Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
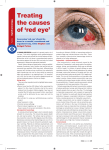
CLINICAL Exploring the different causes of this condition Subconjunctival haemorrhages Not all of them are benign Leonid Skorin Jr, OD, DO, FAAO, FAOCO Patients presenting with a subconjunctival haemorrhage are a common occurrence in every ophthalmic practice. In one study, 2.9% of patients who presented to the outpatient eye clinics and hospitals of a large medical university system over one year were diagnosed with this condition . This study also found that there may be different causes for subconjunctival haemorrhages, with minor local trauma being the most frequent cause in all age groups . Systemic hypertension was noted predominantly in those over 50 years . 1 1 1 Patients with subconjunctival haemorrhages often present with focal or diffuse areas of blood under the conjunctiva and without frank pain but possible irritation and usually no vision loss2,3. The haemorrhage may obscure only a small sector of the underlying sclera or involve the entire visible conjunctiva3. If the haemorrhage is located superiorly on the conjunctiva, it is not uncommon that with gravitational forces, the blood will migrate downward and make it appear as if the haemorrhage is enlarging3. Initially, the haemorrhage is bright red, but the colour changes to a yellowish green, like a bruise, as it resolves2,4. In those cases when the haemorrhage involves the perilimbal conjunctiva, blood breakdown products can be seen in the anterior peripheral corneal stroma as a greenish discoloration4. The borders of the haemorrhage may be distinct or feathered4. In severe cases, when there is a larger accumulation of blood in the subconjunctival space, the conjunctiva may become elevated and redundant, and protrude or prolapse through the palpebral fissure4. Trauma Trauma, even relatively minor trauma to the globe, such as rubbing one’s eye too hard, may cause a subconjunctival haemorrhage1. Often, detailed questioning by the clinician will make the patient remember the incident of such minor trauma to the eye. The frequency of haemorrhage from local trauma is increased in the Summer months when people tend to be more active1. Close inspection of the globe and the area in question with biomicroscopy is recommended to rule out a deeper or more extensive injury, which may be concealed by the blood4. In cases of more extensive injury, consider the possibility of blow-out fracture when subconjunctival and eyelid hematomas develop after a blunt injury to the orbit5. Case 1, Figure 1 A 60-year old man was struck by a fist in his left eye during an altercation. He had an extensive subconjunctival haemorrhage, periorbital oedema and ecchymosis. Extraocular motility was restricted in all fields of gaze. A CT-scan of the orbits identified an orbital floor fracture. Various surgeries can cause post-surgical traumatic subconjunctival haemorrhages. These would include any surgery of the eye or its adnexa. Even LASIK surgery has been found to result in such haemorrhages2. Birth trauma often causes a subconjunctival haemorrhage in newborns2. Case 2, Figure 2 A child with eyelid ecchymosis and subconjunctival haemorrhage after surgical excision of chalazion. Differential diagnosis Most subconjunctival haemorrhages are benign and are the result of innocuous causes. A thorough patient history needs to be taken to help guide the clinician, if a more ominous entity for the subconjunctival haemorrhage is suspected. Figure 2 Case 3, Figure 3 About the author Dr Leonid Skorin Jr is in group practice at the Albert Lea Eye Clinic, Mayo Health System, Minnesota, USA 32 | January 27 | 2006 OT Figure 1 An 80-year old woman underwent unremarkable phacoemulsification cataract extraction. One day post-operatively, she presented with a subconjunctival haemorrhage involving the lower two-thirds of the globe. Her vision was slightly diminished, but this was attributed to postoperative corneal oedema and not to the haemorrhage. No hyphaema was present. In older children, such haemorrhages, especially if they are present bilaterally, may be a sign of child abuse6. CLINICAL Exploring different causes of this condition Figure 3 Figure 5 Case 4, Figure 4 Case 5, Figure 5 Bleeding disorders A young boy was seen in the emergency department of a hospital for a fractured humerus. Bilateral subconjunctival haemorrhages were also identified during the examination. No retinal haemorrhages were present. The child was referred to Children’s Services for suspected child abuse. A 39-year old woman tried to asphyxiate herself by wrapping a cord tightly around her neck. The suicide attempt was unsuccessful. She was examined in a psychiatric facility. Although she had prominent subconjunctival haemorrhages, there were no corresponding retinal haemorrhages. Her visual acuity was unaffected. Other physical activity such as dancing, weight lifting and even inverted positioning have been known to cause subconjunctival haemorrhages9,10. Blood clotting disorders are associated with multiple conditions, such as liver disease, cancer and genetic problems11. Severe hepatic diseases are associated with subconjunctival haemorrhage, as are retinal haemorrhages12. Pancytopenia, which is the pronounced reduction in the number of erythrocytes, all types of white blood cells and the blood platelets in the circulating blood, can cause subconjunctival haemorrhage1. This type of bleeding can also be found in patients with thrombocytopenia, which is a condition where there is an abnormally small number of platelets in the circulating blood13. Around 1-2% of the population (US) has von Willebrand’s disease – an autosomal dominant trait expressing a deficiency in the coagulation cascade and possibly a morphologic defect of platelets14. Patients affected by this condition have a tendency to bleed primarily from mucous membranes, such as the conjunctiva and the lining of the nose, which can cause epistaxis (nosebleeds). They also have increased bleeding after trauma or surgery2. Disseminated intravascular coagulation (DIC) is a complex acquired syndrome where intravascular thrombi form and large numbers of platelets are consumed, resulting in thrombocytopenia15. Choroidal changes are seen most frequently with the syndrome but subretinal, retinal, preretinal and vitreous haemorrhage, haemorrhages into the iris and anterior chamber and conjunctival haemorrhages can all be observed. If these are seen in a patient with DIC, they are usually associated with terminal uraemia and septicaemia15. Valsalva’s manoeuvre Valsalva’s manoeuvre is a rapid rise in intrathoracic (abdominal) pressure, especially against a closed glottis. The pathophysiology of this process occurs because the veins above the heart have no valves. A rapid rise in the abdominal pressure induces a rapid rise in the intravenous pressure, and various vessels inside or around the eye may rupture7. Various straining activities such as heavy lifting, coughing, vomiting, blowing balloons and straining on a stool if constipated frequently lead to subconjunctival haemorrhages1,7,8. Asphyxiation also causes the neck vessels to be compressed, with a sudden increase in venous pressure and subsequent rupture of the delicate subconjunctival vessels5. Severe traumatic asphyxia may produce ocular proptosis and blue discolouration of the eyelids, face and neck, in addition to extensive subconjunctival haemorrhages. Systemic diseases Systemic hypertension is a very common cause of subconjunctival haemorrhages, especially in those over 50 years1. This type of spontaneous haemorrhaging may be the first sign of hypertension1,4. Patients with raised subconjunctival haemorrhages have been shown to have an overall higher systolic blood pressure2. Therefore, it is recommended that the blood pressure should be checked in all patients with spontaneous subconjunctival haemorrhage2,4. Other systemic diseases associated with subconjunctival haemorrhage include diabetes mellitus and hyperthyroidism1. Conjunctival conditions Figure 4 Tumours such as hemangioma or melanoma can cause a secondary subconjunctival haemorrhage that may obscure the tumour. Consider this possibility if the haemorrhage does not resolve within two weeks, or if it recurs in the same location2. Primary conjunctival amyloidosis, Kawasaki disease, which is a childhood disease characterised by an exanthemous 33 | January 27 | 2006 OT CLINICAL Exploring different causes of this condition eruption and multisystem involvement, and any of the acute conjunctivides can all result in subconjunctival haemorrhages1,13,16,17. Both viral and bacterial infections may cause small patches of haemorrhage known as ‘petechial haemorrhages’. Case 6, Figure 6 A 47-year old man with a follicular conjunctivtis and preauricular adenopathy developed a subconjunctival haemorrhage. He had a watery discharge from both eyes. He was suspected to have an adenoviral infection, which is the leading cause of viral conjunctivitis and is responsible for 5-20% of all cases of acute conjunctivitis18. Medication Any medication that can inhibit coagulation can cause subconjunctival haemorrhage. This includes the non-steroidal anti-inflammatory drugs, along with aspirin and the anticoagulants such as heparin or warfarin2. A direct metabolic relationship has been established between ingestion of a large amount of aspirin and presentation of bilateral subconjunctival haemorrhages19. vitamins, such as vitamin E (tocopherol) can also cause bleeding, especially in individuals on anticoagulant medications. Clinical evaluation For all patients presenting with a subconjunctival haemorrhage, conduct a thorough review of their history. In many instances, this history will disclose the underlying cause of the haemorrhage. A blood pressure measurement should be performed on all these patients1,2. In patients with recurrent haemorrhages, laboratory tests such as Prothrombin Time (PT), Activated Partial Thromboplastin Time (APTT) and Complete Blood Count (CBC) with platelets should be ordered to rule out serious systemic diseases2. When ordering a CBC, the laboratory will include values of the patients’ white blood cells (WBCs), red blood cells (RBCs) haemoglobin (Hgb) and haematocrit (HCT). Platelets may or may not be included and, therefore, depending on the laboratory the clinician uses, may have to be ordered separately. The normal value for platelets at the Mayo Clinic for both men and women is 150,000 to 450,000/mm3,20. Haemorrhages may be the first sign of thrombocytopenia, a condition in which a patient’s number of platelets is decreased21. The coagulation activity of a patient can be measured with additional laboratory tests. These include Prothrombin Time (PT; Protime) and Activated Partial Thromboplastin Time (APTT). These are the laboratory tests that are obtained for patients who are using anti-coagulating drugs such as heparin and warfarin. The APTT measures the activity of the intrinsic clotting mechanism (includes Factors I, II, V, VIII, IX, X, XI, and XII). Any deficiency in the intrinsic clotting system will adversely affect fibrin clot formation. A prolonged or elevated test value can result Figure 6 Case 7, Figure 7 A 77-year old man presented for evaluation of a ‘bleeding eye’. A large, elevated, diffuse subconjunctival haemorrhage was involving his left eye. A thorough medical history revealed that the patient was taking warfarin for a cardiac arrhythmia, but also started taking aspirin for his arthritic condition. It was suspected that this combination of medications was inhibiting his normal coagulation. He was advised to stop the aspirin and see his cardiologist for re-evaluation of his warfarin dosage. Certain herbal supplements may increase the risk of bleeding. These include garlic, ginger, gingko biloba and feverfew. They should not be taken in conjunction with other anti-clotting medication. Some 34 | January 27 | 2006 OT Figure 7 from excessive heparin dosing, von Willebrand’s disease, haemophilia and vitamin K deficiency2. A PT laboratory test measures for prothrombin, which is a protein produced by the liver and whose production is dependent on vitamin K. A PT evaluates the extrinsic clotting mechanism (includes Factors I, II, V, VII and X). Patients taking the anti-coagulant warfarin are routinely monitored with the PT laboratory test. Warfarin slows clotting, thereby increasing the PT by interfering with vitamin K dependent clotting factors. Other conditions that can prolong or increase a PT value include liver disease such as hepatitis, vitamin K deficiency and poor fat absorption2. Management If the subconjunctival haemorrhage is mild, monocular or is a first occurrence, often measuring the patient’s blood pressure and patient reassurance is usually all that is necessary2. The patient can also be instructed to apply cool compresses four times a day for four minutes for each application. This should be done during the first 48 hours of the haemorrhages presenting. After 48 hours, the patient can alternate between cool compresses and warm compresses3. Artificial tear drops can also be used if there is any accompanying ocular irritation3. During the time the subconjunctival haemorrhage is resolving, the patient should avoid rubbing their eye, not blow their nose and reduce any activity that would involve significant straining. References Download references from www.optometry.co.uk/references.