absent. Serous cystadenomas are benign and do not require resection. Patients are usually asymptomatic and have microcystic or macrocystic masses anywhere in the pancreas. Cytology is frequently nondiagnostic. CEA and amylase levels are low. DNA analysis may reveal loss of heterozygosity (LOH) at 3p if associated with Von Hippel-Lindau disease. Neoplastic mucinous cysts are highly variable in their presentation. Most are resected. Mucinous cystic neoplasms typically arise in the body or tail of the pancreas of middle-aged women and demonstrate a septated cyst without dilatation of the main pancreatic duct. Branch duct IPMNs are more common in the pancreatic head of elderly men. Main duct dilatation correlates with main duct or combined type IPMN. Both types of mucinous cysts produce variable amounts of mucin. Cytologically nonmalignant but atypical epithelial cells, even when scant, are an indication of a high risk for malignancy. High CEA level supports a mucinous cyst, as do KRAS mutation and good quality DNA levels. KRAS mutation and multiple LOH support malignancy. C 2009 American Cancer Society. Cancer (Cancer Cytopathol) 2010;118:1–13. V KEYWORDS: pancreas, endoscopic ultrasound, fine-needle aspiration biopsy, endoscopic ultrasound fine-needle aspiration, intraductal papillary mucinous neoplasm, mucinous cyst, pancreatic cysts, cyst fluid analysis, carcinoembryonic antigen, molecular analysis, KRAS. Cysts of the pancreas constitute a broad spectrum of entities from non-neoplastic to malignant cysts (Table 1). Until the 1980s, cysts of the pancreas were thought to be relatively rare, but with the routine use of improved cross-sectional imaging, there has been a dramatic increase in the detection of pancreatic cysts in general and asymptomatic cysts in particular.1-8 It is now estimated that approximately 1.2% of general medical patients have a pancreatic cyst requiring follow-up.4,9 Historically, all suspected neoplastic pancreatic cysts have been resected in good surgical candidates because of the uncertainty in the biological behavior of mucinous cysts as well as the uncertainty in preoperative diagnosis. Management algorithms have evolved, however, and nonsurgical treatment options are increasingly available because of our improved understanding of the biological behavior of cystic neoplasms as well as our improved ability to accurately diagnose these cysts preoperatively.8,10-20 Accurate preoperative diagnosis is essential for proper patient management, and the pathologist plays a key role in the preoperative diagnosis. Despite the relatively low sensitivity and specificity of cytology alone in this regard,21-23 when used in a multimodal approach, cytology plays an important role in patient management decisions.11,12,24 We review our current multimodal approach to the preoperative diagnosis of pancreatic cysts at the Massachusetts General Hospital, which includes clinical and radiological evaluation, cytology, cyst fluid chemical analysis for Corresponding authors: Martha Bishop Pitman, MD, Department of Pathology, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114; Fax: (617) 724-6564; [email protected] 1 Department of Pathology, Massachusetts General Hospital, Boston, Massachusetts; 2Department of Radiology, Massachusetts General Hospital, Boston, Massachusetts; 3Department of Medicine, Division of Gastroenterology, Massachusetts General Hospital, Boston, Massachusetts; 4Department of Surgery, Massachusetts General Hospital, Boston, Massachusetts DOI: 10.1002/cncy.20059, Received: July 27, 2009; Revised: August 28, 2009; Accepted: September 1, 2009, Published online December 30, 2009 in Wiley InterScience (www.interscience.wiley.com) Cancer Cytopathology February 25, 2010 1 Review Article Table 1. Cysts of the Pancreas Non-neoplastic cysts Pseudocyst Retention cyst Congenital cyst Foregut cyst Endometriotic cyst Cystic nonepithelial neoplasms Lymphangioma Hemangioma Primarily cystic epithelial neoplasms Serous cystadenoma Microcystic Macrocystic Mucinous cystic neoplasm Mucinous Mucinous Mucinous Mucinous cystic cystic cystic cystic neoplasm neoplasm neoplasm neoplasm with with with with low-grade dysplasia moderate dysplasia high-grade dysplasia (CIS) invasive carcinoma Intraductal papillary mucinous neoplasm Intraductal papillary Intraductal papillary Intraductal papillary dysplasia (CIS) Intraductal papillary mucinous neoplasm with low-grade dysplasia mucinous neoplasm with moderate dysplasia mucinous neoplasm with high-grade mucinous neoplasm with invasive carcinoma Miscellaneous cysts Lymphoepithelial cyst Epidermoid cyst in intrapancreatic heterotopic spleen Secondarily cystic solid neoplasms Solid-pseudopapillary neoplasm Ductal adenocarcinoma Endocrine neoplasms Acinar cell neoplasms CIS indicates carcinoma in situ. Modified from Hruban RH, Pitman MB, Klimstra DS. Tumors of the Pancreas. Atlas of Tumor Pathology. 4th Series. Fascicle 6. Washington, DC: American Registry of Pathology, Armed Forces Institutes of Pathology; 2007. carcinoembryonic antigen (CEA) and amylase, and in select cases, molecular analysis. Although there are many benign and malignant cysts in the pancreas to be aware of, we focus on pseudocysts, serous cystadenomas (SCA), and mucinous cysts (mucinous cystic neoplasms [MCN] and intraductal papillary mucinous neoplasms [IPMNs]), as these cysts represent the most commonly encountered cysts in the pancreas. Clinical Management Patients with known pseudocysts are generally treated medically with drainage.25 A history of acute or chronic pancreatitis, or trauma, is almost always present.26 Serous cystadenomas are benign neoplasms that can be monitored when small but are resected when large (>4 cm), 2 growing rapidly, or symptomatic.27 For patients with suspected mucinous cysts, treatment decisions may be based on the presence or absence of symptoms, size of the cyst, radiological features of the cyst, cytological and other parameters of cyst fluid analysis, patient age, and surgical risk factors.14-16,20 Although both MCNs and IPMNs are known to have malignant potential, and therefore have historically all been resected, recent studies highlighting slow growth and indolence of many of these neoplastic mucinous cysts15,17 have led to increased use of nonsurgical alternatives, from close clinical follow-up to in situ ablation.13,20,28-33 Main duct IPMNs, regardless of symptoms, cytology, or the presence of a mural nodule, are considered high risk for malignancy, and are therefore all resected in surgically fit candidates.8,34 For patients with suspected branch duct IPMNs or MCNs, recent international consensus guidelines recommend surgical resection for patients with mucinous cysts either >3 cm or smaller cysts with high-risk features such as symptoms, positive cytology, or a mural nodule.14 We and others have shown, however, that not all asymptomatic cysts <3 cm12,31,35 or those with less than positive cytology are benign,11,24,28,31 and therefore have proposed aspiration and analysis of fluid from most pancreatic cysts, especially those suspected of being mucinous cysts.20 The specific mode of analysis depends on the fluid volume available. Role of Imaging in Pancreas Cyst Evaluation Imaging plays a crucial role in both detection and characterization of pancreatic cysts. Identification of the cyst’s morphologic details, such as internal septa, micro- or macrocystic appearance, presence of a central scar, cyst communication, cyst wall irregularity, mural nodules, pancreatic duct dilation, and calcification, are essential to categorize a cyst as a pathologic subtype and to stratify risks for potential aggressive behavior.4,20,36 Recent advances in computed tomography (CT), magnetic resonance imaging (MRI), and magnetic resonance cholangiopancreatography (MRCP) imaging techniques as well as the postprocessing methods of the image have led to high quality image acquisition and display in 2D or 3D planes that have improved our ability to confidently recognize cyst features and make a reliable diagnosis. The multidetector row CT is about 80% accurate for discriminating a nonmucinous from a mucinous cyst, and for predicting malignancy.20 MRI and MRCP have inherently superior soft tissue contrast over CT that facilitates Cancer Cytopathology February 25, 2010 Update on Cysts of the Pancreas/Pitman et al Table 2. Morphology of Pancreatic Cysts and Surgical Pathology Diagnoses Unilocular Microcystic Macrocystic Cyst With Solid Component Pseudocyst Retention cyst IPMN MCN Unilocular SCA SCA IPMN MCN IPMN SCA Acinar cystadenoma Lymphangioma Lymphoepithelial cyst MCN IPMN Solid-pseudopapillary neoplasm Neuroendocrine neoplasm Adenocarcinoma Metastases Acinar cell carcinoma SCA indicates serous cystadenoma; MCN, mucinous cystic neoplasm; IPMN, intraductal papillary mucinous neoplasm. recognition of subtle morphologic details not obvious on CT, including small mural nodules, communication between a branch duct cyst and the main duct, in the evaluation of IPMNs.20,37-39 Despite these advances in CT and MRI, reliable image diagnosis of pancreatic cysts is not always possible because of considerable morphological overlap in various cyst subtypes, especially small (<3 cm) cysts. As such, a classification system of cyst morphology has recently been proposed for assessing the risk of malignancy.40 The 4 categories in this system are unilocular, microcystic, macrocystic, and cysts with a solid component (Table 2). Unilocular cysts are those with thin walls and without internal septa, a solid component, or central cyst wall calcification. Of this subtype, pseudocysts are the most common, in which case the patient nearly always presents with a clinical history of pancreatitis (Fig. 1). The diagnosis is supported by imaging findings of inflammation, atrophy, or calcification of pancreatic parenchyma, and dilatation of and calculi in a typically thin-walled cyst. Less commonly, unilocular cysts can be branch duct IPMNs, SCAs, or lymphoepithelial cysts. Benign SCAs are the only true microcystic lesions; however, branch duct IPMNs can produce a raspberrylike microcystic appearance. Typically, SCAs demonstrate a pattern of numerous tiny cysts that range from a few millimeters up to 2 cm and show uniform lobulations. A fibrous central scar is pathognomonic, but is only seen in 30% of multidetector row CT images. Macrocystic lesions are larger (>2 cm in diameter) and yet have fewer compartments than microcystic tumors. Microcystic neoplasms may appear solid, and when microcystic areas are focal in an otherwise oligocystic serous cystadenoma, there may be confusion with a high-risk mucinous cyst. Mucinous cystic neoplasms are found predominantly in young to middle-aged women, are well defined, exophytic lesions commonly located in the tail, and do not Cancer Cytopathology February 25, 2010 Figure 1. An axial computed tomography scan of a pseudocyst revealed a large, thin-walled unilocular cyst around the head of the pancreas after pancreatitis. communicate with the pancreatic duct. Branch duct IPMNs are most often seen in older men. Whereas main pancreatic duct IPMNs are morphologically distinct, branch duct or combined IPMNs often show features similar to other macrocystic lesions. The presence of a channel of communication between the cyst and the main duct is highly suggestive of a branch duct IPMN. Uncommon macrocystic lesions include nonfunctioning neuroendocrine neoplasm, lymphangioma, and rare congenital malformations. The presence of a solid mass or mural nodule in either unilocular or multilocular cysts, main pancreatic duct dilatation >10 mm, thick septations, and biliary obstruction are recognized features of malignancy (Fig. 2).20,37 Both multidetector row CT and MRCP are helpful in characterizing cystic pancreatic neoplasms and, if performed appropriately, demonstrate comparable performance.39,41 In patients with small cysts (<3 cm) without suspicious features, where surgery is not considered the appropriate next step of management, imaging can be used as a 3 Review Article Figure 2. An intraductal papillary mucinous neoplasm with invasive carcinoma is shown. A mural nodule is a high-risk feature of malignancy in a mucinous cyst. surveillance tool to longitudinally follow lesions that could progress to malignancy. Endoscopic Ultrasound and Endoscopic Ultrasound Fine-Needle Aspiration The strength of endoscopic ultrasound (EUS) is its ability to detect and aspirate small cystic lesions with a high level of safety. EUS is very sensitive for detecting small cysts, many of which are branch duct IPMNs, but imaging alone is insufficient for differentiating between mucinous and nonmucinous22 as well as between benign and malignant lesions.42 EUS assists in the detection of malignancy arising from MCNs or IPMNs by demonstrating focal nodules and invasive lesions, and guiding fine-needle aspiration (FNA) of suspicious lesions.43,44 The EUS criteria for malignancy in IPMNs are: 1) main duct >10 mm, 2) focal cystic lesion >3 cm, and 3) nodule >5 mm.45,46 EUS-FNA is performed with a linear echoendoscope passed into the duodenum through the stomach. Pancreatic cystic lesions are readily seen as hypoechoic (dark) lesions within the pancreatic parenchyma on EUS (Fig. 3). FNA is usually performed with a 22-gauge needle containing an occluding stylet. With the echoendoscope transducer in close proximity to the cystic lesion, the needle is guided in a perpendicular path to the wall of the cyst. With 1 passage of the needle into the lumen of the cyst, aspiration of cyst fluid is initiated with suction. The cyst fluid is aspirated until the cyst collapses. Highly viscous fluid may require a considerable amount of time for evacuation of the cyst contents, and this is the first clue that the cyst is likely mucinous. Focal nodules, thick septations, and adjacent masses should be targeted for aspiration and cytologic examination. 4 Figure 3. A mucinous cystic neoplasm with low-grade dysplasia is shown. This endoscopic ultrasound image depicts a large cyst with thin septations in the pancreatic tail of a middle-aged woman. The aspiration needle is seen reflected diagonally across the cyst cavity. Allocation of cyst fluid should be based on the dominant clinical question (Fig. 4). When the clinical question is whether the cyst is mucinous, cyst fluid CEA should receive the highest priority for testing. Consideration of molecular testing of the cyst fluid for KRAS or other mutations is entertained when the clinical and radiological features strongly support a mucinous cyst without obvious malignant features such as a mural nodule or invasion of adjacent structures, and the clinical question is benign versus malignant. Molecular testing should also be considered if the cyst fluid is too scant for CEA and likely nondiagnostic cytology (<1 mL). There are few complications associated with cyst FNA, but intracystic bleeding is the most common. Usually the bleeding stops spontaneously without sequel. Acute pancreatitis is a rare complication, but potentially serious. Cyst Fluid Analysis Chemical analysis of pancreatic cyst fluid has evolved from an experimental evaluation of a long list of cancer antigens, including CEA, CA 72-4, CA 125, CA 19-9, and CA 15-3 to CEA alone, as it has been shown to be the most accurate marker to date to distinguish nonmucinous from mucinous cysts.23,47,48 CEA does not, however, distinguish benign from malignant mucinous neoplasms.23,49 It should be understood, however, that measurement of CEA in cyst fluid has not been approved by the US Food and Drug Administration (FDA), and therefore represents an off-label application in this setting. Furthermore, Cancer Cytopathology February 25, 2010 Update on Cysts of the Pancreas/Pitman et al Figure 4. An algorithm for fluid triage from pancreatic cysts answers the clinical questions of (A) mucinous versus neoplastic nonmucinous cysts and (B) benign versus malignant mucinous cysts. CEA indicates carcinoembryonic antigen. no commercially available CEA assays have been formally validated for any of the cyst fluid matrices that may be encountered in clinical practice. Published cyst fluid data and cutoff values must therefore be viewed with caution, because important validation parameters such as linearity, precision, accuracy, and stability have not been reported. Each cyst type represents a unique matrix that would need to be independently validated. In addition, the handling of cyst fluid submitted for CEA analysis is not standardized, with some laboratories receiving fluid undiluted, and others diluted or placed in fixative such as Preservcyt (Hologic, Inc, Marlborough, Mass) or Cytorich red (Becton-Dickinson, Burlington, NC). Approximately 1 mL of fluid is needed for the CEA analysis. If samples are too scant, too viscous to pipette, or inhomogeneous because of mucin clumps in watery fluid, the cyst fluid can be diluted with saline and/or vortexed to achieve homogeneity. The dilution factor must be accounted for in the final CEA value reported. As such, it is best to let the laboratory handle the fresh, undiluted fluid. Debris within the cyst Cancer Cytopathology February 25, 2010 fluid that may clog the pipette should be removed by centrifugation. Grossly bloody samples present a unique problem, given that contaminating peripheral blood dilutes the cyst fluid by an unknown dilution factor. This is mostly a problem just below the cutoff value, as elevated CEA levels still provide useful information. Finally, it must be remembered that cyst fluid values using different commercial assays may not yield equivalent results. Therefore, reported cutoff values are assay specific, and it is inappropriate to apply a reported cutoff value to an assay from a different manufacturer. That being said, a cyst fluid CEA level of <192 ng/mL (at Massachusetts General Hospital) fails to support the presence of a mucinous cyst, and values >192-200 ng/mL (at Massachusetts General Hospital) support the interpretation of a mucinous cyst.23,48,50,51 A level >800 ng/mL is 98% specific for a mucinous cyst using a meta-analysis of pooled data from 12 studies at different institutions.47 Increasing the cutoff value of CEA for support of a mucinous cyst will have a negative effect on sensitivity. In this same meta-analysis, levels <5 ng/mL were 98% specific for a serous cystadenoma.47 Amylase is also a helpful marker, as amylase is typically very high, usually in the thousands and almost never <250 ng/mL in pseudocysts,47 but is low in serous cysts.23,47 Although it would seem to make sense that high amylase levels would be consistently found in IPMNs, in contrast to MSNs, because of the connectivity to the pancreatic ductal system, this has not proven to be true in our experience.52 Like CEA, measurement of amylase or lipase in pancreatic cyst fluids has never been formally validated or approved by the FDA. Comments concerning technical problems for amylase measurement are similar to those described for CEA. As a final caveat, amylase values may be particularly useful when elevated to rule out the possibility that the cyst in question may be a nonpancreatic cyst. Molecular Analysis of Cyst Fluid The molecular testing of cyst fluid has increased over the past few years because of the availability of a commercially available test (PathFinderTG, RedPath Integrated Pathology, Pittsburgh, Pa) coupled with increasingly small amounts of cyst fluid too scant for chemical analysis or diagnostically useful cytology. Similar to pancreatic ductal adenocarcinoma, molecular alterations in neoplastic mucinous cysts of the pancreas have also demonstrated multistep genetic changes involving early KRAS mutation, followed by p53 5 Review Article mutation, and loss of p16 and SMAD4.53-58 Detection of these underlying molecular changes using cyst fluid DNA derived from exfoliated epithelial cells in a small volume of fluid has become a focus of active research. The group from the University of Pittsburgh subjected cyst fluid obtained from EUS-guided FNA to DNA extraction followed by polymerase chain reaction amplification.59,60 DNA quantity/quality, KRAS-2 gene mutation in the first exon, and loss of heterozygosity (LOH) using microsatellite markers closely linked to a broad panel of genomic loci associated with tumor suppressor genes including p53, p16, PTEN, APC, CDKN2A, CMM, MCC, and VHL, were analyzed and compared with histology.59,60 Their early studies showed that increased levels of DNA, the presence of KRAS mutation, or 2 loci of allelic imbalance (loss of heterozygosity) was each associated more significantly with a mucinous neoplasm, whereas a high amplitude of mutations, more specifically the sequence of KRAS-2 gene mutation followed by allelic loss, was predictive of malignancy.59,60 These results initiated the commercialized testing developed by this group (PathFinderTG, RedPath Integrated Pathology). The use of this specific commercially available molecular analysis is controversial, however. Recent studies have demonstrated that the overall performance of molecular analysis was inferior to CEA analysis in predicting mucinous cysts, although KRAS mutation did show higher specificity, and the concordance of CEA level with increased DNA level, KRAS mutation, or 2 allelic imbalances appeared to be poor (kappa ¼ 0.1-0.3).61 Interestingly, however, in the same study by Sawhney et al,61 the authors showed that although an elevated CEA level (82%) showed higher sensitivity than molecular analysis (77%), the combination of CEA and molecular analysis achieved 100% sensitivity, suggesting that CEA and molecular data may be complimentary rather than concordant. When using a multimodal approach to diagnosis that includes clinical information, CEA level, EUS features, and cytology to render a clinical consensus diagnosis instead of CEA level alone, we found good concordance between the clinical consensus and molecular diagnosis in the categories of nonmucinous, benign mucinous, and malignant mucinous cysts, with an overall kappa statistic of 0.816.62 A recently published multi-institutional prospective study (PANDA study),63 the largest study so far, included 113 cysts with histologic follow-up and found that among the 3 changes, including DNA level, KRAS mutation, and 2 loci of allelic loss, KRAS mutation 6 showed the highest odds ratio (20.9) and specificity (96%), but a low sensitivity (45%), for mucinous cysts. The specific sequence of KRAS mutation followed by allelic imbalance detected in cyst fluid was shown to be specifically associated with mucinous cysts and malignancy, although the sensitivity is again suboptimal.63 In addition to a CEA cutoff value of 192 ng/mL, the presence of a KRAS mutation identified additional mucinous cysts and improved the sensitivity of CEA from 64% to 82% for combination of CEA and KRAS while maintaining the specificity at 83%. Data from the PANDA study, in conjunction with others,61-63 highlight the importance of interpreting information from molecular analysis in the context of the clinical and radiological information as well as cyst fluid analysis for maximizing the sensitivity and accuracy for the diagnosis of mucinous cysts. The current commercially available molecular analysis is by a single commercial laboratory (RedPath Integrated Pathology), and it is unknown whether these results can be reliably reproduced in other laboratories. Most of the published studies have limited sample size and population bias, because the study cohort often consists of a higher number of patients with malignant cysts than expected because of the availability of histologic follow-up. A longer observation period and accumulation of molecular data are needed to draw a definitive conclusion about the clinical utility of molecular analysis of pancreatic cyst fluid in the future. Nevertheless, the current data at least allow us to conclude that cyst fluid analysis for DNA level, KRAS mutation, and allelic imbalances cannot replace other clinical ancillary tests such as CEA or cytology at the present time; rather, this molecular analysis adds additional information to the complex preoperative diagnostic puzzle. Given the increasingly small cysts that are detected resulting in small sample sizes inadequate for optimal cytology or CEA analysis (<1 mL) in many cases, the promise of information from analyzing such a small amount of cyst fluid (200 lL) may be sufficient to warrant this ancillary test despite the expense. In cysts with sufficient aspirate volumes for cytology and CEA analysis, the value-added benefit of molecular analysis is yet to be determined. Cytological Features of Pancreatic Cysts The most important job for the pathologist is to distinguish pseudocysts that can be medically managed from neoplastic cysts that may require resection. The second most important distinction for the pathologist to make is between a serous cyst and a mucinous cyst. Distinguishing Cancer Cytopathology February 25, 2010 Update on Cysts of the Pancreas/Pitman et al lesional cells and fluid from gastrointestinal contamination is vital to making an accurate interpretation. In addition, as we have emphasized in this review, it is important for the pathologist not to interpret the cytology specimen in a vacuum, but to make an interpretation with the knowledge of the clinical history, radiological features, and any ancillary tests, especially cyst fluid analysis of CEA and amylase. Understanding and incorporating these factors into the interpretation of the cytomorphologic findings guides the pathologist into making a more meaningful report for the various clinicians in charge of patient management decisions. Ancillary tests, such as special stains, immunohistochemical tests, and molecular tests, are part of the final pathology report for virtually all pathology specimens, and pancreatic cyst fluid should not be different. Below, the 4 major cysts of the pancreas are discussed using a multimodal approach. Figure 5. A pseudocyst is shown. It is a granular and proteinaceous cyst fluid without cyst-lining cells that may contain histiocytes, inflammation, hemosiderin, and flecks of hematoidin pigment (Cytospin; Papanicolaou stain, high power). Pseudocyst Fluid from a cyst in the clinical setting of pancreatitis and/ or alcohol abuse, or with a history of trauma, should place pseudocyst at the top of the differential diagnosis at the time of slide examination. Caution is needed, however, because patients with IPMNs, and to a lesser degree MCNs and SCAs, can present clinically with pancreatitis.15,27,64 The cyst fluid aspirated from an uncomplicated pseudocyst is generally thin and nonmucoid, and is frequently discolored (not white). An infected pseudocyst, however, may produce purulent, mucoid-appearing fluid. The cells present in the fluid may include acute and chronic inflammatory cells, histiocytes, and hemosiderinladen or foamy macrophages, and by definition should not contain any cyst lining epithelial cells. The background is often granular and proteinaceous, and may contain flecks of hematoidin pigment (Fig. 5).65 Not all pseudocysts have a characteristic ‘‘dirty’’ proteinaceous background, and the cyst contents may appear rather clear with only scattered histiocytes, which may appear epithelioid and can be mistaken for epithelial cells.66 Gastrointestinal epithelial and mucin contamination, particularly from the stomach, can lead to a misdiagnosis of a mucinous cyst.65,67,68 Special stains for mucin that show only scant amounts of mucin-positive fluid should not be interpreted as evidence of a mucinous neoplasm, as this finding may well represent gastrointestinal contamination. Cyst fluid analysis with an elevated amylase in the thousands and low CEA level (<192 ng/mL) supports the interpretation of a pseudocyst.23,47,65 Molecular analysis should not reveal KRAS mutation or LOH.62,63 Serous Cystadenoma Patients are typically asymptomatic without a history of pancreatitis.27 Distinction of a serous from a mucinous cyst is not always straightforward. Despite the more solid than cystic composition of the typical microcystic serous cystadenoma, obtaining diagnostic tissue with EUS-FNA is difficult.69-72 Oligocystic and unilocular variants of serous cystadenoma also occur, mimicking branch duct IPMN and MCNs.20,39 Aspirated fluid is thin and clear or thin and bloody and typically of very scant volume. Intact cells are few, and the scant glycogenated cytoplasm is very delicate, is often destroyed or distorted with smearing.69,70 Many cases are interpreted as nondiagnostic because of insufficient cellularity. Intact cell clusters are composed of bland cuboidal cells with round central to slightly eccentric nuclei and scant finely vacuolated but nonmucinous cytoplasm (Fig. 6). Epithelial cells present on a cellblock preparation or unstained cytospins can be evaluated with histological stains for periodic acid-Schiff (PAS) and PAS with diastase to confirm the presence of cytoplasmic glycogen. In our experience, there is rarely sufficient cyst fluid for cellblock preparation or additional cytospin preparations for such testing. We have noted that hemosiderin-laden macrophages may be a clue to the diagnosis when present in a clean, nonproteinaceous background.69 By using the multimodal approach, even if it is not technically considered diagnostic from a pure cytological point of view, these cells in the setting of a microcystic or septated (rarely unilocular) cyst in the body/tail of the Cancer Cytopathology February 25, 2010 7 Review Article Figure 6. A serous cystadenoma is shown, demonstrating bland cuboidal cells with round central to slightly eccentric nuclei and scant finely vacuolated but nonmucinous cytoplasm (direct smear; Papanicolaou stain, high power). Figure 7. Thick and viscous cyst fluid from either an intraductal papillary mucinous neoplasm or a mucinous cystic neoplasm is reflected on the slide as a thick sheet of colloid-like mucin that often covers much of the slide (direct smear; Papanicolaou stain, low power). pancreas with a low CEA (<5 ng/mL) and amylase level (<250 U/L) are sufficient to be consistent with an interpretation of a serous cystadenoma. Molecular analysis may reveal LOH at 3p25, as serous cystadenomas are associated with von Hippel-Lindau syndrome.73 KRAS mutation or multiple LOH should not be detected.62,63 much of the slide (Fig. 7). Mucin contamination from the gastrointestinal tract will not be of this quality or quantity, and special stains for mucin and CEA analysis are not needed to confirm this type of cyst fluid as mucin. Degenerated inflammatory cells and histiocytes within the mucin provide added support that the mucin is from the cyst.83 This type of mucin is sufficient in and of itself even if acellular to make a diagnosis of a neoplastic mucinous cyst.12,74,79 Approximately 50% of neoplastic mucinous cysts lack such obvious extracellular mucin in our experience. Extracellular mucin may appear as focally thick clumps or thin wisps, and as focal or diffuse thin background mucin not easily observed on routine preparations. Mucin stains can be difficult to interpret because gastrointestinal contamination may introduce wisps of mucin into the specimen, so care must be taken not to interpret any wisp of mucin-positive material as indicative of a mucinous cyst. Scattered wavy clumps or a uniform film of mucin as well as intracytoplasmic mucin accentuated with either Alcian blue or mucicarmine help to identify thin mucin and distinguish it from fibrin and protein (Fig. 8). Liquid-based cytology attenuates the appearance of mucin even more, and is not a recommended mode of cyst fluid processing. In most cases, CEA analysis is particularly helpful in these situations, as an elevated level >192 ng/mL (at Massachusetts General Hospital) supports the interpretation of thin or scant extracellular mucin as originating from a mucinous cyst. MCNs and IPMNs: Neoplastic Mucinous Cysts The cellularity of cyst fluid is rarely sufficient or characteristic enough to distinguish the 2 mucinous cysts, typically resulting in a generic cytology report of a mucinous cyst. Given that the cytological features of the 2 mucinous cysts are similar with respect to the grade of dysplasia, as well as the diagnostic features of carcinoma resulting in similar patient management decisions, these neoplastic mucinous cysts will be discussed together. Aspiration of a neoplastic mucinous cyst produces highly variable amounts of extracellular mucin and cyst lining epithelium.12,21,74-81 Cytology may underestimate the final histologic grade of neoplastic mucinous cyst, given that the cyst lining is quite heterogeneous, and the degree of epithelial atypia may not be representative of the highest degree of atypia of the cyst on histology.12,79,82 Aside from the clinical suspicion of a neoplastic mucinous cyst, the presence of a mucinous cyst is often confirmed at the time of aspiration when thick, viscous mucus is grossly appreciated by the aspirator. Direct smears of this thick and viscous cyst fluid are reflected on the slide as thick sheets of colloid-like mucin that covers 8 Cancer Cytopathology February 25, 2010 Update on Cysts of the Pancreas/Pitman et al Figure 8. An Alcian blue stain highlights scant, thin extracellular and intracellular mucin (direct smear; Alcian blue histochemical stain, high power). Figure 9. Contaminating gastric epithelium may be impossible to distinguish from lesional epithelium of low-grade mucinous cysts (direct smear; Papanicolaou stain, high power). Screening the cytology preparations for an epithelial component is critical to accurate interpretation of the risk of malignancy.11,12,79 Neoplastic mucinous cysts with low-grade dysplasia (adenomas) are difficult to diagnose, because of scantily cellular aspirates that rarely produce epithelial cells confidently interpreted as arising from the cyst. For branch duct IPMNs most commonly lined by gastric-foveolar type epithelial cells, a transgastric EUSFNA may introduce contaminating gastric epithelium impossible to distinguish from lesional epithelium (Fig. 9). Fortunately, most branch duct IPMNs are Cancer Cytopathology February 25, 2010 Figure 10. A mucinous cystic neoplasm with low-grade dysplasia is shown. A small strip of glandular epithelial cells demonstrates cytoplasmic mucin filling the entire cytoplasmic compartment (Cytospin; Papanicolaou stain, high power). located in the pancreatic head, and are accessed by a transduodenal approach, allowing for an easier distinction between duodenal contaminating epithelium and lesional epithelium. MCNs are much more common in the body and tail of the pancreas; however, so distinguishing the epithelium of a MCN adenoma and gastric epithelium remains a challenge. One should not expect a benign MCN adenoma to shed much epithelium into the cyst lining, a fact that is exploited in the molecular analysis of the cyst fluid, resulting in low DNA quantity and quality.62,63 The presence of few single cells, small clusters, and small strips of bland glandular epithelial cells that demonstrate cytoplasmic mucin filling the entire cytoplasmic compartment favors lesional epithelium in contrast to columnar epithelium with a uniform apical mucin cup typical of gastric epithelium (Fig. 10).67 Atypical epithelial cells are most critical to recognize, as we have shown that these cells even when very scant correlate with an increased risk of malignancy.12,62,79 A neoplastic mucinous cyst with a cyst lining of moderate or higher dysplasia may produce atypical epithelial cells in small, tight, bud-like clusters or singly with increased nuclear to cytoplasmic ratio, irregular nuclear membranes, and cytoplasm with or without mucin (Fig. 11). Crowded groups of cells with open chromatin, irregular nuclear membranes and nucleoli, and necrosis support the interpretation of carcinoma both in cyst fluid and in solid mass lesions.79,84-86 Small atypical epithelial cells with necrosis are also a suspicious finding (Fig. 12). 9 Review Article Conclusions In the optimal patient management algorithm, an asymptomatic patient with a noninvasive mucinous cyst could be conservatively managed. We advocate a multimodal approach using cytology, CEA, and molecular analysis in selective cases and emphasize the importance of the cytologist in the preoperative diagnosis of pancreatic cysts. CONFLICT OF INTEREST DISCLOSURES The authors made no disclosures. REFERENCES Figure 11. An intraductal papillary mucinous neoplasm with moderate dysplasia is shown. A small cluster of atypical epithelial cells in a small, tight, bud-like cluster demonstrates an increased nuclear-to-cytoplasmic ratio, irregular nuclear membranes, and cytoplasm with a small mucin vacuole (direct smear; Papanicolaou stain, high power). Figure 12. An intraductal papillary mucinous neoplasm with invasive carcinoma is shown. Atypical epithelial cells and background necrosis support the interpretation of carcinoma, usually invasive carcinoma (direct smear; Papanicolaou stain, high power). Such atypical cells are not those expected from benign epithelium from the stomach or duodenum.67,68 Accurate distinction between carcinoma in situ and invasive carcinoma has not been extensively investigated. In our experience, background cellular, coagulative-type necrosis (not just a few degenerated cells in mucin) distinguished noninvasive from invasive tumors.79 10 1. Mallery JS, Centeno BA, Hahn P, Chang Y, Warshaw A, Brugge WR. Pancreatic tissue sampling guided by EUS, CT/US, and surgery: a comparison of sensitivity and specificity. Gastrointest Endosc. 2002;56:218-224. 2. Eloubeidi M, Chen V, Eltoum I, et al. Endoscopic ultrasound-guided fine needle aspiration biopsy of patients with suspected pancreatic cancer: diagnostic accuracy and acute and 30-day complications. Am J Gastroenterol. 2003;98: 2663-2668. 3. Brugge WR. Role of endoscopic ultrasound in the diagnosis of cystic lesions of the pancreas. Pancreatology. 2001;1:637640. 4. Brugge WR, Lauwers GY, Sahani D, Fernandez-del Castillo C, Warshaw AL. Cystic neoplasms of the pancreas. N Engl J Med. 2004;351:1218-1226. 5. Lee LS, Saltzman JR, Bounds BC, Poneros JM, Brugge WR, Thompson CC. EUS-guided fine needle aspiration of pancreatic cysts: a retrospective analysis of complications and their predictors. Clin Gastroenterol Hepatol. 2005;3: 231-236. 6. Brugge WR. Cystic pancreatic lesions: can we diagnose them accurately? what to look for? FNA marker molecular analysis resection, surveillance, or endoscopic treatment? Endoscopy. 2006;38(suppl 1):S40-S47. 7. Adsay NV. Cystic neoplasia of the pancreas: pathology and biology. J Gastrointest Surg. 2008;12:401-404. 8. Ferrone CR, Correa-Gallego C, Warshaw AL, et al. Current trends in pancreatic cystic neoplasms. Arch Surg. 2009; 144:448-454. 9. Spinelli KS, Fromwiller TE, Daniel RA, et al. Cystic pancreatic neoplasms: observe or operate. Ann Surg. 2004;239: 651-657; discussion 57-59. 10. Pitman MB. The pancreas. In: Sidawy M, Ali S, eds. Fine Needle Aspiration Cytology. Philadelphia, PA: Churchill Livingston, Elsevier;2007:251–298. 11. Pitman MB, Deshpande V. Endoscopic ultrasound-guided fine needle aspiration cytology of the pancreas: a morphological and multimodal approach to the diagnosis of solid and cystic mass lesions. Cytopathology. 2007;18:331-347. 12. Pitman MB, Michaels PJ, Deshpande V, Brugge WR, Bounds BC. Cytological and cyst fluid analysis of small (3 cm) branch duct intraductal papillary mucinous neoplasms adds value to patient management decisions. Pancreatology. 2008;8:277-284. 13. Gan SI, Thompson CC, Lauwers GY, Bounds BC, Brugge WR. Ethanol lavage of pancreatic cystic lesions: initial pilot study. Gastrointest Endosc. 2005;61:746-752. Cancer Cytopathology February 25, 2010 Update on Cysts of the Pancreas/Pitman et al 14. Tanaka M, Chari S, Adsay V, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology. 2006;6:17-32. 15. Crippa S, Salvia R, Warshaw AL, et al. Mucinous cystic neoplasm of the pancreas is not an aggressive entity: lessons from 163 resected patients. Ann Surg. 2008;247:571-579. 16. Scheiman JM. Management of cystic lesions of the pancreas. J Gastrointest Surg. 2008;12:405-407. 17. Liao T, Velanovich V. Asymptomatic pancreatic cysts: a decision analysis approach to observation versus resection. Pancreas. 2007;35:243-248. 18. Wilentz RE, Albores-Saavedra J, Zahurak M, et al. Pathologic examination accurately predicts prognosis in mucinous cystic neoplasms of the pancreas. Am J Surg Pathol. 1999; 23:1320-1327. 19. Wilentz RE, Albores-Saavedra J, Hruban RH. Mucinous cystic neoplasms of the pancreas. Semin Diagn Pathol. 2000; 17:31-42. 20. Sahani DV, Lin DJ, Venkatesan AM, et al. Multidisciplinary approach to diagnosis and management of intraductal papillary mucinous neoplasms of the pancreas. Clin Gastroenterol Hepatol. 2009;7:259-269. 21. Frossard JL, Amouyal P, Amouyal G, et al. Performance of endosonography-guided fine needle aspiration and biopsy in the diagnosis of pancreatic cystic lesions. Am J Gastroenterol. 2003;98:1516-1524. 22. Stelow EB, Stanley MW, Bardales RH, et al. Intraductal papillary-mucinous neoplasm of the pancreas. The findings and limitations of cytologic samples obtained by endoscopic ultrasound-guided fine needle aspiration. Am J Clin Pathol. 2003;120:398-404. 23. Brugge WR, Lewandrowski K, Lee-Lewandrowski E, et al. Diagnosis of pancreatic cystic neoplasms: a report of the cooperative pancreatic cyst study. Gastroenterology. 2004;126: 1330-1336. 24. Pitman MB, Faquin WC. The fine-needle aspiration biopsy cytology of pancreatoblastoma. Diagn Cytopathol. 2004; 31:402-406. 25. Barthet M, Lamblin G, Gasmi M, Vitton V, Desjeux A, Grimaud JC. Clinical usefulness of a treatment algorithm for pancreatic pseudocysts. Gastrointest Endosc. 2008;67: 245-252. 26. Kloppel G. Pseudocysts and other non-neoplastic cysts of the pancreas. Semin Diagn Pathol. 2000;17:7-15. 27. Tseng JF, Warshaw AL, Sahani DV, Lauwers GY, Rattner DW, Fernandez-del Castillo C. Serous cystadenoma of the pancreas: tumor growth rates and recommendations for treatment. Ann Surg. 2005;242:413-419; discussion 19-21. 28. Grobmyer SR, Cance WG, Copeland EM, Vogel SB, Hochwald SN. Is there an indication for initial conservative management of pancreatic cystic lesions? J Surg Oncol. 2009;100:372374. 29. Walsh RM, Vogt DP, Henderson JM, et al. Management of suspected pancreatic cystic neoplasms based on cyst size. Surgery. 2008;144:677-684; discussion 84-85. 30. Tang RS, Weinberg B, Dawson DW, et al. Evaluation of the guidelines for management of pancreatic branch-duct intraductal papillary mucinous neoplasm. Clin Gastroenterol Hepatol. 2008;6:815-819; quiz 719. 31. Garcea G, Ong SL, Rajesh A, et al. Cystic lesions of the pancreas. A diagnostic and management dilemma. Pancreatology. 2008;8:236-251. 32. Oh HC, Seo DW, Lee TY, et al. New treatment for cystic tumors of the pancreas: EUS-guided ethanol lavage Cancer Cytopathology February 25, 2010 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. with paclitaxel injection. Gastrointest Endosc. 2008;67:636642. Sahani DV, Saokar A, Hahn PF, Brugge WR, FernandezDel Castillo C. Pancreatic cysts 3 cm or smaller: how aggressive should treatment be? Radiology. 2006;238:912919. Waters JA, Schmidt CM. Intraductal papillary mucinous neoplasm—when to resect? Adv Surg. 2008;42:87-108. Lee CJ, Scheiman J, Anderson MA, et al. Risk of malignancy in resected cystic tumors of the pancreas < or ¼3 cm in size: is it safe to observe asymptomatic patients? A multiinstitutional report. J Gastrointest Surg. 2008;12:234-242. Allen PJ, D’Angelica M, Gonen M, et al. A selective approach to the resection of cystic lesions of the pancreas: results from 539 consecutive patients. Ann Surg. 2006; 244:572-582. Song SJ, Lee JM, Kim YJ, et al. Differentiation of intraductal papillary mucinous neoplasms from other pancreatic cystic masses: comparison of multirow-detector CT and MR imaging using ROC analysis. J Magn Reson Imaging. 2007; 26:86-93. Fukukura Y, Fujiyoshi F, Hamada H, et al. Intraductal papillary mucinous tumors of the pancreas. Comparison of helical CT and MR imaging. Acta Radiol. 2003;44:464-471. Sahani DV, Kadavigere R, Blake M, Fernandez-Del Castillo C, Lauwers GY, Hahn PF. Intraductal papillary mucinous neoplasm of pancreas: multi-detector row CT with 2D curved reformations–correlation with MRCP. Radiology. 2006;238:560-569. Sahani DV, Kadavigere R, Saokar A, Fernandez-del Castillo C, Brugge WR, Hahn PF. Cystic pancreatic lesions: a simple imaging-based classification system for guiding management. Radiographics. 2005;25:1471-1484. Sainani NI, Saokar A, Deshpande V, Fernandez-del Castillo C, Hahn P, Sahani DV. Comparative performance of MDCT and MRI with MR cholangiopancreatography in characterizing small pancreatic cysts. AJR Am J Roentgenol. 2009;193:722-731. Ahmad NA, Kochman ML, Lewis JD, Ginsberg GG. Can EUS alone differentiate between malignant and benign cystic lesions of the pancreas? Am J Gastroenterol. 2001; 96:3295-3300. Pais SA, Attasaranya S, Leblanc JK, Sherman S, Schmidt CM, DeWitt J. Role of endoscopic ultrasound in the diagnosis of intraductal papillary mucinous neoplasms: correlation with surgical histopathology. Clin Gastroenterol Hepatol. 2007; 5:489-495. Poley JW, Kluijt I, Gouma DJ, et al. The yield of first-time endoscopic ultrasonography in screening individuals at a high risk of developing pancreatic cancer. Am J Gastroenterol. 2009;104:2175-2181. Ahmad NA, Kochman ML, Brensinger C, et al. Interobserver agreement among endosonographers for the diagnosis of neoplastic versus non-neoplastic pancreatic cystic lesions. Gastrointest Endosc. 2003;58:59-64. Okabayashi T, Kobayashi M, Nishimori I, et al. Clinicopathological features and medical management of intraductal papillary mucinous neoplasms. J Gastroenterol Hepatol. 2006; 21:462-467. van der Waaij LA, van Dullemen HM, Porte RJ. Cyst fluid analysis in the differential diagnosis of pancreatic cystic lesions: a pooled analysis. Gastrointest Endosc. 2005;62: 383-389. 11 Review Article 48. Maire F, Voitot H, Aubert A, et al. Intraductal papillary mucinous neoplasms of the pancreas: performance of pancreatic fluid analysis for positive diagnosis and the prediction of malignancy. Am J Gastroenterol. 2008;103:28712877. 49. Correa-Gallego C, Warshaw AL, Fernandez-del Castillo C. Fluid CEA in IPMNs: a useful test or the flip of a coin? Am J Gastroenterol. 2009;104:796-797. 50. Linder JD, Geenen JE, Catalano MF. Cyst fluid analysis obtained by EUS-guided FNA in the evaluation of discrete cystic neoplasms of the pancreas: a prospective single-center experience. Gastrointest Endosc. 2006;64:697-702. 51. Shami VM, Sundaram V, Stelow EB, et al. The level of carcinoembryonic antigen and the presence of mucin as predictors of cystic pancreatic mucinous neoplasia. Pancreas. 2007;34:466-469. 52. Moparty B, Pitman MB, Brugge WR. Pancreatic cyst fluid amylase is not a marker to differentiate IPMN from MCN. Gastrointest Endosc. 2007;65:AB303. 53. Hruban R, Goggins M, Parsons J, Kern S. Progression model for pancreatic cancer. Clin Cancer Res. 2000;6:2969-2972. 54. Izeradjene K, Combs C, Best M, et al. Kras(G12D) and Smad4/Dpc4 haploinsufficiency cooperate to induce mucinous cystic neoplasms and invasive adenocarcinoma of the pancreas. Cancer Cell. 2007;11:229-243. 55. Biankin AV, Biankin SA, Kench JG, et al. Aberrant p16(INK4A) and DPC4/Smad4 expression in intraductal papillary mucinous tumours of the pancreas is associated with invasive ductal adenocarcinoma. Gut. 2002;50:861868. 56. Jimenez RE, Warshaw AL, Z’Graggen K, et al. Sequential accumulation of K-ras mutations and p53 overexpression in the progression of pancreatic mucinous cystic neoplasms to malignancy. Ann Surg. 230:501-509, 1999; discussion 509511. 57. Gerdes B, Wild A, Wittenberg J, et al. Tumor-suppressing pathways in cystic pancreatic tumors. Pancreas. 2003;26:4248. 58. Yoshizawa K, Nagai H, Sakurai S, et al. Clonality and K-ras mutation analyses of epithelia in intraductal papillary mucinous tumor and mucinous cystic tumor of the pancreas. Virchows Arch. 2002;441:437-443. 59. Khalid A, McGrath KM, Zahid M, et al. The role of pancreatic cyst fluid molecular analysis in predicting cyst pathology. Clin Gastroenterol Hepatol. 2005;3:967-973. 60. Schoedel KE, Finkelstein SD, Ohori NP. K-Ras and microsatellite marker analysis of fine-needle aspirates from intraductal papillary mucinous neoplasms of the pancreas. Diagn Cytopathol. 2006;34:605-608. 61. Sawhney MS, Devarajan S, O’Farrel P, et al. Comparison of carcinoembryonic antigen and molecular analysis in pancreatic cyst fluid. Gastrointest Endosc. 2009;69:1106-1110. 62. Shen J, Brugge WR, Dimaio CJ, Pitman MB. Molecular analysis of pancreatic cyst fluid: a comparative analysis with current practice of diagnosis. Cancer Cytopathol. 2009;117: 217-227. 63. Khalid A, Zahid M, Finkelstein SD, et al. Pancreatic cyst fluid DNA analysis in evaluating pancreatic cysts: a report of the PANDA study. Gastrointest Endosc. 2009;69:1095-1102. 64. Salvia R, Fernandez-del Castillo C, Bassi C, et al. Mainduct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection. Ann Surg. 2004;239:678-685. 12 65. Gonzalez Obeso E, Murphy E, Brugge W, Deshpande V. Pseudocyst of the pancreas: the role of cytology and special stains for mucin. Cancer Cytopathol. 2009;117:101-107. 66. Stelow EB, Bardales RH, Stanley MW. Pitfalls in endoscopic ultrasound-guided fine-needle aspiration and how to avoid them. Adv Anat Pathol. 2005;12:62-73. 67. Nagle J, Wilbur DC, Pitman MD. The cytomorphology of gastric and duodenal epithelium and reactivity to B72.3: a baseline for comparison to pancreatic neoplasms aspirated by EUS-FNAB. Diagn Cytopathol. 2005;33:381-386. 68. Nawgiri RS, Nagle JA, Wilbur DC, Pitman MB. Cytomorphology and B72.3 labeling of benign and malignant ductal epithelium in pancreatic lesions compared to gastrointestinal epithelium. Diagn Cytopathol. 2007;35:300-305. 69. Belsley NA, Pitman MB, Lauwers GY, Brugge WR, Deshpande V. Serous cystadenoma of the pancreas: limitations and pitfalls of endoscopic ultrasound-guided fine-needle aspiration biopsy. Cancer. 2008;114:102-110. 70. Huang P, Staerkel G, Sneige N, Gong Y. Fine-needle aspiration of pancreatic serous cystadenoma: cytologic features and diagnostic pitfalls. Cancer. 2006;108:239-249. 71. Logrono R, Vyas SH, Molina CP, Waxman I. Microcytic adenoma of the pancreas: cytologic appearance on percutaneous and endoscopic ultrasound-guided fine-needle aspiration. Report of a case. Diagnostic Cytopathol. 1999;20:298-301. 72. Lal A, Bourtsos EP, DeFrias DV, Nemcek AA, Nayar R. Microcystic adenoma of the pancreas: clinical, radiologic, and cytologic features. Cancer. 2004;102:288-294. 73. Mohr VH, Vortmeyer AO, Zhuang Z, et al. Histopathology and molecular genetics of multiple cysts and microcystic (serous) adenomas of the pancreas in von Hippel-Lindau patients. Am J Pathol. 2000;157:1615-1621. 74. Layfield LJ, Cramer H. Fine-needle aspiration cytology of intraductal papillary-mucinous tumors: a retrospective analysis. Diagn Cytopathol. 2005;32:16-20. 75. Dodd LG, Farrell TA, Layfield LJ. Mucinous cystic tumor of the pancreas: an analysis of FNA characteristics with an emphasis on the spectrum of malignancy associated features. Diagn Cytopathol. 1995;12:113-119. 76. Recine M, Kaw M, Evans DB, Krishnamurthy S. Fine-needle aspiration cytology of mucinous tumors of the pancreas. Cancer. 2004;102:92-99. 77. Sole M, Iglesias C, Fernandez-Esparrach G, Colomo L, Pellise M, Gines A. Fine-needle aspiration cytology of intraductal papillary mucinous tumors of the pancreas. Cancer. 2005;105:298-303. 78. Emerson RE, Randolph ML, Cramer HM. Endoscopic ultrasound-guided fine-needle aspiration cytology diagnosis of intraductal papillary mucinous neoplasm of the pancreas is highly predictive of pancreatic neoplasia. Diagn Cytopathol. 2006;34: 457-462. 79. Michaels PJ, Brachtel EF, Bounds BC, Brugge WR, Pitman MB. Intraductal papillary mucinous neoplasm (IPMN) of the pancreas: cytohistologic analysis and correlation with histologic grade. Cancer Cytopathol. 2006;108:163-173. 80. Bardales RH, Stelow EB, Mallery S, Lai R, Stanley MW. Review of endoscopic ultrasound-guided fine-needle aspiration cytology. Diagn Cytopathol. 2006;34:140-175. 81. Stelow EB, Shami VM, Abbott TE, et al. The use of fine needle aspiration cytology for the distinction of pancreatic mucinous neoplasia. Am J Clin Pathol. 2008;129:67-74. 82. Basturk O, Coban I, Adsay NV. Pancreatic cysts: pathologic classification, differential diagnosis, and clinical implications. Arch Pathol Lab Med. 2009;133:423-438. Cancer Cytopathology February 25, 2010 Update on Cysts of the Pancreas/Pitman et al 83. Lau SK, Lewandrowski KB, Brugge WR, Warshaw AL, Centeno BA. Diagnostic significance of mucin in fine needle aspiration samples of pancreatic cysts. Mod Pathol. 2000; 13:48A. 84. Robins DB, Katz RL, Evans DB, Atkinson EN, Green L. Fine needle aspiration of the pancreas. In quest of accuracy. Acta Cytol. 1995;39:1-10. Cancer Cytopathology February 25, 2010 85. Lin CC, Lin CJ, Hsu CW, Chen YC, Chen WT, Lin SM. Fine-needle aspiration cytology to distinguish dysplasia from hepatocellular carcinoma with different grades. J Gastroenterol Hepatol. 2008;23:e146-e152. 86. Lin F, Staerkel GA. Cytologic criteria for well differentiated adenocarcinoma of the pancreas in fine-needle aspiration biopsy specimens. Cancer. 2003;99:44-50. 13