Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
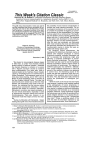
Nephrol Dial Transplant (1996) 11: Editorial Comments 1952 patients with different degrees of renal insufficiency and on different renal replacement therapies to treatment with either lovastatin, simvastatin, or pravastatin [2]. Rhabdomyolysis has not been reported as a major complication, although a moderate rise in serum creatine kinase is observed occasionally [3,4]. However, experience is limited particularly in patients with severe impairment of renal function prior to initiation of dialysis. It can be argued that drug or metabolite accumulation and uraemia-related muscle injury increase the risk of myositis, especially in this subset of patients. The situation is somewhat different and the risk of drug and metabolite accumulation probably less severe in dialysis patients since lovastatin is cleared by the haemodialysis procedure itself [5]. Therefore the protocol of the US HEMO study forsees HMGCoA reductase inhibitors as drugs of first choice for treatment of persistent elevation of serum LDL cholesterol (> 160 mg/dl) in haemodialysis patients [6]. Several large-scale intervention and regression studies (4S, WOS and CARE) have given a rationale for using HMG-CoA reductase inhibitors in primary and secondary prevention of coronary heart disease. Therefore a number of patients, among them many with impaired renal function, will be candidates for treatment in the future. HMG-CoA reductase inhibitors are safe and valuable drugs in patients with renal insufficiency. However, before further experience is published, it may be prudent to limit the dose of lovastatin and pravastatin (<20mg/day) as well as simvastatin (<10mg/day) in patients with a GFR below lOml/min and prior to initiation of dialysis, as recommended by Biesenbach and collegues [1]. References 1. Biesenbacli G, Janko O, Stuby U, Zazgornik J. Myoglobinuric renal failure due to long-standing therapy in a patient with preexisting chronic renal insufficiency. Nephrol Dial Transplant 1996; 11: 000-000 [THIS ISSUE—INSERT NOS] 2. Massy ZA, Ma JZ, Louis TA, Kasiske BL. Lipid lowering therapy in patients with renal disease. Kidney Int 1995; 48: 188-198 3. Wanner C, H6rl WH, Luley CH, Wieland H. Effects of HMGCoA reductase inhibitors in hypercholesterolemic patients on hemodialysis. Kidney Int 1991; 39: 754-760 4. Wanner C, Bohler J, Eckardt HG, Wieland H, Schollmeyer P. Effects of simvastatin on lipoprotein (a) and lipoprotein composition in patients with nephrotic syndrome. Clin Nephrol 1994; 41: 138-143 5. Eckardt H, Karkas JD, Germershausen JI, Liou R, Wanner C. Lovastatin is hemofiltrable. In: Gotto AM, Mancini M, Richter WO, Schwandt P (eds). Treatment of Severe Dyshpoproteinemia in the Prevention of Coronarv Heart Disease. Karger, Basel 1992; 292-295 6. Eknoyan G, Levey AS, Beck GJ et al. for the Hemo Study Group. The hemodialysis (HEMO) study: rationale for selection of interventions. Semin Dial 1996; 9: 24-33 Editor's note Please see also the Case Report by Biesenbach et al. (pp. 2059-2060 in this issue). Are post-transplant lymphomas inevitable? G. Opelz Department of Transplantation Immunology, Institute of Immunology, University of Heidelberg, Germany An increased occurrence of non-Hodgkin lymphomas in kidney transplant patients was first reported by Penn some 25 years ago [1]. Many authors have confirmed this finding and post-transplant lymphomas have become a well-recognized 'complication' of immunosuppressive treatment. The majority of posttransplant lymphomas are of B cell origin, they are Epstein-Barr virus (EBV) induced, and it is believed that immunosuppressive therapy interferes with the T cell control mechanisms that prevent the uninhibited proliferation of B cells in healthy individuals [2]. How frequent are post-transplant lymphomas? Reliable figures on the incidence of post-transplant lymphomas have been difficult to obtain because the Correspondence and offprint requests to: Gerhard Opelz, MD, Institute of Immunology, Im Neuenheimer Feld 305, D-69120 Heidelberg, Germany. absolute numbers of cases occurring at individual transplant centres are small. A large multicentre analysis of the Collaborative Transplant Study arrived at an incidence in cadaver kidney recipients of approximately 0.2% during the first post-transplant year [3]. The yearly incidence decreased during subsequent years and remained fairly stable at approximately 0.04% per year. Compared with the general population, the first year incidence is about 20-fold increased. Interestingly, post-transplant lymphomas occur approximately twice as often in North America than in Europe [3]. Lymphomas are seen at a much higher rate in heart transplant recipients than in kidney transplant recipients. This observation provides important clues with respect to the nature of promoting factors. Figure 1 illustrates an update of the Collaborative Transplant Study analysis on the cumulative incidence of posttransplant lymphomas in kidney and heart transplant recipients. 1953 Nephrol Dial Transplant (1996) 11: Editorial Comments FIRST HEART TX 100 o o o FIRST CADAVER KIDNEY TX o o i * 4000 4000 • CD a. CD Q. ! 8 3000- g CD T3 _C y* 2000 3 o 2000 y* * CD * 1000- •2 1000E 3 j 00 1 3000 CD / CD > co 5000 o 2 3 4 5 6 Years 7 8 9 10 0 1 2 3 4 5 6 7 8 9 Years 10 n=72360 HEART n=14284 Fig. 1. Cumulative incidence of non-Hodgldn lymphomas in recipients of heart transplants (left) or cadaver kidney transplants (right). The numbers of patients studied are indicated at the bottom of each graph. Factors that influence the occurrence of lymphomas It is widely believed that the strength of immunosuppressive treatment is directly related to the incidence of post-transplant lymphomas. The differential incidence in kidney and heart transplant recipients supports this notion. Heart recipients are known to receive more aggressive immunosuppressive treatment during the early post-transplant period than kidney recipients. Moreover, evidence was found for higher immunosuppressive maintenance doses in heart than in kidney recipients (as well as in kidney and heart recipients treated in North America compared to patients treated in Europe) [3]. Unquestionably, induction therapy with monoclonal or polyclonal antilymphocyte antibodies increases the risk of lymphoma. The risk associated with antibody induction is moderate [4], although the massive administration of antilymphocyte antibodies was associated with an excessive rate of lymphomas in one series of heart transplant patients [5]. There has been speculation that the cumulative dose of immunosuppressive drugs and antibodies administered may be a key variable. The case report published in this issue, in which a patient developed a lymphoma after receiving antibody induction as treatment for a kidney graft, having had a previous heart transplant, would seem to fit the 'cumulative dose' hypothesis [6]. There are intriguing data, however, indicating that the occurrence of lymphoma is not completely explained by the effect of potent immunosuppression. When the locations at which the lymphomas occurred were analysed, there was a striking prevalence of lymphomas of the kidney in renal transplant recipients, and of lymphomas of the lung or heart in heart transplant recipients [3], These highly significant associations indicate that the local immune response against the transplanted organ must play an important role in the cellular deregulation process that results in lymphomas. Another interesting observation is that lymphomas of the CNS occur at a relatively high frequency in organ transplant recipients, whereas they are extremely rare among lymphoma patients in the non-transplant population [4]. Prognosis of lymphomas There are a number of anecdotal reports in the literature showing that lymphomas regressed or disappeared in patients when immunosuppressive treatment was reduced or discontinued [7]. Therefore, it is nowadays common practice to decrease or, if deemed permissible, discontinue immunosuppressive treatment in patients developing a lymphoma. Unfortunately, this strategy does not uniformly result in permanent regression of the tumour. The survival statistics following the diagnosis of post-transplant lymphoma show a sobering 50% death rate within a year of diagnosis (Fig. 2). Patients with CNS lymphoma appear to do particularly poorly [4]. What can be done? With the rather grim survival prospects of patients who develop post-transplant lymphomas, prevention rather than treatment would seem to deserve the high- Nephrol Dial Transplant (1996) 11: Editorial Comments 1954 FIRST CADAVER KIDNEY TX 100-] 100- 90- 90 80- 80- 7060- its Surviving its Surviving FIRST HEART TX • 50- 40a. 3020CD CD CO "ra Q. 70- I 6050403020- 10- 10- n U n c 1 2 3 4 5 6 7 8 9 Years 10 c HEART n=354 1 2 3 4 5 6 7 8 9 Years 10 KIDNEY n=360 Fig. 2. Survival after the time of diagnosis in heart or kidney transplant recipients with non-Hodgkin lymphomas. The numbers of patients studied are indicated at the bottom. est priority. This raises the dilemma of balancing too little against too much, that is, underimmunosuppression with resulting graft rejection against overimmunosuppression and lymphoma. Clearly, some risk of lymphoma must be accepted in organ transplant recipients. In general, because the risk of lymphoma is infinitely smaller than that of graft rejection, there is an understandable inclination of preserving a functioning graft even though this may carry on increased risk of lymphoma. Nevertheless, it would seem prudent to aim at the 'smallest necessary' cumulative immunosuppressive regimen. In this context, good HLA compatibility deserves special attention since it provides an opportunity for getting by on less intensive immunosuppressive treatment. More potent and more effective immunosuppressive medication is usually associated with some increase in the risk of lymphoma. Combination drug therapy, which is commonly used because it allows for a reduction of other drug-related side effects, also is associated with an increased lymphoma risk [4]. The argument to be addressed here is that more powerful immunosuppression should not be avoided at all cost, and that sound judgement should dictate the choice of immunosuppressive induction and maintenance regimen, as well as the doses at which the drugs are administered. In a 'high risk' recipient, e.g. a patient with highly reactive lymphocytotoxic antibodies or a retransplant recipient, induction therapy with poly- or monoclonal antibodies may well be appropriate. Likewise, triple drug maintenance will be necessary for some patients but not for others. Especially when the cumulative load of previous immunosuppression, including rejection treatment, has already been high, caution must be exercised. Unfortunately, little information is currently available on 'acceptable thresholds' of cumulative immunosuppression beyond which the risk of lymphoma becomes unacceptable. It therefore remains a challenge for each physician to carefully weigh any benefits of increased immunosuppression against the potential risk of lymphoma. A final word of caution would seem appropriate with respect to the new, even more powerful immunosuppressive drugs which are currently being introduced. While there is an understandable desire for stronger and better immunosuppression, the lymphoma issue should not be overlooked. It would be wrong to take an alarmist position and to argue against the introduction of new immunosuppressants. Nevertheless, care should be taken to carefully monitor the effect of any new drug on the incidence of lymphomas, a complication which fortunately affects a very small proportion of all transplant patients but which is associated with a high risk of death. References 1. Perm I, Hammond W, Brettschneider L, Strzl TE. Malignant lymphomas in transplantation patients. Transplant Proc 1969; 1: 106-112 2. York LJ, Qualtiere LF. Cyclosporine abrogates virus-specific T cell control of EBV-induced B-cell lympho-proliferation. Viral Immunol 1990; 3: 127-136 3. Opelz G, Henderson R. Incidence of non-Hodgkin lymphoma in kidney and heart transplant recipients. Lancet 1993; 1514-1516 4. Opelz G, Schwarz V, Wujciak T et al. Analysis of non-Hodgkin's lymphomas in organ transplant recipients. Transplant Rev 1995; 231-240 5. Swinnen U A , Constanzo-Nordin MR, Fisher S el al. Increased incidence of lymphoproliferative disorder after immunosuppres- Nephrol Dial Transplant (1996) 11: Editorial Comments sion with the monoclonal antibody OKT3 in cardiac transplant recipients. N EnglJ Med 1990; 323: 1723-1728 6. Haas et at. Nephrol Dial Transplant 1996; 11: 000-000 7. Starzl TE, Nalesnik MA, Porter KA et al. Reversibility of lymphomas and lymphoproliferative lesions developing under cyclosporine-steroid therapy. Lancet 1984; 1: 583-587 1955 Editor's note Please see also the Case Report by Haas et al. (pp. 2085-2087 in this issue). Nitric oxide (NO) in renal physiology and pathophysiology C. Baylis and J. Bloch Department of Physiology, West Virginia University, Morgantown, WV, USA Renal localization of NO synthesis Endogenous NO is synthesized by nitric oxide synthases (NOS) which use L-arginine as substrate. The various isoforms of NOS are widely distributed within the kidney. Brain NOS (bNOS) and endothelial NOS (eNOS) are constitutively expressed and are both distributed in glomeruli and vasculature. In addition bNOS is found in epithelial tissue including macula densa and the collecting duct. Two structurally distinct inducible NOS (iNOS) are 'constitutively expressed' at the juxtaglomerular apparatus (JGA) and in tubules and after immune stimulation iNOS has been located in glomerular mesangial cells and several locations in the tubule [1,2] Physiological actions of NO on the kidney NO synthesized by eNOS, and possibly bNOS, has a major role in control of renal vascular tone, via its vasodilatory actions. NO produces vasodilatation via a cyclic guanosine, 3',5', monophosphate (cGMP) mechanism and also by stimulating calcium-dependent potassium channels [1]. Generalized systemic NO inhibition (NOI) leads to dose dependent increases in blood pressure (BP) and renal vascular resistance (RVR), a large fall in renal plasma flow (RPF) and a slight fall in glomerular nitration rate (GFR) [1]. The kidney is particularly sensitive to NO inhibition, which leads to increases in afferent arteriolar resistance (RA), decreases in the ultrafiltration coefficient (K f ), possibly via mesangial cell contraction [ 1 ] and a variable effect on the efferent arteriolar resistance (RE)- When systemic NO inhibition leads to increased BP, RE rises and causes marked elevation in the glomerular blood pressure (PGc)- I n addition to directly influencing vascular tone via eNOS, NO at the JGA controls glomerular hemodynamics via the tubuloglomerular feedback mechanism (TGF). JGA NO blunts the Correspondence and offprint requests to: Chris Baylis, Department of Physiology, PO Box 9229, West Virginia University, Morgantown, WV 26506-9229, USA. increase in RA seen when the macula densa is perfused with high NaCl [3]. Also, NO plays complex roles in control of JGA renin release [1-3] and the physiological relationship between NO and renin has not yet been defined. NO also influences sodium excretion and may play a physiological role in control of sodium balance. NO has a direct tubular effect to inhibit sodium reabsorption in the collecting duct . Also local administration of NOI into the renal medullary interstitium selectively decreases papillary blood flow and lowers urinary sodium excretion with no change in GFR or BP. It is likely that NO controls sodium excretion both by direct tubular actions and also by regulating the vascular tone in the medullary circulation and the pressure natriuresis. There is some evidence that increased NO production is stimulated by increased dietary salt intake in normal animals, and may function as a 'natriuretic hormone' although the origin of this NO remains to be determined [2]. NO also influences growth and is generally reported to function as an anti-growth factor, although this has recently been disputed [1,2,4]. Deranged NO production in renal pathology Overproduction of NO There is increasing evidence that elevated levels of NO play a primary pathogenic role in some forms of immune-mediated glomerular injury. The injurious NO in glomerular inflammation probably originates from iNOS and may come from a variety of cell types including infiltrating macrophages and resident glomerular cells including mesangial cells [1]. NO appears to play a primary pathogenic role in the glomerular injury caused by antithymocyte serum; an acute glomerulonephritis that primarily involves the glomerular mesangial cells. Both NOI and dietary arginine deprivation are protective, and in this model excess NO actually promotes glomerular extracellular matrix accumulation [5]. Excessive NO is cytotoxic by several mechanisms, including formation of peroxynitrite and