Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
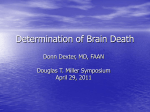
Jornal de Pediatria - Vol. 77, Supl.1 , 2001 S97 0021-7557/01/77-Supl.1/S97 Jornal de Pediatria Copyright © 2001 by Sociedade Brasileira de Pediatria REVIEW ARTICLE Neonatal apnea José Maria de Andrade Lopes* Abstract Objective: to review medical literature related to apnea of prematurity. Sources: extensive literature search and clinical practice-oriented concepts. Summary of the findings: apnea is one of the most common respiratory disorders in the neonatal period. Immaturity of the central nervous system is associated with instability of respiration. Therefore, apnea manifests itself in other systems, causing problems such as hypoglycemia, hypothermia, infection, or patent ductus arteriosus. Apnea may be central, obstructive or mixed depending on the presence of air flow through the upper airways. Diagnosis should involve careful observation by unit personnel and the monitoring of heart rate, respiratory frequency or arterial oxygen saturation. Initially, the treatment consists of xanthines (caffeine and aminophylline). If respiratory failure occurs, then continuous positive airway pressure (CPAP), and mechanical ventilation should be used. Conclusions: preterm newborns are susceptible to respiratory problems, having apnea as a clinical manifestation of disorders in many organs and systems. J Pediatr (Rio J) 2001; 77 (Supl.1): S97-S103:apnea, prematurity, respiration. Introduction Apnea is the most frequent type of breathing disorder in the neonatal period.1 During the past few years, the use of artificial surfactants, of new technologies, and the progress in neonatal care have allowed for a considerable increase in the survival of newborn infants with less than 1,500 grams and, consequently, in the population at risk for apnea. 2 Most of the times, apnea is an isolated event, but that can put the newborn’s life at risk if not promptly diagnosed and adequately treated. Exceptionally, severe apnea affects term newborn infants, but it is common in newborns with less than 2,500 grams. In this paper, we will discuss basic concepts and practical aspects of the treatment of apnea in newborn infants. Definition and concepts The definition of apnea has been changing in the past years due to new findings on its physiopathology. Initially, apnea was defined in terms of respiratory movements. Cessation of respiratory movements of 5, 10, 20, or 30 seconds’ duration have been used to define apnea. Most authors agree that episodes of any duration followed by bradycardia and/or cyanosis are considered pathological.3,4 It is important to underscore that the more immature the newborn, the greater the irregularity of respiration and the * Chief, Department of Neonatology, Instituto Fernandes Figueira, FIOCRUZ. Member, Perinatology Committee, Brazilian Society of Pediatrics (SBP). S97 S98 Jornal de Pediatria - Vol. 77, Supl.1, 2001 number of episodes of apnea without bradycardia and cyanosis, and with spontaneous recovery. Particularly during REM (Rapid Eye Movement) sleep, apneic spells with 10 to 15 seconds’ duration are very frequent.5 Alternately with episodes of periodic respiration, others have also reported apneic spells lasting 5 to 10 seconds without physiological consequences (see next section). The definition of apnea based on respiratory movements is incomplete, and that is because even during active respiratory movements there may be an obstruction of the upper airways and a cessation of gas exchange. This condition is known as obstructive apnea (Figure 1). Central apnea - total cessation of respiratory movements, and consequent cessation of airflow in the upper airways. Obstructive apnea - cessation of airflow in the upper airways in the presence of active respiratory movements. Mixed apnea episode of central apnea followed by obstructive episode (respiratory movements without airflow in the airways) or obstructive episode followed by central apnea. Figure 1 - Classification of neonatal apneas In this sense, apnea is currently defined as the cessation of airflow longer than 5 seconds in the upper airways. Apnea is pathological and, independently of its duration, it is followed by bradycardia and cyanosis. It is interesting to underscore that as a general rule, obstructive apneas lead to earlier bradycardia. Central apnea rarely presents hemodynamic consequences if it lasts less than 20 seconds. Predisposing factors We will discuss two of these factors, firstly, respiration control and, secondly, sleep and alterations of thoracic cavity. Respiration Control Respiration control in newborn infants is the focus of extensive research projects carried out worldwide due to the differences in relation to adult patients. Neonatal apnea - Lopes JMA The response to hypoxia is paradoxal.6 While in adults patients hypoxemia stimulates breathing, in newborn patients the response is diphasic, initially with hyperventilation and followed by ventilatory depression. One of the possible causes of post-hypoxia depression in newborns is the release of adenosine to the central nervous system. Adenosine is a nitrogen base produced with breakdown of adenosine triphosphate (ATP) during hypoxia. Its effects can be blocked by xanthines (caffeine and teophylline). Xanthines are adenosine receptor antagonists. Lopes et al. 7 studied the role of adenosine in newborn piglets. The authors concluded that pretreatment with xanthine abolished the ventilatory depression associated with hypoxia.7 The diphasic response to hypoxia can deteriorate cases of neonatal apnea because patients will enter an endless cycle of apnea-hypoxia-apnea, which leads to worsening of ventilatory depression.6 The response to hypercapnia is still controversial. Some authors consider that the response is similar to that of the adult; whereas others insist that, at least during the first days of life, the response is depressed. In very low birth weight newborns (less than 1,500 g), studies have reported a reduced sensitivity to CO2, which improved with increase in gestational age.8 The most important aspect of respiration control is that there is a poor neuronal organization. The more immature the newborn infant, the more immature the central nervous system, with reduced synapses and dendritic branches.9 Physiologists tend to define the respiration of the newborn as a sensory and motor experience extremely dependent on the quantity and quality of sensory afferent stimulation. This concept is based on the facts that simple alterations of room temperature (hypo and hyperthermia) can, sometimes, cause apnea; physical or sensory stimulation are capable or reverting clinical status of apnea; hypoglycemia is frequently associated with apnea; and apnea itself is, at times, the most common symptom in the presence of infection, anemia, or metabolic disorders.10 Consequently, if, on the one hand, there are more exciting stimuli than grating stimuli, breathing will continue. If, on the other hand, there are more grating stimuli, apnea will occur. Sleep and alterations of the thoracic cavity Sleep will determine important changes in the respiration of the newborn infant. There are basically two types of sleep, non-rapid eye movement (NREM) and rapid eye movement (REM). As soon as we fall asleep we enter the NREM stage. This stage is characterized by regular breathing, broadband waves, low-frequency EEG, and no REM for a duration of 15 to 20 minutes (EEG indicating rapid, low-voltage waves). These two stages are repeated Neonatal apnea - Lopes JMA Jornal de Pediatria - Vol. 77, Supl.1 , 2001 S99 during sleep in the NREM-REM sequence. Adults will have approximately 80% of their sleep in NREM. Conversely, premature newborn infants with less than 32 weeks will have approximately 80%of their sleep in REM.4,11 Table 1 - Factor Possible mechanism During sleep, the REM stage is characterized by irregular breathing with intermittent respiratory pauses and apneas. During this period of sleep, there is a central inhibition of all postural muscles inducing a generalized muscle hypotonia. Among the muscles affected there are the inspiratory intercostal muscles, which keep the thoracic cavity together. Near atonia of these muscles will lead, consequently, to distortion of the rib cage during inspiration causing what is called paradoxical inspiratory motion of the abdomen (abdominal paradox). This distortion will result in an increase in the work done by the diaphragm, which will have to contract more in order to maintain adequate levels of ventilation (see below fatigue of the diaphragm).12,13 PDA Hypoxia and/or muscle fatigue Anemia Hypoxia Hypoglycemia Central, lack of substrate to respiratory muscles Hypocalcemia Central, lack of substrate to respiratory muscles Infection Hypoxemia? Increased metabolic rate, central inhibition Prematurity CNS immaturity, muscle fatigue Thermal instability Inhibitory afferent stimulation Intracranial pathology Direct effect on respiratory centers The lung volume at rest (functional residual capacity = residual volume + expiratory reserve volume) is 30% lower in REM sleep in relation to that of NREM sleep.24 According to some authors, this fact, in addition to the alterations to the thoracic cavity, is responsible for the fall of approximately 10 mmHg in TcPO2 (transcutaneous PO2) during REM sleep.14 It is a known fact that a small grade of hypoxia can be the cause of apnea; in this sense, this condition can be easily reverted with the newborn being administered oxygen at 25%. Gastroesophageal reflux Inhibitory reflex concerning upper airways Drugs CNS depression Another important aspect related to sleep is muscle tonus. It is understood that muscle tonus is reduced during sleep and there is a near state of atonia in REM sleep. This hypotonia also affects the upper airway muscles, and it is responsible for a significant increase in lung resistance and in respiratory work.15 Currently, it is understood that maintaining airways permeable depends on a perfect respiratory, pharynx and larynx muscles coordination. These muscle groups contract in synchrony during inspiration. The generation of negative airway pressure by the respiratory muscles, in normal situations, should be counteracted by contraction of upper airway muscles. One of these muscles, which is widely studied even in newborn patients, is the genioglossus (GG). Contraction of the GG will set the tongue in the anterior position, avoiding contact with the posterior wall of the pharynx. Lack of contraction of this muscle, consequently, will almost always result in obstructive apnea. In 1987, Carlo et al. detected obstructive episodes related to unsynchronized GG and diaphragm.17 Etiology The mechanisms through which different factors are related to the occurrence of apnea are not entirely established. Table 1 presents a relationship between some of the possible physiological mechanisms involved. Factors related to the occurrence of apnea, and some possible physiological mechanisms involved For a long time neonatologists and physiologist have been in search for an explanation for occurrence of apnea. It is neither understood why newborns stop breathing nor why once it has stopped most of these babies do not resume regular breathing. These are classical factors reported in the literature as to the occurrence of apnea. Often, when the related pathologies are treated, apnea will improve or disappear completely. However, there are many cases of newborn infants whose apnea does not present a related cause; these cases are called idiopathic apnea. 1,10 Recently, at the Instituto Fernandes Figueiras, a study was carried out on the risk factors for neonatal apnea in newborns with less than 1,500 g. Out of a total 63 newborns who survived until 1 year of age, 32 presented apnea at some point and that required treatment, and 10 presented severe and recurring apnea. The average weight of newborns with apnea was of 1,124 g, whereas in those without apnea it was of 1,270 g. The incidence of apnea was inversely proportional to gestational age/weight. Results indicated an incidence of 90% in patients with less than 1,000 g and of 43% in those between 1,000 and 1,500 g. The relative risk for apnea did not differ for type of delivery, sex, sepsis, intracranial hemorrhage, and bronchopulmonary dysplasia. However, results also indicated that the relative risk for apnea was of 1.73 (1.13 - 2.66) in patients with weight appropriate for gestational age as compared to those small for gestational age; and of 2.58 (1.16 - 5.74) in patients with hyaline membrane disease as compared to those without hyaline membrane. These data corroborate the international literature in the sense that risk for apnea is greater in small, appropriate for gestational age newborns and in situations of posthyaline membrane disease.18 S100 Jornal de Pediatria - Vol. 77, Supl.1, 2001 In a different study carried out in Canada, we indicated that approximately 30% of the so-called idiopathic apneas may actually be a consequence of respiratory muscle failure.12 The increase in respiratory work associated with increased rib cage compliance will put the premature newborn infant at risk for muscular fatigue. Moreover, the respiratory muscles (especially the diaphragm) of these babies are not well-developed, and present poor differentiation and low enzymatic capacity. Keens et al. showed that the percentage of muscle fibers with great oxidizing capacity (type 1 fibers) in the diaphragm is reduced at 32 weeks. Adult percentage levels are attained only at approximately one year of age.19 During the 1980s, studies with adult patients provided information on the possible occurrence of diaphragm fatigue in premature newborns. Chronic alcoholic, phosphorusdepleted patients with serum levels below 40 mg% were removed from the ventilator as soon as plasmatic phosphorus was corrected.20 In this sense, it is known that hypophosphatemia is common in premature newborns, especially in those with birth weight less than 1,500 g and with history of respiratory disease and parenteral nutrition. Human milk lacks adequate phosphorus (P) content. Parenteral feeding of P usually follows a fixed calcium:P ratio which affects the intake of P. Currently, at various centers worldwide, the administered intake of calcium and phosphorus is much higher than that provided by human milk. The supplementation with calcium and P is aimed at preventing rickets of prematurity. The increased intake of these minerals will certainly bring benefits to the respiratory muscle function if normal levels of P are delivered to the patient. Another mechanism of apnea - which is not widelydiscussed in the literature but is frequent in very low birth weight newborns - is the reduction of functional residual capacity. Newborns with birth weight less than 1,000 grams, and who do not present severe pulmonary disease on the first days of life can frequently maintain a regular respiratory rhythm in the first few days of life. In this case, apnea appears, in general, after the third day of life. Based on indirect evidence only, it is believed that functional residual capacity decreases progressively with repetitive collapse and reexpansion (this can be verified with chest X-rays). This situation will lead the newborn patient to hypoventilation, increase in oxygen requirements, and apnea. Usually, these cases of apnea are severe enough to require intubation and assisted ventilation. Diagnosis Apnea can be diagnosed as obstructive, mixed, or central and also according to the etiology. In order to correctly diagnose the type of apnea, it is necessary to use a polygraph to register movements of the thorax and abdomen, and to register airflow in the upper airways. In turn, direct and careful observation by doctors and nurses for periods of 15 to 20 minutes can allow for an approximate clinical diagnosis. Neonatal apnea - Lopes JMA In a different study with a population of 20 newborns with apnea, we showed the predominance of central episodes in newborn infants without intracranial hemorrhage. 13 As to what concerns the etiology of episodes of apnea, it is necessary to be on the look for the related factors, as described above. Figure 2 presents the general diagnostic guidelines. 1. In-depth clinical examination(auscultation of the heart, and pulse rate); 2. Environmental conditions(temperature, necessity of oxygen therapy, and positioning of the newborn); 3. Dextrostix, Multistix, Hematocrit; 4. Sodium, potassium, calcium, magnesium; 5. Hemogram + mini VHS (Screening for sepsis, as indicated); 6. Blood gas analysis; 7. Chest x-ray; 8. pHmetry of the esophagus or radiological screening for reflux; 9. Transfontanelle ultrasonography. Figure 2 - General guidelines for the diagnosis of apnea Treatment General guidelines Most services adopt a criterion for the beginning of treatment for apnea. We indicate intervention when three or more episodes requiring resuscitation and bag-mask ventilation occur within 24 hours. Mild apneas with slight cardiovascular complications and that require only physical stimulation are usually directly observable. In these cases, the most important measure is to monitor the newborn and adequately register the number, the duration, and the types of episodes. Before beginning the treatment it is important to try to establish an etiologic factor according to the discussion above. When an etiologic factor is not identified, the apnea is idiopathic and there is no question whether treatment should be started. But if the diagnosis of apnea is related to neonatal infection, the anti-infection therapy will not bring, as a rule, immediate results. The question that remains is whether it would be best to start pharmacological treatment even considering that it is a case of infection; or whether it Neonatal apnea - Lopes JMA would be best to submit the patient to mechanical ventilation until the infection gets better. This question is still to be answered. The routine procedure at the Instituto Fernandes Figueira is to treat only non-idiopathic apneas if the clinical status of the patient is suggestive of rapid reversal of the symptomatology. Newborn infants with apnea following intracranial hemorrhage or with apnea following severe infection require, first and foremost, that the baseline disease be treated. Treatment - basic principles a) correct metabolic disorders or other intercurrent pathologies and check environmental conditions b) eliminate neonatal infections c) register episodes appropriately, indicating duration, type, frequency, and physiological consequences d) establish treatment criteria - 3 episodes in 24 hours that require bag-mask ventilation Metabolic disorders and environment Considering what we presented in the above section, it is important to note that careful screening should be carried out in order to correct the most frequent metabolic disorders. Control of temperature is also critical in these situations. Hypo- and hyperthermia can be easily corrected with adequate temperature adjustments of the newborn’s surrounding environment. It is recommended to register the thermal curve simultaneously with the temperature of the newborn and of the incubator in order to check the efficacy of these measures. Together with the assessment of environmental conditions, it is also important to check the position and the neck flexion of the newborn (cause of obstructive apnea). Moreover, it is also important to check for upper airway obstruction and to ensure patent airways. Neonatal infection Unfortunately, neonatal infection is still very common. Hence, all efforts should also be directed towards eliminating or treating this type of infection, if it is the case. Apneas are frequent and difficult to revert in cases of severe infection, thus compromising the overall clinical status of the newborn. According to our experience, infection/sepsis has been the most frequent cause for indication of mechanical ventilation in premature newborn infants. At our services, mechanical ventilation is indicated in these cases since we know that clinical status of severe infections last 48 to 72 hours, and that apneas rarely improve before 72 hours. Apnea and gastroesophageal reflux The occurrence of apnea related with gastroesophageal reflux is still a focus of discussion in the literature. 21,22 In some cases, there is a clear relation between administration Jornal de Pediatria - Vol. 77, Supl.1 , 2001 S101 of diet and episodes of apnea, which can be verified with continuous esophageal pH-metry. In other cases, the pHmetry will indicate the reflux and the newborn will have an episode of apnea, but the two episodes are not time-related. In cases of apnea provenly related to reflux, it is recommended that specific treatment observing posture, diet, and administration of prokynetic drugs be carried out. Registering episodes of apnea Following the indication of an episode of apnea, it is important to characterize and register episodes adequately. It is important to register the number of episodes that occurred within a 24-hour period, the duration of each episode, the complications (bradycardia or cyanosis) and if they were related to any procedure (airway aspiration or feeding) or to position of the baby, and the maneuvers required to reverse the situation. Careful observation of the newborn in the incubator may not indicate the type of apnea. Bradycardia can be often observed in newborns who are apparently breathing normally (active thoracic movements); hence, this is clearly an obstructive episode. If the episodes can be reverted with adequate positioning of the baby or changing decubitus, this indicates that they may be related to upper airway obstruction. Criteria for beginning treatment We apply the criterion of occurrence of 3 or more episodes, within 24 hours, requiring resuscitation and bagmask ventilation for the indication of intervention. Usually, patients with apneas with 20 seconds duration or less, that revert spontaneously or with slight physical stimulation, and with mild cardiovascular complications can be simply indicated for observation. In these cases, the most important measure is to monitor the newborn and register the number, duration, and type of episodes. Therapeutics Physical stimulation Physical stimulation or repeated stimulation (kinesthetic stimulation) are recommended in cases of mild apnea. Other services have reported the use of oscillating mattress as a form of repeated stimulation. This method was carried out placing a disposable glove under the mattress and connecting the glove to a ventilator, which is set at a low frequency (5 to 10 minutes) for slight and intermittent stimulation. This method has been reported efficient in a number of cases.23,24 For severe, frequent apnea, we present 3 alternatives to be considered: – pharmacological treatment; – continuous positive airway pressure - CPAP; – mechanical ventilation. S102 Jornal de Pediatria - Vol. 77, Supl.1, 2001 Pharmacological treatment The drug of choice is the teophylline. An initial dosage of 6 mg/kg followed by a maintenance dosage of 4 mg/kg/ day divided in three doses is indicated. Dosages can be administered either orally or endovenously since the absorption of the drug is excellent. Thirty minutes after administration of the drug, adequate plasmatic levels can be detected, which can produce a therapeutic response. It is important to monitor plasmatic levels 2 or 3 days after treatment because the half-life of teophylline in newborns varies considerably.23 Collection of blood samples pre- and postxanthine treatment (30 minutes before and after) will provide good information on minimum and maximum plasmatic levels in blood. Levels between 5.0 and 15 mg/l are considered adequate. One of the problems with teophylline is that treatment levels are very near the toxic levels. Clinically, tachycardia is an early sign of toxicity. If the newborn presents tachycardia before administering a dose of the drug (obviously excluding other possible reasons), the next dose should not be given. Next, plasmatic dosage should be carried out in order to adjust blood levels. The drug causes other undesirable effects such as upper digestive hemorrhage, increase in diuresis, hyperglycemia, and hypercalciuria. It is recommended to test periodically for blood glucose and occult blood in feces.25 In the late 1980s, studies described the efficacy of doxapram in the treatment of apnea refractory to therapeutic levels of aminophylline. The treatment required continuous infusion of the drug due to its short half-life. The therapeutic regimen did not become widely used due to its complications, such as hypertension and even intestinal hypoperfusion with increased risk for enterocolitis. Before indicating doxapram, it is necessary to better understand the pharmacokinetics of the drug in newborns, as well as the possible short- and long-term side-effects.26-28 Still in relation to treatment, it is important to comment on the use of caffeine, which is the drug of choice at other centers.29 The advantage of caffeine over teophylline is its longer half-life, which allows for timed 24-hour administration of the drug with less side-effects. In Brazil, the caffeine citrate is not available for endovenous administration. In turn, caffeine citrate for oral administration is commercially available. Different authors have recommended administration of caffeine in newborns who despite the use of teophylline still present apnea. Use of CPAP Newborn infants with recurring apnea require a more aggressive treatment despite administration of aminophylline, caffeine, or other drugs. Apneas followed by bradycardia and cyanosis frequently require bag-mask ventilation. CPAP is indicated in cases of long and/or frequent episodes of apnea. Neonatal apnea - Lopes JMA A common endotracheal tube can be used for CPAP. The tube is inserted through the nose and located at the hypopharynx. Positive pressure can be administered following Gregory’s classical circuit or with a mechanical ventilator. The administration of nasal CPAP can prevent tracheal intubation in many newborn infants with apnea. The action of CPAP is still being discussed. It is known that there is an increase in functional residual capacity, especially in newborns with less than 1,500 g. However, it is not established that this is the reason for the efficacy of CPAP. In some newborn infants, the action of CPAP is basically that of maintaining a patent airway, which is probably a case of obstructive apnea. Finally, it is still necessary to consider the action described as afferent stimulation. Positive pressure in the hypopharynx and distention of the airways (trachea and bronchi) can lead to stimulation of peripheral receptors. In turn, these receptors would support the activity of respiratory centers, thus allowing for regular breathing. Mechanical ventilation Mechanical ventilation is indicated in the treatment for apnea refractory to clinical and pharmacological treatment or to CPAP. There are two major groups of patients who usually require mechanical ventilation: – newborns of all birth weights and gestational age with severe infection; – newborns with very low birth weight (less than 1,000 g). In septic newborns, the metabolic requirements are increased and situations of coma are not infrequent. In these cases it is indicated that early mechanical ventilation be administered with the objective of reducing respiratory work and improving prognosis. In newborns with this clinical status, especially in septic newborns, pharmacological treatment is indicated. In cases of good response to antibiotictherapy, ventilatory assistance is usually carried out for shorter periods of time. Mechanical ventilation is indicated for newborns with less than 1,000 g when, as a result of apnea, the baby is labile, incapable of maintaining adequate oral intake, and incapable of maintaining good lung volume (functional residual capacity). When carrying out ventilatory assistance with very low birth weight newborns, it is important to monitor minimal ventilator settings. Usually, there are no pulmonary diseases and mechanical ventilation is indicated due to insufficient drive or muscle fatigue. FiO2 (concentration of oxygen in inspired air) should be monitored with frequency. Oxygen should be used in amounts as low as possible to maintain arterial PO2 between 50 and 60 mmHg in order to minimize risks for bronchopulmonary dysplasia and retrolental Neonatal apnea - Lopes JMA fibroplasia. Ventilator frequency settings should be as low as possible in order not to inhibit spontaneous breathing of the newborn and, thus, prevent atrophy of respiratory muscles. References 1. Kattwinkel J. Neonatal apnea: Pathogenesis and therapy. J Pediatrics 1977;90:342-7. 2. Vohr RB. Survival of the extremely preterm infant in North America in the 1990s. Clin Perinatol 2000;27:255-62. 3. Martha M, Martin RJ. Apnea of prematurity. Clin Perinatol 1992;19:789-808. 4. Harthorn MK. The rate and depth of breathing in newborn infants during different sleep states. J Physiol 1974;243:101-13. 5. Gabriel M, Albani MD, Schulte FJ. Apneic spells and sleep states in preterm infants. Pediatrics 1976;57:142-7. 6. Rigatto H, Brady JP. Periodic breathing and apnea in preterm infants. II. Hypoxia as a primary event. Pediatrics 1972;50:219-28. 7. Lopes JMA, Aranda JV, Davies GM, Mullahoo K. The role of adenosine in the hypoxic response of the newborn piglet. Pediatric Pulmonol 1994;17:50-5. 8. Rigatto H, Brady JP, De La Torre Verduzco R. Chemoreceptor reflexes in the preterm infant II. The effect of gestational and post neonatal age on the ventilatory response to carbon dioxide. Pediatrics 1975;55:614-20. 9. Langercrantz H. Improved understanding of respiratory control implications for the treatment of apnea. Eur J Pediatr 1995;154(suppl):s10-2. 10. Schulte FJ. Apnea. Clin Perinatol 1977;4:65-79. 11. Curzi-Dascalova L. Development of sleep and autonomic nervous system control in premature and full-term newborn infants. Arch Pediatr 1995;2:255-62. 12. Lopes JMA, Bryan AC, et al. Synergistic behaviour of inspiratory muscles after diaphragmatic fatigue in the newborn. J App Physiol 1981;51:447-551. 13. Lopes JMA. Respiratory muscle function during sleep [thesis]. Toronto: University of Toronto; 1982. 14. Martin RJ, Okken A, Rubin D. Arterial oxygen tension during active and quiet sleep in the normal neonate. J Pediatrics 1979;94:271-4. 15. Phillipson EA. Control of breathing during sleep. Am Rev Resp Dis 1978;118:909-39. 16. Jeffries B, Brouilette RT, Hunt C. Electromyographic study of some accessory muscles of respiration in children with obstructive sleep apnea. Am Rev Respir Dis 1984;129:696-702. 17. Carlo WA, Di Fiori JM, Martin RJ, et al. Differences in CO2 threshold of respiratory muscles in preterm infants. J App Physiol 1988;65:2434-9. Jornal de Pediatria - Vol. 77, Supl.1 , 2001 S103 18. Lopes JMA, Carvalho M, Moreira MEL, et al. Análise dos fatores de risco para apnéia neonatal no recém-nascido com peso inferior a 1.500g. Trabalho apresentado no Congresso Brasileiro de Perinatologia. Belo Horizonte;1996. 19. Keens TGA, Bryan AC, Bryan MH. Developmental pattern of muscle fiber types in human ventilatory muscles. J App Physiol 1978;44:909-13. 20. Aubier M, Marciano D, Lecognic Y, Viires N, Jaquens Y, Squara P, et al. Effect of hypophosphatemia on diaphragmatic contractility in adults with acute respiratory failure. N Engl J Med 1985;313:420-4. 21. Kinball AL, Carlton DP. Gastroesophageal reflux medications in the treatment of apnea in premature infants. J Pediatric 2001;138:355-60. 22. Wenzl TG, Schenke S, Peschgens T, Silny J, Heimann G, Skopnik H. Association of apnea and non-acid gastroesophageal reflux in infants: Investigations with intraluminal impedance technique. Pediatric Pulmonol 2001;31:144-9. 23. Henderson-Smart DJ, Steer P. Kinesthetic stimulation for preventing apnea of preterm infants (Cochrane review) Cochrane Database Syst Review 2000:000373. 24. Konner AF, Guillerminault G, Van den Hoed J, Baldwin RB. Reduction of sleep apnea and bradycardia in preterm infants on oscillating waterbeds: a controlled polygraphic study. Pediatrics 1978;61:528-33. 25. Zanardo V, Dani C, Trevisanuto D, Menegethi S, et al. Methylxanthines increase renal calcium excretion in preterm infants. Biol Neonate 1995;68:169-74. 26. Barrington KJ, Finer NN, Torok-Both GR, et al. Dose response relationship of doxapran in the therapy for refractory idiopathic apnea of prematurity. Pediatrics 1987;80:22-7. 27. Colonna F, Pahor T, de Vonderweid U, Radillo L, Tamaro G. Metabolic, hormonal and nutritional effects of long term theophylline therapy in preterm infants: a case control study. Pediatr Med Chir 1995;17:345-8. 28. Henderson-Smart DJ, Steer P. Doxapram vs methylxanthine for apnea in preterm infants (Cochrane Review). Cochrane Database Syst Rev 2000(4):000075. 29. Henderson-Smart DJ, Steer PA. Prophylactic methylxanthine for preventing apnea of preterm infants. Cochrane Database Syst Rev 2000(2):000432. Review - 000273. Correspondence: Dr. José Maria de Andrade Lopes Fundação Oswaldo Cruz Av. Rui Barbosa, 716 - Flamengo CEP 22250-020 – Rio de Janeiro, RJ, Brazil Phone: + 55 21 558.1434 – Fax: + 55 21 558.1780 E mail: [email protected]