Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
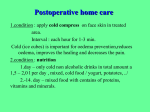
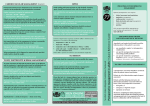
N124IN Spring 2013 Used for: • Connective tissue diseases where joints are severely deteriorated • Long-term steroid therapy • Avascular necrosis Inadequate blood supply causes bone tissue death Goal: • Alleviate severe chronic pain • Improve capability to perform ADLs Replacement of any synovial joint can occur Arthroplasty Replacement devices/prostheses • Made of: metal, ceramic, plastic, combination • Hold in place: cement, patient bone • Bone substitutes (biologics) Used when bone isn’t able to support replacement devices • Bone glues/fillers, bone stimulants Assist in better support for prosthetics 2-piece device • Acetabular cup that’s placed into pelvic acetabulum • Femoral part that’s placed into femur Replaces femoral head/neck Cemented THR average life span: 10 years Noncemented prostheses: can last longer Preoperative Care • Case manager • Ensure patient has caregiver available to help patient after surgery • Standard preoperative care • Baseline assessments Neurovascular status of extremity Pain Mobility • IV Prophylactic antibiotics Preoperative Care, cont. • Education Surgery Postoperative expectations • Meet with physical therapist Learn exercises for postoperatively Learn how to walk with walker/crutches • Total joint education programs, if present • Autologous blood donation • Typically admitted morning of surgery Length of stay is usually 2-5 days Joint camp programs Postoperative Care • Interdisciplinary • Patient moves into chair night of surgery or next morning No adduction or hyperflexion of surgical hip! • Weight bearing dependent upon prosthesis type Cemented: as tolerated or full weight bearing Uncemented: toe-touch, partial weight bearing, or featherweight bearing Postoperative Care, cont. • Pain management Initially: epidural analgesia, patient-controlled analgesia (PCA), analgesic injections After first day: oral analgesic Proper positioning • Early ambulation Walker, crutches Cane • Hip flexion restriction Educate patients to not bend forward • Interventions to prevent complications Postoperative Complications: Hip Dislocation • Can be a partial dislocation (subluxation) or total dislocation • When femoral component dislodges from acetabular cup • Audible “pop” and then pain Surgical leg shortens and possibly rotates • Nursing considerations Keep patient in bed Inform surgeon stat Give analgesics until surgery Postoperative Complications: Hip Dislocation, cont. • Prevention After PACU, keep patient in supine position with slightly elevated head of bed Use methods to prevent leg adduction Trapezoid-shaped abduction pillow, splint, wedge, bed pillows When turning patient, avoid hip adduction Prevent hyperflexion Use fracture pan when patient is on bedrest and needs to void Postoperative Complications: Skin Breakdown • Turn patient at least q 2 hours • Keep heels off bed • Prophylactic DuoDERM dressings • Heel protectors • Incontinence Keep clean/dry Help patient to toilet every 2 hours Use protective barrier cream • Diet, hydration Postoperative Complications: Infection • Prophylactic IV antibiotic preoperatively Can also give intraoperatively and postoperatively for 24 hrs • Aseptic wound care at incision, drain sites • Assess for infection signs/symptoms Redness, swelling, warmth, odor, pain, drainage that is yellow/green/brown Temperature Confusion (elderly) • Antibiotics often placed into wound during surgery Beads, part of cement mixture, irrigating solution Postoperative Complications: Bleeding • Surgical drain (Hemovac, Jackson-Pratt) Empty q 8-12 hours or per orders • Assess dressing for bleeding; reinforce if necessary • Blood transfusion On day 2-3, hemoglobin/hematocrit may decline • Replace blood Collect shed blood postoperatively into reservoir via suction Filter, reinfuse within 6 hrs • Assess for signs of blood loss and shock Postoperative Complications: Neurovascular Compromise • Neurovascular checks Circulation (color, warmth, pulses) Sensation Movement Postoperative Complications: Thromboembolitic Complications • DVT, pulmonary embolus risk • Preventions: Thigh-high elastic stockings Sequential compression devices (SCDs) Anticoagulant medications Subcutaneous low molecular weight heparin (Lovenox) Oral warfarin (Coumadin) Heparin Assess partial thromboplastin times (heparin), International normalized ration/prothrombin time (warfarin) Leg exercises Rehabilitation • Home with rehabilitation, subacute care unit, rehabilitation unit, nursing home • Rehab continues after discharge until patient can ambulate and perform selfcare independently Education • Hip precautions Prevent dislocation Keep legs abducted Place pillows between legs when sleeping Bend at waist (not more than 90 degrees) Push straight up off chair or bed when getting up and don’t lean forward Use walker if needed Use equipment to help put on socks/shoes Total replacement • 3 components Femoral, tibial, patellar button Similar to care of patient with THR • After surgery, drain and bulky dressing in place • Assess for bleeding • Standard postoperative care • Work to prevent complications similar to those for total hip replacement Continuous passive motion (CPM) machine • Physician orders degree of flexion and speed • Can be applied by nurse, physical therapist, technician • Used intermittently (8-12 hours/day) or continuously when patient is in bed • Purpose: Keeps joint mobile • Nursing care Position joint over machine’s flexion area Use padding, especially at proximal end Make sure speed/angle settings are correct and monitor them per protocol Assess toleration of speed/angle Body part removal • Surgical Caused by disease • Traumatic Caused by accident Surgical Amputation • Primary indication: ischemia related to peripheral vascular disease in elderly • Can also be done for: Bone tumors Thermal injuries (frostbite, electric shock) Crushing injuries Congenital problems Infections Traumatic Amputation • Accident-related Industrial machinery, motor vehicles, lawn mowers, chain saws, snow blowers • Replantation may occur Amputated part is typically healthy Prehospital care of part: Wrap in cool, slightly moist cloth Put in sealed plastic bag Can submerge bag in cold water until hospital Microscope used in reattachment procedure Nerves, vessels, muscle reattached Amputation levels • Lower Extremity Small toes: little problem Great toe: more of problem because it alters balance and gait Midfoot: preferred over below-the-knee for PVD Syme amputation: most of foot removed, ankle left intact for walking and weight bearing Lower leg: below-the-knee preferred over above-the-knee for joint function preservation Hip disarticulation: hip joint removal Hemipelvectomy: part of pelvis removal Hemicorporectomy: hemipelvectomy and translumbar amputation Removes almost half of body Bowel and urinary diversion surgeries (ostomies) required Levels of Amputation, cont. • Upper Extremity More often result from trauma Upper extremities needed for ADLs Will more than likely have a greater impact on individual than a lower extremity amputation Replacement with prosthesis early is important Levels Of Amputation, cont. • Below-the-knee (BKA) • Above-the-knee (AKA) • Below-the-elbow (BEA) • Above-the-elbow (AEA) Preoperative Care • Elective amputations Education Prosthesis fitting Adjustment to loss Review postoperative and rehab care • Traumatic amputations No preparation for changes Meet physical needs Address psychological and emotional concerns • Assess reaction to having amputation • Identify support systems and coping mechanisms Postoperative Care • Standard post operative care • Interventions to prevent complications (hemorrhage, infection) • Pain control • Mobility/Ambulation • Prosthesis care • Lifestyle adaptation Postoperative Care: Prevention of Hemorrhage • Large pressure dressing is placed on patient after surgery Secured with elastic wrap • Palpate most distal pulse between heart and amputated body part Assess strength Compare with other extremity Postoperative Care: Prevention of Hemorrhage, cont. • Assess dressing for bloody drainage Circle, date, time drainage and assess for enlargement Inform surgeon if bleeding continues • Keep tourniquet available in case of hemorrhage • After dressing is removed: Assess for perfusion to skin flap at end of stump Light-skinned patient: skin should be pink Dark-skinned patient: skin should not be discolored Stump should be warm, not hot Postoperative Care: Prevention of Infection • Assess wound for signs of infection • Assess temperature • Traumatic amputations have infection risk due to injury’s nature and exposure to environmental pathogens Postoperative Care: Pain control • Incisional pain • Phantom limb pain Severe pain where body part was Described as: intense burning, crushing sensation, or cramping Can be triggered by: touching stump, fatigue, emotional stress, pressure changes, weather changes Treat pain with meds and complementary therapies Knifelike pain: anticonvulsants Burning sensations: beta-blocking agents Nerve pain: gabapentin, amitriptyline Complementary therapies: biofeedback, massage, imagery, hypnosis, acupuncture, acupressure, distraction Postoperative Care: Mobility/Ambulation • Prevent swelling Cold application Elevate limb for 24 hrs or less • Assess limb periodically to make sure it lies completely flat • Have patient avoid flexion positions Lying prone assists in preventing contractures (30 minutes, 4 times a day) • Rehabilitation (sub-acute unit, extended care facility, ambulatory basis) • Trapeze bar Postoperative Care: Prosthesis care • Prepare residual limb for prosthesis • Wrap residual limb q 8 hours with elastic wrap in figure-of-eight pattern With each wrapping, do neurovascular checks and assess for infection and tissue integrity alterations Start with distal portion and move proximally until bandage secures to most proximal joint Bandage needs to be tighter at distal end Postoperative Care: Prosthesis care, cont. • Perform and educate patient on prosthesis care Use mild soap and water to clean prosthesis socket Dry it after Regularly clean inserts and liners To keep socks in place, use garters Grease parts per instructions When shoes wear out, replace them with shoes that are same height and type Postoperative Care: Lifestyle adaptation • If necessary, job analysis may be performed • Most patients can return to work after surgery • Many individuals who have amputations can bowl, ski, hike, etc. • Assess family support • Assist patient with setting realistic expectations • If patient did not get prosthesis, may need to have home adaptations for wheelchair http://www.youtube.com/watch?v=UQo7 QOz_EO0 http://www.youtube.com/watch?v=njJUc TbR2SY&feature=related