Survey
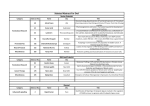
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hello. My name is Ayse Sahin. I’m a Professor of Pathology at University of Texas MD Anderson Cancer Center. I would like to review Pathology of Breast Cancer. Upon completion of this lecture, participants will be able to understand basic principles of breast pathology; integrate histopathologic features of breast cancer into clinical decision making; [and] recognize the importance of integration of clinical and histopathologic information to provide the optimal care for breast cancer patients. Breast cancer is the most common cancer in the western world. Progress has been made in the detection, diagnosis, and treatment of breast cancer. However, breast cancer still is the second leading cause of cancer death, resulting in over 44,000 deaths annually in the United States. There are many unknowns about breast cancer. The un --- the etiology of breast cancer is unknown and it seems that there are multifactorial inherited and acquired factors that cause breast cancer. I would like to discuss risk factors and multi-steps involved in breast carcinogenesis and mechanisms of invasion and metastasis of breast cancer. 90% of breast neoplasms arise from breast epithelium. So when the tumors arise from epithelium, we classify them as carcinomas and they are ri --- arising epitheliums of breast, so they are classified as adenocarcinoma. This is a diagram of breast. There are approximately six to eight branches of ductal system that open to the nipple. And in the terminal ductal lobular unit, which is the end of these branches, there is a grouping of lobules and intralobular and extralobular stroma. [A] great majority of the breast cancers are thought to arise from these terminal ductal lobular units, or they are also called as TDLU. This is the histopathologic features of TDLU. This is the main duct coming into the terminal ductal lobular unit. This is the outside stroma. And this is the inside stroma which is supporting the acini. In higher magnification of a normal lobule, show that in each acini,… … there are two types of cells – the peripheral cells, these are myoepithelial cells, and the acinar cells or ductal cells. Breast cancer is a heterogenous disease. It’s a heterogeneous disease based on microscopic appearance, biological features, and clinical behavior. There are different types of breast carcinomas. The main classification of breast carcinoma is ductal and lobular carcinoma. And among invasive carcinomas there are different types of histologic cancers. Again, this is the chest wall and here is the nipple. And these are the nipple ducts going into the terminal ductal lobular units. First, I would like to start with in situ carcinoma. In situ carcinoma used to be a rare disease prior to mammographic screening. In 1970s to 1980s when the mammographic screening became more common, DCIS used to make less than 1% of all newly diagnosed breast cancers. In the mammographically screened populations today, DCIS comprises up to 40% of newly diagnosed breast cancer. Among non-screened populations, it is today 5-10% of all breast carcinomas. Screened populations, this is 25-30%. And among the screened detected cancers, it can make up all --- up to half of newly diagnosed breast cancer. In terms of classification of DCIS, in the past, we had this traditional classification system as comedocarcinoma and non-comedo DCIS. And under non-comedo DCIS, we --- we had different histopathologic features. But, today, we classify DCIS based on mainly grade of the nuclei as high grade, intermediate grade, and low grade. This is an example of low grade ductal carcinoma in situ, cribriform type; and this tumor is associated with microcalcifications. This is an intermediate grade ductal carcinoma in situ, again, associated with microcalcifications. In this case the nuclei are a little more pleomorphic and there is an intraductal comedo-type necrosis indicating that this is a higher grade tumor. And this is high grade DCIS. Again, it’s associated with microcalcification. But compared to previous two cases, nuclear pleomorphism is significant, and there are scattered mitosis. In addition to comedonecrosis, there is also individual cell necrosis. So, this is a high grade DCIS. In terms of natural history of DCIS, we know that it progresses to invasive carcinoma and the progression rate depends on grade. A high grade DCIS takes a lot shorter to progress into invasive carcinoma. And low grade DCIS may or may not progress to invasive carcinoma but when it progresses to invasive carcinoma, it usually takes a lot longer to progress. In terms of treatment of DCIS, we pay attention to histopathologic features which include grade of the tumor, size of the tumor, margin status of the excised specimen either on a segmental resection or mastectomy, and expression of hormonal receptors, namely estrogen receptor and progesterone receptor. Paget’s disease is a form of DCIS. Up to 60% of the patients with Paget’s disease will have [an] underlying mass and in situ carcinoma. Prognosis and therapy depend on [the] underlying carcinoma. So when we make the diagnosis of Paget’s disease we always look for an underlying lesion. And the therapy will depend on if there is any invasive or in situ carcinoma. This is an example of Paget’s disease with an ulcerated lesion. Here is the part of the nipple. The rest of the nipple is destroyed by this lesion. The second type of in situ carcinoma is lobular carcinoma in situ and comp --- in contrast to lobular car --- ductal carcinoma in situ, lobular carcinoma in situ is characterized by stereotypical morphology, very uniform cells involve acini or lobules, and they distend these involved acini. In majority of the cases lobular carcinoma in situ is an incidental finding. Lobular carcinoma in situ, as we understand [it] today, is both precursor lesion and it’s a risk marker. Patients with lobular carcinoma in situ have 1% per year risk for developing subsequent invasive carcinoma. And in [the] case of lobular carcinoma in situ, the risk is at same at the both breasts. Ductal carcinoma in situ, we feel that it is a precursor lesion and the risk is in the same breast. But for lobular carcinoma in situ, both breasts are at the same risk. This is an example of lobular carcinoma in situ. Monotonous uniform cells involve lobular units and acini, and they expand acini. And the expansion is pretty uniform and symmetrical. Higher magnification: the nuclei are very uniform. hypochromatic nuclei and the nuclei are evenly spaced. They have these round When we move to the invasive breast cancer: Again, invasive breast cancer is a very heterogenous group of tumors. Even though we discuss, in general, breast cancer as if it is a single disease, there are many different types with different biologic and clinical outcomes. 75-80% of invasive carcinomas are classified as invasive ductal carcinoma or invasive carcinoma not otherwise specified. 20-25% of invasive carcinomas are special types. They have special morphologic features and they have --- these special types have different clinical outcomes. Classification is based on morphologic features. Histopathologic categorization is based on two things: one is histopathologic type; the second is grade. WHO recognizes 17 different types of breast carcinomas based on morphologic features. As I indicated before, invasive ductal carcinoma is the largest category comprising more than 80% of the tumors. The second common type is invasive lobular carcinoma. And then we have these special types including tubular, cribriform, mucinous, and less commonly, invasive papillary, micropapillary, medullary, and metaplastic carcinomas. Majority of the times, invasive ductal carcinoma can have other types of carcinomas associated with it. In a pure form, invasive ductal carcinoma comprises approximately 55% of tumors but when you are mixed with other carcinomas, it is the largest category. Invasive lobular carcinoma is approximately 10% and the other types are quite rare. Many of the other special types are listed at special category and when the tumor does not fit in any of the special category then we call it as invasive ductal carcinoma. Because of that, tumors not otherwise specified or tumor no special type is also used to describe ductal carcinoma. Scirrhous carcinoma is a term used in the literature to indicate… … that the tumor is firm and it is very fixed to the adjacent breast parenchyma. This is a gross picture of an invasive carcinoma, scirrhous type, and these white, chalkyappearing tissue infiltrate into adjacent breast parenchyma. And on palpation this feels extremely firm. And this firmness is usually due to desmoplastic reaction that the infiltrative carcinoma cells elicit. Here is the example of desmoplastic reaction, which appears to --- blue to pink-appearing stroma in reg --- routine H&E stain sections. Here is adipose tissue, and [the] desmoplastic reaction go into the adjacent stroma. This is an example of invasive lobular carcinoma which is characterized by infiltration of single cell types associated with stromal collagen. And one characteristic feature of invasive lobular carcinoma is that as tumor cells infiltrate into adjacent stroma, they may leave normal breast glands intact. This is an important clinical feature because having these reg --- routine --- normal ducts left behind, the tumor may not be felt as a firm mass on palpation. Similarly, on imaging findings, we may underestimate [the] size of invasive lobular carcinoma. In contrast, this is an invasive ductal carcinoma. Tumor cells are making these glandular spaces. And as they infiltrate, they cause this desmoplastic reaction which can cause palpable mass. And at the same time, on imaging modalities, this desmoplastic stroma can easily be seen. So the determination of tumor size on imaging is a lot more accurate for invasive ductal carcinoma. This is another example of invasive carcinoma. Histologic classification of breast carcinoma in relation to prognosis is based on a patient’s outcome. Breast carcinomas are classified into good prognosis, intermediate, and poor prognosis categories. And the good prognosis category includes tubular carcinoma, invasive cribriform carcinoma, and mucinous carcinoma. Intermediate prognosis category includes medullary invasive lobular carcinoma. Poor prognosis category includes metaplastic, signet-ring, inflammatory, and lipid-rich carcinoma. It is important to recognize these good prognostic category tumors because compared to invasive ductal carcinoma, cribriform, tubular, and mucinous carcinomas, [they] have significantly better clinical outcomes. Invasive ductal carcinomas can show wide morphologic features including cords, nests, ducts, anastomosing tubules. And they also have different cytologic details. In addition to morphologic features, there are additional histopathologic features such as lymphatic invasion, perineural invasion, blood vessel invasion, necrosis, and [the] number of mitosis which also are important in prediction of outcomes of invasive ductal carcinoma. Invasive lobular carcinoma is the second most frequent types of invasive carcinoma, constituting 5-10% of all breast carcinomas. They have [a] higher frequency of bilaterality and multicentricity. Often invasive lobular carcinomas show [a] diffuse infiltration pattern. And they most frequently metastasize to serosal surfaces, ovaries, central nervous system, and bone marrow. Invasive lobular carcinomas are characterized by low grade nuclear features. They are usually estrogen/progesterone receptor positive. And they lack [the] cell-to-cell adhesion molecule E-cadherin. And they are characterized by this single cell infiltration pattern. High magnification: the single cells are shown here. When we look at the molecular and genetic features of invasive lobular carcinoma, they are very similar to low grade ductal lesion. And the main distinction between invasive ductal and invasive lobular carcinoma is that lobular carcinomas lack E-cadherin expression due to genetic and epigenetic changes in the CDH1 gene which is located on Chromosome 16. E-cadherin is the critical cell adhesion molecule and the loss of Ecadherin is reflected at the morphologic level by the discohesive nature of individual cells and overall growth pattern. E-cadherin can be evaluated by immunohistochemistry, shown in this slide, and [the] typical membranous staining pattern. Medullary carcinoma is an important category, although it is a con --- it constitutes only 4-5% of all breast carcinomas. Among patients who are BRCA1 gene carriers, they can constitute up to 15% of the carcinomas. And it is important to recognize this category, especially among young patients. Medullary carcinomas are characterized by lack of desmoplasia. These tumor cells grow in a sheet-like fashion. Histologically and grossly it forms this circumscribed mass and the tumor cells are always high grade. This is an example of medullary carcinoma forming this well-circumscribed mass. And histopathologically, it’s a high grade tumor of significant pleomorphism associated with lymphoplasmacytic infiltrate. Colloid carcinoma occurs in older patients, grows slowly. These tumors are characterized by low tumor grade. And they --- they are estrogen and progesterone receptor positive. Colloid carcinoma is one of the best prognostic category invasive carcinoma. Survival rates of patients with colloid carcinoma [are] significantly better. And lymph node metastasis is usually less common. Colloid carcinoma is also called mucinous carcinoma. And it has this gelatinous gross appearance due to extensive mucin. This is the histologic picture of a colloid or mucinous carcinoma. Tumor cells float in this mucinous material. Tubular carcinoma is another good prognostic category tumor. It used to be a rare tumor. But among mammographically detected carcinomas, it can make up --- up to 20% of carcinomas. Tubular carcinomas have excellent prognosis. They are ER/PR positive and [the] majority of tubular carcinomas are diploid tumors. Here is an example of tubular carcinoma, characterized by these infiltrating glands with open lumina and irregular edges. Invasive cribriform carcinoma is also a rare tumor but has [an] excellent prognosis. This is also a well-differentiated carcinoma characterized by these small tubules and cribriform complex structures infiltrating into stroma. In terms of grading of tumors, there are different grading systems, using either nuclear features of --- or architectural features. And there are different levels in each grade. Unfortunately, there is a significant inter- and intra-observer variation. In terms of architectural features, we look for tubule and gland formation. In terms of cytologic features, we look at the nuclear size and nuclear pleomorphism. In terms of grading systems, in general, whatever grading it is used, Grade 1 tumors always have better outcomes, compared to Grades 2 and 3 tumors. And Grade 3 tumors have significantly worse outcomes than other grades. But depending on which grading system is used and what type of cutoff point [is] used, there might be significant overlap between Grade 2 and Grade 3. This is an example of low grade tumor infiltrating ducts and not significant cyt --cytologic atypia, ---in contrast to this tumor which has significant nuclear atypia. Regardless of grading, stage is the most important prognostic parameter of invasive carcinoma regardless of histologic type and grade. Therefore, in a pathology report, we should report the TNM staging as accurately as possible. In the TNM staging, T stands for primary tumor; N stands for regional lymph nodes; M stands for distant metastasis. Pathologic tumor size is the size of [the] invasive carcinoma before any tissue is removed for special studies. If multiple core biopsies are performed, [the] original tumor site should be reconstructed on the basis of combination of imaging and histologic features. Tumor size can be evaluated based on clinical findings, imaging, or pathologic. But pathologic tumor size is the most accurate size to correlate with clinical outcome. If a tumor is [a] well circumscribed mass like this. This happens to be a medullary carcinoma that --- I showed before – a gross measurement with a ruler is an adequate assessment. However, if the tumor is non-palpable, in this case of invasive lobular carcinoma, here is the biopsy site. We know the tumor is here. But, as I indicated before, invasive lobular carcinomas do --- sometimes do not form a mass. That they are diffuse and they do not elicit desmoplastic reaction. In this case, this entire region is involved by invasive lobular carcinoma. But, this is very difficult to appreciate on this gross evaluation. Therefore, we recommend specimen x-rays in addition to gross appearance of the tumor to assess the extent of the tumor. In this case, here is the nipple, here are the skin edges. And there is an invasive lobular carcinoma extending [from] this resection margin. And here is the corresponding specimen x-ray showing invasive carcinoma. When we are evaluating tumor size, if there are more than one foci of invasive lesions, then we see if there is a connection between these foci. In this diagram, this ragged, red areas is representing invasive carcinoma. And these blue circles are representing in situ carcinoma. And the yellow circles are representing normal breast parenchyma. In this case we would measure invasive carcinoma from this end to this end of invasive focus. If there are two invasive foci connected by in situ carcinoma, from one edge of invasive to another invasive edge, we will consider the invasive focus. If there are multiple foci of invasive carcinoma all connected with DCIS, we will include the in situ carcinoma with an invasive foci in determination of the tumor size. But, if there are two separate foci of invasive cancer separated by normal breast parenchyma, then we say this is a multiple focal invasive tumor and for staging purpose, we report the largest size of invasive carcinoma. We do not add up these tumors. So, if there are simultaneous bilateral breast carcinomas, each carcinoma is staged separately as primary tumors. If there is an inflammatory carcinoma, the definition is --- should be done based on clinical pathologic features, which is diffuse erythema and edema of breast. Inflammatory carcinoma is often without [an] underlying palpable mass. Imaging studies show skin thickening with or without mass. And biopsy should show lymphatic invasion by tumor. This is a patient with inflammatory breast carcinoma, presented with diss --- diffuse redness of the breast without any palpable mass. Lymph node status is the most important prognostic parameter of the invasive breast carcinoma. It can be assessed by different methodologies. And histopathologic evaluation is the most accurate method. [The] number of lymph nodes involved in an invasive carcinoma is directly associated with both [the] five-year and ten-year outcomes of breast carcinoma. When we have [a] full axillary lymph node dissection, we look at [the] number of lymph nodes with metastatic carcinoma, size of the largest metastasis, and presence and absence of extranodal extension. And if there is extranodal extension, we measure the size of extranodal extension. We utilize immunohistochemistry for cytokeratin to identify and sometimes to assess the extent of metastatic carcinoma. Here is a lymph node. And this is a keratin immunohistochemical staining for cytokeratin, highlighting the metastatic carcinoma foci. In this case, it’s a single focus. And here, it’s multiple tumor cells distributed throughout the lymph nodes. Hormone receptor status is another important prognostic and predictive factor of invasive carcinoma. And it should be evaluated in each newly diagnosed breast cancer. This is an example of immunohistochemical staining for estrogen receptor showing strong positivity in the tumor’s nuclei. Another important prognostic and predictive marker occurs, and now it is a therapy target, is HER-2/neu protein which is --- a HER-2/neu gene is located on Chromosome 17. And overexpression and amplification of this gene is associated with poor prognosis. In addition to HER-2/neu, there are number of other prognostic factors and predictive factors in breast carcinoma. And the most important thing is that when we are evaluating these prognostic factors, they need to have a clinical indication. And right now with all the targeted therapy options, some of these prognostic and predictive markers have targetable therapy options. On a molecular level invasive carcinoma is, again, a very heterogenous disease. And if you look at the gene expression profiles, the heterogeneity of breast cancer is evident, just like [the] morphology and immunohistochemical features of breast carcinoma. The most important categorization of breast cancer on [the] molecular level is [the] estrogen receptor. These are estrogen receptor positive tumors and estrogen receptor negative tumors. And [the] clinical outcomes of these tumors are significantly different. So, in summary, the role of pathology is not only to establish diagnosis and classify tumor but we have to provide accurate information on staging. And we have to evaluate prognostic and predictive factors. Breast cancer is the most common malignancy in women. Histopathologic features have significant impact in [the] biology of breast cancer and need to be incorporated in clinical therapy decisions. Tumor size, axillary lymph node status, and biologic marker expression, estrogen receptor, progesterone receptor, and HER-2/neu need to be evaluated for all newly diagnosed breast cancers. Thank you very much for your attention. And we would welcome all your feedback.