Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
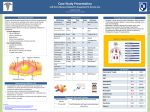
Neuro4Nurses www.neuro4nurses.com Brain Abscess Definition A brain abscess is defined as an intraparenchymal infection caused by bacteria, mycobacteria, fungi, protozoa, or helminthes that evolve to an encapsulated purulent 1,2 collection . can also view the sinuses, middle ears, and orbits to search 2 for a potential source of infection . Epidemiology A brain abscess is a rare disease. The incidence of brain abscess was 1.3/100,000 per year. The male to 3 female ratio was approximate 3:1 . Pathophysiology Brain abscesses are serious, life-threatening conditions. Despite advances in diagnostic imaging, surgical interventions, and antimicrobial treatment, the mortality (5.9% to 20%) and morbidity rate of brain abscess remain high. Approximately 35% children with brain abscesses do 1,4 not return to their predisease state after treatment . Brain abscesses are mostly related to the invasion of infectious organisms that were transmitted from an infection 5 focus in other part of the body . Spreading of infection from a remote site can occur through contiguity (close proximity) 6 or via the blood stream . The most common predisposing conditions for brain abscess are infections from contiguous foci such as otitis media or mastoiditis, sinusitis, meningitis, and odontogenic foci. Thirty three percent of brain abscess are resulted from hematogenous spread. Common sources for hematogenous spread are pulmonary infection, gastrointestinal tract, congenital heart diseases, and endocarditis. Fourteen percent are resulted from 1,7 penetrating head injuries . Eighteen percent of the 8 abscesses are due to unknown origin . Brain abscesses begin with a local infection that evolves into a collection of pus surrounded by a well vascularized 9 capsule . Approximately 80% of brain abscesses are 10 located in the cerebral hemisphere . Approximately 50% - 76% of the causative organisms of 3,7 brain abscesses are streptococci . Other causative organisms include anaerobic bacteria, staphylococci, gram11,12 negative bacteria, and fungus . Diagnostic Tests Computerized tomography (CT) scan, magnetic resonance imaging (MRI), completed blood count, blood culture, echocardiogram, and teeth examination are the most common tests for diagnosing brain abscess and to 2 detect the source of infection . In laboratory tests, signs of infection such as leukocytosis, elevated C-reactive protein concentration, and elevated erythrocyte sedimentation rate may be 8 revealed . Blood cultures are useful to detect the source of 1 microorganism from hematogenous spread . Computerized tomography is non-invasive and has a sensitivity of 95% - 99%. It is used to identify the location and size of the abscess and any mass effect. A CT scan A CT scan showing the brain abscess (arrow) Magnetic resonance imaging is able to demonstrate more anatomical detail and has better resolution than CT 13 scan . Magnetic resonance imaging is useful to detect 14 early cerebritis and alterations of the blood brain barrier . It is also able to differentiate brain abscess from brain tumor 15 or infarcts . A T-2 MRI showed a brain abscess (arrow) with cerebral edema Lumbar punctures are frequently performed when patients are suspected to have concomitant meningitis and/or ventriculitis. Cultures of the CSF obtained from lumbar puncture may grow the microorganism responsible 14 for the brain abscess . Lumbar punctures should not be performed when patients have increased intracranial 16 pressure in order to prevent cerebral herniation . Manifestations The classic triad presentation for brain abscess are 1,2,3 headache, fever, and neurological deficits . However, 12 only 20% of patients present with the classic triad . Approximately 30% of patients with brain abscess are 17 apyrexia . Manifestations of brain abscess can vary based on the location and size of the abscess. The most common presentations include headache, fever, nausea and vomiting, seizures, motor or sensory dysfunction, visual 2,4,7,12 field deficits, memory loss, and personality changes . Treatment Options The treatment choice for brain abscess depends on different factors. It includes the signs and symptoms of the patient, the number, size, and location of the abscess, and 18 health condition of the patient . Treatment options include 12,16 medical treatment, and surgical intervention . Medical treatment involves administration of antibiotic, antiepileptic agent, and corticosteroid therapy. Medical treatments are appropriate for patients who have small lesions (< 2-3 cm in diameter), are clinically stable, have no signs of increased intracranial pressure, have been diagnosed within 2 weeks after the initial presentation, abscesses in an inaccessible location, or patients who are 2,18 critically ill . Broad spectrum antibiotics are used in medical treatment or combined with surgical interventions. The most commonly used antibiotics include penicillin, ceftriaxone/cefotaxime, metronidazole, or carbapenem. Antibiotic therapies are normally continued for 4 to 8 weeks 2,7,12 . Surgical interventions are invasive, but it has several advantages. It is able to remove the pathogens and necrotic tissues, and reduce the mass effect and intracranial pressure. In addition, pus sample can be obtained and send for bacteriological analysis during the 18 surgical procedure . The advantages of aspiration are, it is minimal invasive, can be performed under local anesthetic, and has less potential morbidity. Sterotactic aspiration provides a more 19 precise and rapid access to the abscess . It is more useful in deep-seated abscess or abscess located in eloquent 20 areas . Very often, aspiration may require repeated 9 aspirations to clear the abscess . Craniotomy and excision of abscess is more invasive. Craniotomy and excision of abscess is recommended for patients with multiple abscess, larger lesions with significant mass effect, or recurrent pus collection after 19 several aspiration . Patients after craniotomies and excision of abscesses often do not require second 9 surgeries . Corticosteroids are often prescribed for reducing cerebral edema. Fifteen percent to twenty eight percent of patients with brain abscesses present with seizures. It is the also the most common post-operative complication. Anti-epileptic agents are frequently used as seizure 2,4 prophylaxis . Nursing Implication Frequent neurological assessment such as level of consciousness, motor and sensory function, and cranial nerve function should be performed to monitor for any signs of complications such as increased intracranial pressure or 14 cerebral herniation . Due to patients with brain abscess requiring long term intravenous antibiotic therapy, long term central venous catheters are recommended to avoid risks of infections 21 such as phlebitis . References 1) Bouwer, M.C., Coutinho, J.M., & van de Beek, D. (2014). Clinical characteristics and outcome of brain abscess: Systematic review and met-analysis. American Academy of Neurology, 82, 806-813. 2) Johnson, T.J., & King, C. (2013). An 11-year-old girl with right-sided weakness secondary to cerebral abscess: A case report. Pediatric Emergency Care, 29, 360-363. 3) Nicolosi, A., Hauser, W.A., Musicco, M., & Kurland, L.T. (1991). Incidence and prognosis of brain abscess in a defined population: Olmsted county, Minnesota, 1935-1981. Neuroepidemiology, 10, 122131. 4) Zhang, C., Hu, L., Wu, X., Hu, G., Ding, X., & Lu, Y. (2014). A retrospective study on the aetiology, management, and outcome of brain abscess in an 11-year, single-center study from China. BMC Infectious Diseases, 14, 311, 1-7. 5) Ç avuşoglu, H., Kaya, R.A., Türkmenoglu, O.N., Ç olak, I., & Aydin, Y. (2008). Brain abscess: Analysis of results in a series of 51 patients with a combined surgical and medical approach during an 11-year period. Neurological Focus, 24, E9, 1-7. 6) Antunes, A.A., de Santana Santos, T., de Carvalho, R.W.F., Avelar, R.L., Pereira, C.U., & Pereira, J.C. (2011). Brain abscess of odontogenic origin. The Journal of Craniofacial Surgery, 22, 23632365. 7) Felsenstein, S., Williams, B., Shingadia, D., Coxon, L., Riordan, A., Demetriades, A.K., ... Bryant, P.A. (2013). Clinical and microbiologic features guiding treatment recommendations for brain abscesses in children. The Pediatric Infectious Disease Journal, 32, 129-135. 8) Oyama, H., Kito, A., Maki, H., Hattori, K., Noda, T., & Wada, K. (2012). Inflammatory index and treatment of brain abscess. Nagoya Journal of Medical Science, 74, 313-324. 9) Sarmast, A.H., Showkat, H.I., Kirmani, A.R., Bhat, A.R., Patloo, A.M., Ahmad, S.R., & Khan, O.M. (2012). Aspiration versus excision: A single center experience of forty-seven patients with brain abscess over 10 years. Neurologia medico-chirurgica, 52, 724-730. 10) Goodkin, H.P., Harper, M.B., & Pomeroy, S.L. (2004). Intracerebral abscess in children: Historical trends at Children’s Hospital Boston. Pediatric, 113, 1765-1770. 11) Choudhury, N., Khan, A.B., Tzvetanov, I., Garcia-Roca, R., Oberholzer, J., & Benedetti, E. (2014). Multiple aspergillus brain abscess after liver transplantation. Transplantation, 97, e72-e73. 12) Helweg-Larsen, J., Astradsson, A., Richall, H., Erdal, J., Laursen, A., & Brennum, J. (2012). Pyogenic brain abscess, a 15 year survey. BMC Infectious Diseases, 12, 1-10. 13) Frazier, J.L., Ahn, E.S., & Jallo, G.I. (2008). Management of brain abscesses in children. Neurological Focus, 24, E8, 1-10. 14) Twomey, C.R. (1992). Brain abscess: An update. Journal of Neuroscience Nursing, 24, 34-39. 15) Chen, M.H., Kao, H.W., & Cheng, C.A. (2013). Complete resolution of a solitary pontine abscess in a patient with dental caries. American Journal of Emergency Medicine, 31, 892.e3-892.e4. 16) Erdoğan, E., & Cansever, T. (2008). Pyogenic brain abscess. Neurosurgical Focus, 24, E2, 1-10. 17) Couloigner, V., Sterkers, O., Redondo, A., & Rey, A. (1998). Brain abscess of ear, nose, and throat origin: Comparison between otogenic and sinogenic etiology. Skull Base Surgery, 4, 163-168. 18) Hakan, T. (2008). Management of bactyerial brain abscess. Neurosurgical Focus, 24, E4, 1-7. 19) Moorthy, R.K., & Rajshekhar, V. (2008). Management of brain abscess: An overview. Neurosurgical Focus, 24, E3, 1-6. 20) Kocherry, X.G., Hegde, T., Sastry, K.V.R., & Mohanty, A. (2008). Efficacy of sterotatic aspiration in deep-seated and eloquent-region intracranial pyogenic abscess. Neurosurgical Focus, 24, E13, 1-5. 21) Baumann, C.K. (1997). Multiple bilateral cerebral abscesses with hemorrhage. Journal of Neurosciences Nursing, 29, 1-11. © 2014 Disclaimer: The author of this article neither represents nor guarantees that the practices described herein, if followed, ensure safe and effective patient care. The author further assumes no responsibility or liability in connection with any information or recommendations contained in this article. The recommendations and instructions in this article are based on the knowledge and practice in neuroscience as of the date of publication. These recommendation and instructions are subject to change based on the availability of new scientific information.