Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
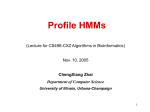
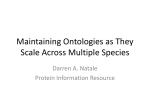
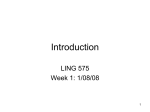
[CANCER RESEARCH 47, 5070-5073, October 1, 1987] Pharmacokinetics of Hexamethylmelamine Administration in Rabbits in Intralipid following Hepatic Regional Ian L. Gordon, Rita Kar, Richard W. Opfell,1 and Alan G. Wile2 Departments of Surgery [I. G., R. K., A. G. WJ and Medicine [R. W. O], University of California, Irvine, California 92668 ABSTRACT Hexamethylmelamine (HMM) is a cytotoxic agent demonstrated to have broad antitumor activity. Poor solubility in aqueous media has precluded significant evaluation of parenteral administration of this drug. A formulation of HMM dissolved in Intralipid has demonstrated excel lent tolerance following parenteral administration. The goal of this study was to evaluate the pharmacology of HMM in Intralipid following hepatic regional administration. The routes of administration were intraarterial via the hepatic artery with and without arterial occlusion, i.v. via the portal and jugular veins, and i.p. All animals received a total dose of 10 mg HMM/kg of body weight. Hepatic extraction of HMM was most evident via the portal vein (PV) route |AUC(PV)/AUC(i.v.) = 0.5; P < 0.05). Lower plasma levels and areas under the curve (AUCs) were observed for the hepatic artery and hepatic artery-stop flow groups when compared to i.v., but the difference was not significant. Administration i.p. yielded low plasma levels but a very long half-life (88 min). Hepatic tissue levels were highest in the group receiving HMM by the hepatic artery-stop flow route. We conclude that the HMM-Intralipid mixture is well tolerated, that HMM is extracted to a significant degree by the liver following PV administration, and that an i.p. installation of HMMIntralipid results in prolonged plasma drug levels. This preclinical study supports further efforts at evaluation of parenteral administration of the HMM-intralipid mixture. INTRODUCTION HMM3 is an S-triazine derivative which has been shown to have clinical antitumor activity against ovarian cancer (1), lymphoma (2), bladder cancer (3), and small cell lung cancer (4) and as a component of multiple drug regimens (for review see Refs. 5 and 6). Although the action of HMM is not completely understood, it appears to entail W-demethylation mediated by cytochrome P-4SO. Reactive intermediates are formed, in particular /V-methylolpentamethylmelamine (7) which forms covalent adducts with cellular macromolecules (8, 9). Multiple metabolites of HMM, including PMM and triand tetramethylmelamine, are formed as a result of A^-demethylation and can be detected in plasma after HMM administra tion (10, 11). A correlation between the degree of methylation and antitumor activity has been drawn from in vitro and animal studies, with the most methylated compounds, HMM and PMM, having the greatest activity (12). It has also been sug gested that the liberation of formaldehyde by reactive interme diates is the basis of cytotoxicity of HMM (13). HMM is poorly soluble in aqueous media except dilute hydrochloric acid, limiting its use to p.o. preparations. PMM is sufficiently water soluble for i.v. administration but has unacceptable gastrointestinal and neurological toxicity (14,15). It has recently been shown that HMM can be dissolved in 20% Received 10/17/86; revised 4/13/87. 6/30/87; accepted 7/9/87. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1Present address: Penthouse Suite, 425 East 61 Street, New York, NY 10021. 1To whom requests for reprints should be addressed, at 1(1 Medical Center, Division of Surgical Oncology, 101 City Drive South, Orange, CA 92668. ' I tu' abbreviations used are: HMM, hexamethylmelamine; PMM, pentamethylmelamine; HA, hepatic artery; HA-SF, hepatic artery stop flow; PV, portal vein; AUC, area under the curve; HPLC, high performance liquid chromatography. Intralipid, a soybean oil emulsion widely used for parenteral nutrition, and safely infused i.v. (16). As a consequence phase I clinical trials with the use of HMM dissolved in Intralipid are currently under way.4 Our interest in HMM stems from studies in animals showing a significant first pass hepatic extraction of HMM when ad ministered via the gastrointestinal tract or portal vein (17). This study raised the issue of the value of HMM in Intralipid in the therapy of primary and secondary hepatic cancer by means of regional administration. If sufficient hepatic extraction of HMM in the lipid medium could be demonstrated, then this mixture might have application analogous to the intraarterial infusion of fluorodeoxyuridine. Fluorodeoxyuridine is effi ciently extracted by the liver (18), providing for the administra tion of increased amounts of drug and increased activity against colorectal carcinoma metastatic to the liver compared to sys temic administration of S-fluorouracil (19, 20). The goal of this study was to characterize the pharmacokinetics of HMM dissolved in Intralipid and the extent of hepatic extraction in various modes of regional administration in rab bits. The routes of administration studied were intraarterial administration via the hepatic artery with and without arterial occlusion proximal to the point of infusion, i.v. administration via the portal and jugular veins, and i.p. instillation. MATERIALS AND METHODS HMM was obtained from the Drug Synthesis and Chemistry Branch, Division of Cancer Treatment, National Cancer Institute, Bethesda, MD. The HMM was dissolved at a concentration of 3 mg/ml in 20% Intralipid (Kabivitrum, Alameda, CA) at room temperature and stored at 4*C. Prior to use this mixture was filtered through Whatman No. 1 filter paper. Quantitative HPLC analysis showed that nearly 100% dissolved HMM remained in solution. Female New Zealand White rabbits (3.5 to 4.5 kg) were housed under standard vivarium conditions. Food and water were withheld for 12 h prior to drug administration. General anesthesia was induced by the i.v. injection of acepromazine (1 mg/kg; Ayerst Laboratories, New York, NY), Rompun (5 mg/kg; Cutter Labs, Shawnee, KS), and ketamine hydrochloride (50 mg/kg; Bristol Laboratories, Syracuse, NY). The right jugular vein was cannulated for the infusion of maintenance fluids. All animals received a total dose of 10 mg HMM/kg body weight. Animals undergoing i.v. administration (\ = 5) received drug through the jugular vein catheter. To accomplish portal vein administration (N = 5) the proximal superior mesenteric vein was exposed via an abdom inal incision and cannulated by puncture with a sharply beveled small caliber polyethylene tube. HA infusion ( v - 4) was achieved by exposing the celiac artery near its origin from the aorta. Direct puncture with a beveled polyethylene tube was used to cannulate the common hepatic artery. During all hepatic arterial infusions a clamp was placed across the left gastric artery to prevent egress of drug from the hepatic arterial tree. HA-SF (N = 4) was achieved by occluding blood inflow into the common hepatic artery with a second clamp proximal to the site of arterial puncture by the catheter used for drug infusion. Administration ¡.p.(N = 5) was achieved by instilling the drug directly into the peritoneal cavity through a small midline incision. A syringe pump was used to deliver the HMM-Intralipid preparation at a constant rate of 4 M. M. Ames, Mayo Clinic, personal communication. 5070 Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1987 American Association for Cancer Research. PHARMACOKINETICS 0.66 ini/min with the average infusion time being 20 min. At the end of drug infusion for all PV, HA, and HA-SF infusions catheters and clamps were removed, hemostasis at the puncture sites was achieved with temporary pressure, and blood was sampled. Blood samples were obtained via a No. 5 French catheter in the right carotid artery. Blood was collected in heparinized syringes with volu metric replacement using isotonic saline. For i.p. experiments, blood was collected at intervals up to 10 h. For other routes, sampling was performed at 5 min intervals during infusion and then at intervals up to 2 h. At the end of each experiment the rabbit was euthanized with pentobarbital i.v. and the liver was removed for liver tissue drug level determinations. Plasma was separated from blood samples in a tabletop centrifuge and stored at —20°C. Minced liver specimens were similarly stored. Drug concentrations were determined by reverse phase HPLC analysis (21). After thawing, 0.5 ml of the plasma samples was extracted twice with 1.5 ml of ethyl acetate. The organic layers were combined and evaporated to dryness under nitrogen, and the residue was dissolved in 0.25 ml methanol. The concentration of HMM in the methanol solution was analyzed by injection into a HPLC apparatus. Weighed samples of minced liver were homogenized in 0.15 M hydrochloric acid (1:6, w/v) in a Polytron tissue homogenizer (Tekmar Corporation, Cincinnati, OH). After centrifugation for 10 min at 1500 rpm, the supernatant was withdrawn. Three ml of supernatant were neutralized with 4 M NaOH and then extracted twice with 4 ml of ethyl acetate. The organic layers were pooled and processed as above. Greater than 85% recovery of HMM was demonstrated in control experiments using this technique, in accord with previous reports (22). A 0.45- x 25-cm dg Econosphere Chromatographie column (Alltech, Los Altos, CA) was used for HPLC analysis with a Beckman pump and UV detector system read at 254 nm (Models I IDA and 164; Beckman Instruments, Fullerton, CA). The solvent used was mei ha nohphosphate buffer (0.01 M, pH 7.4, with 0.01 M EDTA), 60:40 (v/v) (8), at a flow rate of 1.1 mi/min. HMM had a retention time of 18 min and could readily be distinguished from other metabolites. HMM i)uam nai ion was performed using planimetrie analysis of the area under the HMM peak with reference to a standard curve. Under these conditions a lower limit of 0.05 /tg HMM/ml in plasma was detectable. The terminal half-life and elimination constants were determined from semilogarithmic plots. Statistical analysis was conducted using Stu dents' / test. OF HMM o IQ IO 0.1 Eoi 20 40 60 TIME (min) 80 100 120 Fig. 1. Concentration of HMM in plasma for those rabbits undergoing sys temic (i.v.) infusion of HMM in Intralipid. A slow infusion of the mixture was administered to avoid acute toxicity. Samples were obtained periodically from the end of infusion (Eoi). The i.v. group demonstrated the highest peak plasma level (24.0 Mg/ml) and the largest AUC (423 MgHMM/ml x min). Bars, SD. 10 6 ÃŒ S S ; ..o RESULTS In general, administration of HMM in Intralipid was well tolerated. Preliminary experiments using rapid drug infusions encountered a high incidence of cardiopulmonary arrest similar to the experience of other investigators (23). Slower infusion rates were adopted for the remainder of the study. Figs. 1 to 4 show the plasma concentration versus time plots for i.v., PV, HA, and HA-SF groups. In general, plasma levels were near the limit of sensitivity of the HPLC assay or undetectable by 2 h after the end of the drug infusion. Fig. 5 shows the results of i.p. administration which revealed prolonged but low plasma levels in comparison to the intravascular routes. The pharmacokinetic parameters and liver tissue levels for each treatment group are displayed in Table 1. Administration i.v. resulted in the highest peak plasma levels and the largest AUC of any route. In contrast, PV administra tion yielded the lowest peak plasma level and smallest AUC of any intravascular route. PV administration resulted in a peak plasma level 39% and an AUC 50% of the values obtained following i.v. administration. The 50% decrease in the AUC represents a 50% hepatic extraction with the PV route when compared to systemic HMM administration. Significantly lower peak plasma levels, approximately 50% that of i.v. admin istration, were also seen with HA and HA-SF routes. The AUC measurements for HA and HA-SF were approximately 75% of 01 Eoi 20 40 60 TIME (min) 80 100 120 Fig. 2. Plasma concentration of HMM over time for those animals undergoing PV intusion. When compared to the i.v. group this group had a lower peak plasma level (9.8 pg HMM/ml) and the smallest AUC (211 MgHMM/ml x min) (/' < O.OS)representing significant hepatic extraction. Eoi, end of infusion. Bars, SD. the i.v. AUC, representing 25% hepatic extraction, but these differences were not significant at the 0.05 level. The distributions of HMM via the i.V., PV, and HA routes were very similar with peak plasma levels achieved at the end of infusion and a rapid clearance of drug from circulation with a terminal half-life of approximately 20 min for all three routes. This is consistent with a pharmacokinetic model in which the elimination of HMM is not altered, despite tirsi pass hepatic extraction once the drug reaches systemic circulation. With HA-SF administration the peak plasma level is achieved 2 min after the end of infusion suggesting an accumulation of drug in the liver with a washout into systemic circulation after the restoration of arterial inflow. Of interest is the observed de crease in plasma clearance of HMM with an approximate doubling of the drug half-life seen with the HA-SF route. This may represent sequestration of the Intralipid in the hepatic 5071 Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1987 American Association for Cancer Research. PHARMACOKINETICS OF HMM •K01 001 0! Fig. 3. Plasma concentration of HMM over time for those animals undergoing HA infusion. Although peak plasma HMM concentration was less than that in the i.v. group (12.8 pg HMM ml: /' < O.OS)the AUC was intermediate (298 *tg HMM/ml x min) and not significantly different from the i.v. group. Eoi, end of infusion. Bars, SD. 200 300 400 TIME (min) 500 600 Fig. 5. Plasma concentration of HMM over time for those animals receiving i.p. infusion. Although plasma concentrations were substantially lower than in those animals receiving HMM through vascular routes, drug persisted over time yielding an AUC (216 ^g HMM/ml x min) similar to that observed in groups receiving intravascular HMM. Bars, SD. 120 40 60 TIME (mm) 100 was seen with the HA-SF and was 2.5 times higher than i.v. administration results. DISCUSSION 10 io § 01 Eoi 20 40 60 TIME (min) 100 120 Fig. 4. Plasma concentration of HMM over time for those animals undergoing HA-SF infusion. Again peak plasma concentration was less than the i.v. group (12.9 /ig HMM/ml; r < O.OS)with an intermediate AUC (325 pg HMM/ml x min). It can be observed that the peak plasma level was reached shortly after end of infusion (Eoi) following release of the clamp from the hepatic artery. Bars, SD. vascular tree with washout of the mixture occurring only after restoration of blood flow. Administration of HMM i.p. yielded the lowest peak plasma level and the longest half-life. The total systemic exposure to the drug, as measured by the AUC, was reduced approximately 50% when compared to the i.v. AUC. The prolonged half-life is consistent with the Intralipid acting as a depot within the peritoneal cavity and prolonged absorption into systemic cir culation as previously reported with i.p. delivery of HMM in Intralipid in a murine model (22). When liver tissue levels were examined, HMM was not detectable in liver 10 h after i.p. administration, consistent with the short half-life of the drug in tissue (11). HA-SF, HA, and PV administration all resulted in higher tissue levels than systemic i.v. administration, although not significant at the 0.05 level. The highest tissue level, 2.17 /ugHMM/g liver tissue, The relative insolubility of HMM in aqueous solution has precluded significant clinical experience with parenteral admin istration of this drug. Administration p.o. of HMM to rats resulted in extensive drug metabolism with urinary, biliary, and fecal excretion accounting for only 0.1 % of the administered dose (24). This finding suggested that regional administration of HMM might generate substantial pharmacological advan tage due to decreased systemic drug exposure. When this po tential was investigated during portal vein and intraduodenal administration in rats, HMM was found to be extracted exten sively by the liver and bowel wall [73 and 71%, respectively (18)]. The conclusion of this study was that administration p.o. resulted in very little drug being available to come in contact with cancer cells residing beyond the liver. The realization that HMM can be administered in Intralipid in relatively high drug concentrations per volume of Intralipid has rekindled enthusiasm for regional administration of HMM. This would obviate the mucosal degradation of HMM by the gastrointestinal tract. If sufficient extraction of HMM could be demonstrated by the liver, then the combination of HMM and Intralipid when administered in regional manner may be effi cacious in the treatment of cancer involving the liver. Evalua tion of the pharmacokinetics in this preclinical model of re gional chemotherapy was the goal of this project. It was demonstrated that the greatest extraction of HMM in Intralipid was only 50% by the PV route when compared to the i.v. route. Although this difference was statistically significant it was not the 1- to 3-log difference in extraction as seen with some drugs when administered regionally to the liver. It is concluded that hepatic regional administration of HMM would be only slightly more efficacious than systemic administration but might not warrant the extra morbidity associated with regional chemotherapy. The observation that HMM in Intralipid is stable, is well tolerated in i.v. infusion, and provides a means of parenteral administration deserves further attention. In light of the low bioavailability following administration of HMM p.o. the use of the lipid vehicle combined with HMM should provide re- 5072 Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1987 American Association for Cancer Research. PHARMACOKINETICS OF HMM Table 1 Pharmacokineticparametersand livertissuelevelsfor experimentaltreatmentgroups plasma level (jig I24.0 HMM ml Routei.v. ±4.1° (N = 5) 1.6 ±1.3* i.p.(7V=5) 9.8 ±7.1* PV(JV=5) 12.8 ±8.6* HA(/V=4) 12.9 ±6.3*AUC HA-SF (N = 4)Peak • Mean ±SD. * P < 0.05 compared to i.v. route. tissue level (MgHMM/g tissue)0.84 (tigmin)423 HMM/ml x ±92 2 16 ±305 211 ±95* 298 ±205 325 ±144Hepatic newed enthusiasm for this drug. This enthusiasm should be further supported by its activity in a variety of malignant diseases. The modes of regional chemotherapy utilized in this study were intended to mimic those approaches in clinical medicine requiring a direct surgical approach or placement of a catheter by an interventional radiologist. The HA-SF mode is intended to provide access to the hepatic arterial tree by a percutaneously placed balloon-tipped catheter. Inflation of the balloon proxi mal to drug infusion is intended to retard drug washout. Pre vious experimental studies with this technique had demon strated high tissue levels of 5-fluorouracil in a dog hind limb model (25) and high tissue levels of cisplatin in a rabbit hind limb model (26). The present study is the initial evaluation of this mode of therapy in the potential treatment of hepatic disease. Although the trends toward longer drug half-life and higher tissue levels were in favor of HA-SF they did not reach statistical significance. This failure might have been overcome by enlarging the treatment groups. It is also known that the liver has a dual blood supply via the portal vein and hepatic artery. Occlusion of the hepatic artery in the normal liver should allow for continued perfusion of hepatic parenchyma by portal venous blood by means of collaterals. This portal venous blood would remove drug from the hepatic vascular tree. However, the major blood supply to hepatic tumors is by means of the hepatic artery with poorly established collaterals from the portal vein (27). It is possible that HA-SF directed at hepatic cancer would demonstrate significantly higher tumor levels of drug than those observed in normal hepatic parenchyma. Administration of HMM i.p. in Intralipid was included in this study because it might be used as a means of treating intraabdominal disease such as ovarian cancer or as a means of treating hepatic disease. Uptake of the HMM-Intralipid com bination by the peritoneal surface of the bowel would subse quently deliver drug to the liver via the portal vein. While prolonged absorption into the systemic circulation can be dem onstrated in this model it is unclear whether or not HMM can be cytotoxic without metabolic conversion. At the present time this issue remains to be resolved. REFERENCES 1. Wharton, J. T., Rutledge, F., Smith, J. P., Herson, J., and Hodge, M. P. Hexamethylmelamine: an evaluation of its role in the treatment of ovarian cancer. Am. J. Obstet. Gynecol., ¡ÌÌ: 833-844, 1979. 2. Bennett, J. M., Lenhard, R. E., Ezdinli, E., Johnson, G. J., Carbone, P. P., and Popcock, S. J. Chemotherapy of non-Hodgkin's lymphomas: Eastern Cooperative Oncology Group experience. Cancer Treat. Rep., 61: 10791083, 1977. 3. Gad, E. L., Mawla, N., Fergler, J. L., Hamza, R., Elserafi, M., and Khaled, H. Randomized phase II trial of hexamethylmelamine versus pentamethylmelamine in carcinoma of the bilharzial bladder. Cancer Treat. Rep., 68: 793-794, 1984. 4. Greco, F. A., Richardson, R. L., Snell, J. D., Shoop, S. L., and Olkham, R. K. Small cell lung cancer—complete remission and improved survival. Am. J. Med., 66:625-630, 1979. 5. Legna, S. S., Slav ik. M., and Carter, S. K. Hexamethylmelamine: an evalu ±0.22 Not detectable 1.37+ 1.45 1.54 ±1.64 2.17 ±1.87*«•*, (rain"1)0.0315 0.0079 0.0385 0.0385 0.0182Drug half-life (min)22 88 18 18 38 ation of its role in the therapy of cancer. Cancer, 38:27-35, 1976. 6. Hahn, D. A. Hexamethylmelamine and pentamethylmelamine: an update. Drug Intel!. Clin. Pharm., 17:418-424, 1983. 7. Gescher, A., D'Incaici, M., Fanelli, R., and Farina, P. /V-Hydroxymethylpentamethylmelamine, a major in vitro metabolite of hexamethylmelamine. Life Sci., 26:147-154,1980. 8. Bonn, P. J. A., Mingels, M. J., Frankhuijzen-Sierevogel, A. C, Von Graft, M., Hulshoff, A., and Noordhoek, J. Cellular and subcellular studies of the biotransformation of hexamethylmelamine in rat isolated hepatocytes and intestinal epithelial cells. Cancer Res., 44: 2820-2826, 1984. 9. ( ¡aratimi.E., Donelli, M. G., Colomiso, T., Paesani, R., and Pantarotto, C. In vivo and in vitro irreversible binding of hexamethylmelamine to liver and ovarian tumor macromolecules of mice. Biochem. Pharmacol., 30: 11511154,1981. 10. Leyland-Jones, B. R., Deesen, P. E., Casper, E. S., and Young, C. W. Specific determination of pentamethylmelamine and its demethylated metabolites in human plasma by high pressure liquid chromatography. Ther. Drug Monit., 4:185-190, 1982. 11. Broggini, M., Rossi, C., Colombo, T., and D'Incaici, M. Hexamethylmelam ine and pentamethylmelamine tissue distribution in M 5076/73A ovarian cancer bearing mice. Cancer Treat. Rep., 66:127-133, 1982. 12. Ross, D., Langdon, S. P., Gescher, A., and Stevens, M. F. G. Studies on the mode of action of anti-tumor triazenes and triazines—V. The correlation of the in vitro cytotoxicity and in vivo antitumor activity of hexamethylmelamine analogues with their metabolism. Biochem. Pharmacol., 33: 1131-1136, 1984. 13. Rutty, C. J., and Connors, T. A. In vitro studies with hexamethylmelamine. Biochem. Pharmacol., 26: 2385-2391, 1977. 14. Muindi, J. R. E., Newell, D. R., Smith, I. E., and Harrap, R. R. Pentame thylmelamine: phase I clinical and pharmacokinetic studies. Br. J. Cancer, ¿7:27-33,1983. 15. Foster, B. J., Claqqett-Carr, K., Hoth, D., and Leyland-Jones, B. Pentame thylmelamine: review of an aqueous analog of hexamethylmelamine. Cancer Treat. Rep., 70: 513-516, 1986. 16. Ames, M. M., and Kovach, J. S. Parenteral formulation of hexamethyl melamine potentially suitable for use in man. Cancer Treat. Rep., 66: 15791581, 1982. 17. Klippen. P. J. M., Hulshoff, A., Mingels, M. J., Hofman, G., and Noordhoek, J. Low oral bioavailability of hexamethylmelamine in the rat due to simul taneous hepatic and intestinal metabolism. Cancer Res., 43: 3160-3164, 1983. 18. Ensminger, W. D., Rosowsky, A., Raso, V., Levin, D. C., Glode, M., Come, S., Steele, G., and Frei, E. A clinical-pharmacological evaluation of hepatic arterial infusions of 5-fluoro-2'-deoxyuridine and 5-fluorouracil. Cancer Res., 38: 3784-3792, 1978. 19. Niederhuber, J. E., Ensminger, W., Gyves, J., Thrali, J., Walker, S., and Lozzi, E. Regional chemotherapy of colorectal cancer metastatic to the liver. Cancer (Phila.), 55: 1336-1343, 1984. 20. Baldi, C M., I risi. M. M., Soong, S., and McGregor, M. A prospective phase II clinical trial of continuous I I I)R regional chemotherapy for colo rectal métastasesto the liver using a totally implantable drug infusion pump. Ann. Surg., 198: 567-573, 1983. 21. Benvenuto, J. A., Stewart, D. J., Benjamin, R. S., Smith, R. G., and Loo, T. L. High-performance liquid Chromatographie analysis of pentamethylmela mine and its metabolites in biological fluids. J. Chromatogr., 222: 518-522, 1981. 22. Wickes, A. D., and Howell, S. B. Pharmacokinetics of hexamethylmelamine administration via the IP route in an oil emulsion vehicle. Cancer Treat. Rep., 69:657-662,1985. 23. Legna, S. S., Slav ik. M.. Livingston, R. B., and Carter, S. K. Clinical brochure on hexamethylmelamine. Investigational Drug Branch, Clinical Therapeutics and Experimental Pharmacology, National Cancer Institute, 1974. 24. Colombo, T., Broggini, M., Grescher, A., and D'Inalci, M. Routes of elimi nation of hexamethylmelamine and pentamethylmelamine in the rat. Xeno biotica, 315-321, 1982. 25. Anderson, J. H., Gianturco, C., and Wallace, S. Experimental transcatheter mi mark-rial ¡illusion<uvliisii >nchemotherapy. Invest. Radio!., 16:496-500, 1981. 26. Wile, A. G., Kar, R., Cohen, R. A., Jakowatz, J. G., and Opfell, R. W. The Pharmacokinetics of cisplatin in experimental regional chemotherapy. Cancer (Phila.), 59:695-700, 1987. 27. Breedis, C., and Young, G. The blood supply of neoplasms in the liver. Am. J. Pathol., 50:969-975, 1954. 5073 Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1987 American Association for Cancer Research. Pharmacokinetics of Hexamethylmelamine in Intralipid following Hepatic Regional Administration in Rabbits Ian L. Gordon, Rita Kar, Richard W. Opfell, et al. Cancer Res 1987;47:5070-5073. Updated version E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://cancerres.aacrjournals.org/content/47/19/5070 Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1987 American Association for Cancer Research.