Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
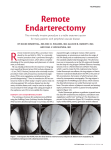
GE Healthcare CT Clinical Case Study Trauma CT Occlusion Superficial Femoral Artery (SFA) Jorge Soto, M.D. Stephan Anderson, M.D. Boston University Medical Center Boston, MA imagination at work CT Clinical Case Study Trauma CT Occlusion Superficial Femoral Artery (SFA) Jorge Soto, M.D. Stephan Anderson, M.D. Boston University Medical Center Boston, MA Figure 1 Oblique Angio View demonstrating thrombosis within the Left Femoral Artery. Patient History A 14-year-old male presented to the emergency department with injuries sustained to the left lower extremity and pulsatile bleeding that he obtained from a rollover All-Terrain Vehicle (ATV) collision. A Computed Tomography Angiography (CTA) of the left lower extremity was requested by the referring emergency physcian for further evalution of the patient’s injuries. Acquisition Protocol Scanner: Scan Type: Rotation Speed: Detector Configuration: Slice Thickness: Pitch: SFOV: DFOV: kVp: mA: Total Scan Time: Figure 2 Lateral Angio View demonstrating thrombosis within the Left Femoral Artery. LightSpeed® VCT Helical 0.5 seconds 64 x 0.625 0.0625mm 0.516:1 50.0cm 36.0cm 120 200mA 15.8 seconds Contrast Injection Parameters Using a Double-Barrel Injector: • Prep Delay = 25 seconds • 100ml of contrast at 5cc/sec. +30 ml of saline at 5cc/sec. Contrast Type: Non-Ionic 320mg I/ml Clinical Findings The CTA exam assisted the radiologist in determining the following clinical diagnostic imaging findings: 1. There is a traumatic thrombosis within the left Superficial Femoral Artery (SFA) in the region of the soft tissue abnormality secondary to the patient’s injury. The lumen of the vessel is totally absent distally from this level until reconstitution is seen from the superior geniculate arteries in the region of the popliteal fossa. 2. The popliteal artery reconstitutes and then demonstrates a normal trifurcation. 3. The distal anterior tibial artery is not clearly seen. Figure 3 Oblique Angio View demonstrating popliteal artery with normal trifurcation. Figure 4 Lateral Angio View demonstrating popliteal artery with normal trifurcation. Figure 6 Oblique Bone/Vessel Transparency View demonstrating popliteal artery with normal trifurcation. Figure 7 Axial MIP View demonstrating subcutaneous emphysema throughout the fascial planes. 4. There is subcutaeous emphysema seen throughout the fascial planes in the region of the patient’s injury. 5. There are no fractures. Discussion Based on the CTA findings the patient went directly to surgery for surgical intervention to restore blood flow to the left lower extremity. Because there was extensive damage to the Superfiical Femoral Vein (SFV) and SFA, the SFV was ligated to ensure no future bleeding and a portion of the SFA was resected, leaving a substantial gap. Therefore, a segment of the Saphenous Vein was used to graph the dissected SFA both Figure 5 Oblique Bone/Vessel Transparency View demonstrating thrombosis within the left femoral artery. proximally and distally to restore blood flow. In addition, due to the prolonged ischemic time to the patient’s left lower extremity, four compartment fasciotomys were also done at the time of surgery to help control swelling of the leg to avoid compromising blood flow in the graft. ©2006 General Electric Company – All rights reserved. GE and GE Monogram are trademarks of General Electric Company. LightSpeed is a registered trademark of GE Medical Systems. GE Medical Systems, a General Electric company, going to market as GE Healthcare. GE Healthcare 3000 North Grandview Waukesha, WI 53188 U.S.A. www.gehealthcare.com imagination at work CT-0253-02.06-EN-US