Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
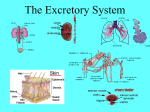
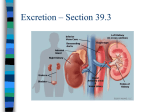
THE RENAL SYSTEM The two kidneys lie on either side of the vertebral column below the diaphragm. A coronal section of the kidney shows two distinct regions, the outer cortex and the deeper medulla which is striped in appearance due to the presence of tubules. The medulla is composed of 8-15 conical renal pyramids. Each pyramid projects into a minor calyx. Several minor calyces unit to form a major calyx. The major calyces then join to form the funnel shaped renal pelvis that collects urine from the calyces and transports it to the ureters and urinary bladder. Functions of the kidneys 1- Regulation of the extracellular fluid volume through the formation of urine. 2- Regulation of plasma volume, thus contribute to regulation of blood pressure. 3- Regulation of the concentration of waste products in blood. 4- Regulation of the concentration of electrolytes in plasma. 5- Regulation of pH of plasma. Renal blood vessels The kidneys have a rich blood supply. 25% of the total blood supply of the body passes through the kidneys each minute. Arterial blood enters the kidney through the renal artery, which divides into interlobar arteries that pass between the pyramids. Arcuate arteries branch from the interlobar arteries at the boundary of the cortex and medulla. A number of interlobular arteries radiate from arcuate arteries into the cortex and subdivide into many afferent arterioles, which deliver blood into glomeruli- capillary network that produce blood filtrate that enters the renal tubules. The blood leaves the glomerulus thro ugh an efferent arteriole which delivers blood into another capillary network, the peritubular capillaries surrounding the renal tubules. Venous blood draining from the kidney flows through the veins that trace the pathway of the arteries but in a reverse direction. 1 Microscopic structure of the kidney Each kidney contains over a million tiny structures called nephrons which are the structural and functional units and are responsible for urine formation. Structure of the nephron Each nephron consists of A- Glomerulus (network of capillaries) B- Renal tubules which consist of: Bowman’s capsule, proximal convoluted tubules (DCT), loop of Henle and distal convoluted tubules (DCT) that enter collecting ducts. The collecting ducts run downward through the medullary pyramids, giving them their striped appearance. They deliver the final urine product into the calyces and renal pelvis and out of the kidney in the ureters. Types of nephrons:1- Cortical nephrons (most nephrons) that originate in the outer 2/3 o f the cortex. 2- Juxtamedullary nephrons (few nephrons) are next to the medulla and their loops of Henle are long and dip deep into the medulla. They originate in the outer 1/3 of the cortex a play an important role in the ability of the kidney to produce a concentrated urine. Each nephron is associated with two capillary beds, the glomerulus and the peritubular capillary bed. A- The glomerulus It is fed by the afferent arteriole and drained by the efferent arteriole which are high resistance vessels, and the afferent arteriole has a larger diameter than the efferent, so blood pressure in the glomerulus is extraordinary high. This forces fluid and solutes smaller than proteins out of the blood into the glomerular capsule. 99% of this filtrate is reabsorbed by the renal tubules and returned to blood. B- The peritubular capillaries They arise from the efferent arterioles. These capillaries are low pressure vessels that are adapted for absorption instead of filtration. Urine formation Urine formation is the result of three processes:- filtration, reabsorption and secretion. 1- Filtration It is a nonselective passive process. Water and solutes smaller than proteins are forced through the capillary walls and pores of the glomerular capsule into the renal tubules. 2 Blood cells are normally too large to pass through the filtration membrane. The large size and negative charges of plasma proteins restrict their passage through the capillary membrane. The fluid that enters the glomerular capsule is called ultrafiltrate because it is formed under pressure-the hydrostatic pressure of the blood. If arterial blood pressure drops too low, the glomerular pressure becomes inadequate to force substances out of the blood into the tubules and filtrate formation stops. The force favoring filtration is opposed by:a. The hydrostatic pressure of fluid in glomerular capsule. b. The greater colloid osmotic pressure of plasma proteins as protein concentration of plasma is higher than that of tubular fluid. When these 2 forces subtracted from the hydrostatic pressure of glomerular capillaries, a net filtration pressure of about 10 mmHg is obtained. The glomerular filtration rate (GFR) It is the volume of filtrate produced by both kidneys per minute.GFR averages 115ml/min. in women and 125 ml/min in men. This is equivalent to 180 L/day. Most of the filtered water must be returned to blood or a person die within minutes. Regulation of GFR GFR is affected by changes in the diameter of afferent arterioles which result from:A- Extrinsic regulatory mechanisms (sympathetic nerve innervation) B- Intrinsic regulatory mechanism (renal autoregulation). Sympathetic nerve innervation An increase in sympathetic nerve activity, as occurs during exercise and shock, Stimulates constriction of afferent arteriole. The decrease GFR and urine formation help to preserve blood volume. Renal autoregulation It is the ability of the kidneys to maintain relatively constant GFR despite changes in mean ABP from 70 to 180 mmHg. When ABP falls toward a mean of 70 mmHg, the afferent arterioles dilate, and when the pressure rises, the afferent arterioles constrict. Blood flow to the glomeruli and GFR remain relatively constant. Also an increased flow of filtrate is sensed by special cells called macula densa, it signals the afferent arteriole to constrict thereby lowers GFR. This is called tubuloglomerular feedback. 3 2- Reabsorption About 99 % of the filtrate must be returned to the vascular system to maintain blood volume and pressure, while 1 % is excreted in urine. Tubular reabsorption begins as soon as the filtrate enters PCT. The tubular cells are transporters taking up needed substances from the filtrate (as water, glucose, amino acids and ions), and then passing them out into the peritubular capillary blood. Waste products (as urea, uric acid and creatinine) are poorly reabsorbed. Absorption of salt and water About 65 % of salt and water in glomerular filtrate is reabsorbed across the PCT and returned to the vascular system. An additional amount of salt and water (20 %) is returned to the vascular system by reabsorption through the descending limb of loop of Henle. Only 15 % of the filtrate remains to enter DCT and collecting ducts and they are absorbed by the action of hormones according to the body's state of hydration. The filtrate that enters the PCT is isotonic with plasma i.e. the total solute concentration is the same as that of plasma. The epithelial cells of the tubules have a much lower Na+ concentration. Na+-K+ pumps at the basal and lateral sides of plasma membrane of the cells in PCT transport Na+ out of the cell. As a result, a concentration gradient is created that favors diffusion of Na + from tubular fluid into the cells of PCT. Na+ is then extruded into the surrounding tissue fluid by Na +- K+ pumps. Cl- ions passively follow Na+ out of the filtrate into interstitial fluid. As a result of accumulation of NaCl, the osmotic pressure of interstitial fluid is increased above the filtered fluid and water moves by osmosis from tubular fluid into the ce lls and then into interstitial fluid and peritubular capillaries. 3- Secretion Tubular secretion is reabsorption in the reverse. Some substances such as hydrogen, potassium ions and creatinine move from the blood through the tubule cells into the filtrate to be eliminated in the urine. Characteristics of urine Freshly voided normal urine is:1- Clear and its color is pale to yellow (due to urochrome). 4 2- Sterile and its odor is slightly aromatic (but if it is allowed to stand, it takes on an ammonia odor. 3- Urine pH is slightly acidic (around 6), but certain food may cause it to be much more acidic (ac proteins diet) or basic (as vegetarian diet). 4- Its specific gravity is 1.001-1.030 (heavier than water). *Conditions that produce urine with low specific gravity are drinking excessive fluids, using diuretics, chronic renal failure. *Conditions that produce urine with high specific gravity are inadequate fluid intake, fever, a kidney inflammation (pyelonephritis). 5- Solutes normally found in urine include Na+, K+, urea, uric acid, creatinine, ammonia, bicarbonate ions. Substances not normally found in urine are glucose, blood proteins as albumin, blood cells, hemoglobin, white blood cells (pus), and bile. Concentrating mechanism of the kidney (the counter current mechanism). The kidneys excrete concentrated urine in insufficient water intake, so that excess solutes are eliminated with a little loss of water from the body. The kidneys have a special mechanism for concentration the urine called the counter current mechanism. The first step in concentration of urine is to create the hyperosmolarity of the medullary interstitial fluid. Four different solute concentrating mechanisms are responsible for this hyperosmolarity: 1- The principle cause is active transport of Na+ and secondary active transport of Cland K + out of the thick portion of ascending loop of Henle into medullary interstitial fluid. 2- Passive reabsorption of Na+ and Cl- from the thin ascending limb of loop of Henle. 3- Antidiuretic hormone helps reabsorption of urea from the inner medullary part of collecting ducts. This part becomes highly permeable to water, so urea diffuses by concentration gradient through the collecting ducts into the medullary interstitium. 4- Active Na+ and passive Cl- reabsoption from the collecting ducts into the medullary interstitial fluid. The net result of these 4 steps is an increase the osmolarity of medullary interstitial fluid (multiplier mechanism means that it multiplies or increase the osmolality of 5 medullary interstitial fluid). This cause water reabsorption from DCT and collecting ducts into the highly concentrated medullary interstitial fluid. Counter current exchange mechanism The blood vessels that run parallel to loop of Henle are called vasa recta. As blood flows down the descending limb in vasa recta, its osmolality is lower than the osmolality of medullary interstitial fluid, so NaCl and urea diffuse from the interstitial fluid into blood while water diffuses out into the interstitium. Then as the blood flow back up in the ascending limb, the osmolality of blood is higher than the osmolality of the medullary interstitial fluid, so NaCl and urea diffuse from blood into the interstitium and water diffuses back into blood. Thus the blood of vasa recta removes a little of solutes from interstitial fluid. Maintaining acid-base balance of blood Blood pH must be maintained between 7.35-7.45. Acidosis: a drop in arterial pH below 7.35 (Physiological acidosis is any arterial pH between 7.35-7.00). Alkalosis: a rise in arterial pH above 7.45. Sources of acids: 1- From ingested food. 2- As by-products of cellular metabolism. 3- Acids are produced by the body (e.g. phosphoric acid, lactic acid, fatty acids). 4- Carbonic acid is formed from CO 2 released during energy production. Sources of basic substances Ammonia and other basic substances are released to blood due to cell metabolism. Acid base balance is maintained by chemical buffers in blood, the respiratory system and the kidney (the kidney assumes most of the load for maintaining acid-base balance). Blood buffers * Chemical buffers are systems of one or two molecules that act to prevent dramatic changes in (H+) concentration when a strong acid or strong base is added. * They bind to H+ when pH drops, and by releasing H+ when the pH rises. * They are the first line of defense in resisting the pH changes as they act within a fraction of a second. 6 The bicarbonate buffer system:- is a mixture of carbonic acid (H2CO3) and its salts, sodium bicarbonate (NaHCO 3 ). * When a strong acid such as HCl is added, HCO 3 - of the salt act as bases to tie up H+ released by the stronger acid, forming more H2CO 3 which is a weak acid and lower pH only very slightly. HCl + NaHCO 3 → H2CO 3 + NaCl * When a strong base like NaOH is added to a solution containing bicarbonate buffer system, carbonic acid will be forced to dissociate further by the presence of strong base, liberating more H+ to bind with OH- released by NaOH. The net result is replacement of a strong base by a weak one, so that pH rises very little. NaOH + H2CO 3 → NaHCO3 + H2 O Respiratory system controls The respiratory system corrections of blood pH occur via regulation of CO 2 content of blood. When CO 2 enters blood from tissue cells, it is converted to H2 CO3 - for transport in plasma. CO 2 + H2O ↔ H2CO3 ↔ H+ + HCO 3 An increase in CO2 pushes the reaction to the right producing more H2CO 3 . An increase in H+ pushes the reaction to the left producing more H2CO 3 . In healthy people, CO 2 is expelled from the lungs at the same rate as it is formed in the tissues. *When CO 2 accumulates in the blood (e.g. during restricted breathing), or more H+ is released to blood from metabolic processes, the chemoreceptors in respiratory centers of brain or peripheral blood vessels are activated. As a result, breathing rate and depth increase and the excess H+ is blow off as more CO 2 is moved from the blood. *When blood pH begins to rise (alkalosis), the respiratory center is depressed. So, the respiratory rate and depth fall, allowing CO 2 (hence H+ ) to accumulate in the blood. Thus blood pH is restored to normal range. These respiratory system corrections of blood pH are accomplished within a minute or so. The renal mechanism Although the kidneys act slowly and require hours or days to bring about changes in blood pH, they are the most potent of the mechanisms for regulating blood pH. Chemical buffers can tie up excess acids or bases temporarily. The lung can dispose only H2CO 3 by eliminating CO 2 . 7 The kidneys can rid the body of other acids generated during metabolism, and have the power to regulate blood levels of alkaline substances. The kidneys maintain acid-base balance of blood by: 1- Excreting H2CO 3 2- Conserving (reabsorption) or generating new HCO 3 * As blood pH rises (alkalosis), H2CO 3 - is excreted and H+ is retained by the tubule cells. * When blood pH falls (acidosis), H2CO 3 - is reabsorbed and H+ is secreted. So the kidneys have the ability to excrete basic or acidic ions to maintain blood homeostasis (urine pH varies from 4.5-8). 8