Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Social Bonding and Nurture Kinship wikipedia , lookup
Insufficient justification wikipedia , lookup
Developmental psychology wikipedia , lookup
Social psychology wikipedia , lookup
Symbolic behavior wikipedia , lookup
Behavioral modernity wikipedia , lookup
Prosocial behavior wikipedia , lookup
Bullying and emotional intelligence wikipedia , lookup
Verbal Behavior wikipedia , lookup
Observational methods in psychology wikipedia , lookup
Organizational behavior wikipedia , lookup
Social perception wikipedia , lookup
Neuroeconomics wikipedia , lookup
Impression formation wikipedia , lookup
Applied behavior analysis wikipedia , lookup
Operant conditioning wikipedia , lookup
Psychological behaviorism wikipedia , lookup
Residential treatment center wikipedia , lookup
Attribution (psychology) wikipedia , lookup
Abnormal psychology wikipedia , lookup
Theory of planned behavior wikipedia , lookup
Thin-slicing wikipedia , lookup
Adherence management coaching wikipedia , lookup
Transtheoretical model wikipedia , lookup
Theory of reasoned action wikipedia , lookup
Descriptive psychology wikipedia , lookup
Behavior analysis of child development wikipedia , lookup
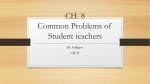
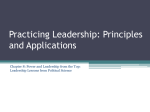
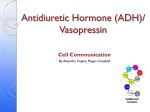
Uniqque asso ociations of callous‐uneemotionnal versuus oppossitional a and atteention‐deficit/hyyperactiive behaaviors am mong prreschool childreen: are therre multipple dom mains witthin earlly‐startiing childd behaviior problems? Key Terrms Defin ned Callous‐une emotional beh havior – Callouus unemotionaal (CU) behavio ors refer to beh haviors such as a lack of e empathy, low g guilt, and shal low affect. Oppositiona al behavior – O Oppositional b behaviors incluude behaviors s such as irritablle mood, defiance, vin ndictiveness, n negative affectt, and emotion nal dysregulation. Authors & Affiliations R Rebecca Wa aller1 Lu uke W. Hyd de1,2,3 Ad dam S. Grab bell1,4 M Martha L. Allves1 Sheryl L. Olson1,2 1 Departmen nt of Psycchology, University of Michigan, USA 2 C Center for Hu uman Growth an nd Developme ent, Univversity of Michigan, USA 3 In nstitute for S Social Reseearch, Unive ersity of Michigan, U USA 4 Departmen nt of Psyychiatry, University of P Pittsburgh M Medical Center, US SA Attention d deficit/hyperacctive behaviorr ‐ Attention deficit/hyperacttive (ADH) beh haviors refer to behaviorss, such as atten ntional problem ms, impulsivityy, lack of focuss, and an inability to concentrate e. Nomologica al network ‐ re efers to the chaaracteristics and observable behaviors thaat define the variables of interest in a sttudy, includingg their associattions with otheer variables and the outcomes th hey predict. Proactive ag ggression ‐ plaanned and goaal‐oriented agg gressive behavvior for individual gain, including maaterial possesssions or social dominance. Reactive ag ggression ‐ frusstrated and hoostile aggressivve behavior in response to peerceived provocation n or stimulation n. Backgro ound Child behavior problems (e e.g., aggressioon, rule‐breaking), beginning g as early as the toddler n important pu ublic health co ncern becausee of the harm t they cause to t he well‐ years, are an being of chilldren, families, communitiess, and schools. In particular, e early child beh havior problems pu ut children at r isk of develop ing aggression n and violence as they grow u up, which is harmful to t hemselves, other people, annd very costly t to society as a whole. Thus th here is a evention and trreatment proggrams that worrk with families and children to reduce need for pre the risk for f future aggression and violencce. However, a an issue that complicates our ability to design effecctive treatments is that child behavior prob blems are heteerogeneous in n nature, differing in t the age that th hey start (e.g., early childhoo od versus earlyy adolescence),, the outcomes th hat they are asssociated with,, and the facto ors that cause t them. Research is needed to identify d different types of behavior prroblems so we can better maatch different t treatments according to o children’s ind dividual needs.. In relation to o this question n, researchers h have proposed d three differen nt domains witthin child behavior pro oblems. The firrst domain is d defined by high h levels of oppositional behaavior and includes deffiance, anger, a and emotionall dysregulation n. A second do omain comprisees attention‐ deficit/hyperactive (ADH) behavior, com mprising poor in nhibitory control, high impulsivity, and onal control. Finally, a third d domain focusess on callous‐un nemotional (CU) behavior low attentio and includess reduced emo otional responssiveness, deficcits in empathyy, and a lack off guilt. Several rece ent studies havve investigatedd these three d domains among older childreen and adolescents (see a review by Frick et al., 2014), but litttle research has been conduccted among i.e., under 5 yeears old), which preschool‐aged samples (i h is a critical peeriod for severral reasons. e or violent havve often shown n behavior pro oblems as youn ng children. Adults who are aggressive Thus, a focu us on understan nding the emeergence and deevelopment off behavior prob blems before they become severe is imp portant for infoorming interveentions that co ould help preveent children uent violence o or crime. In ad ddition, evidence suggests th hat behavior from perpettrating subsequ National Cente er for Injury Prevvention and Coontrol Unique associations of callous‐unemotional versus oppositional and attention‐deficit/hyperactive behaviors among preschool children: are there multiple domains within early‐starting child behavior problems? problems are more malleable at younger ages (e.g., Dishion et al., 2008; Reid et al., 2004), allowing for greater possibility of improving children’s current and future outcomes through early‐starting treatment and interventions strategies. Finally, the preschool years represent an important time of change when children undergo rapid physical, neurological, and psychological development. This period of transition is often very hard for parents to manage and a time when break‐downs in the parent‐child relationship can commonly occur. The current study investigated three research questions. First, can these three domains of child behavior problems (ADH, oppositional, and CU behaviors) be measured as separate constructs at age 3? To test this question we collected parent reports on a child behavior questionnaire and used quantitative factor analytic techniques. Second, do ADH, oppositional, and CU behaviors have different nomological networks of associated behaviors? To test this question, we examined their unique associations with measures of various socio‐emotional and cognitive processes. Third, do oppositional, ADH, or CU behaviors predict higher teacher‐reported behavior problems from ages 3‐6 years old? Overall, the aims of the study were to provide a thorough examination of the potentially distinct nomological networks of ADH, oppositional, and CU behaviors; and to evaluate which of these behaviors predicted the worst outcomes at school age. Study Methods: Data are from 240 children (118 girls) and their parents, who were part of a study of young children at risk for behavior problems in Michigan. Data were collected when children were 3 years old and again when they were 6 years old. Most children were of European American background (86%), with others self‐identifying as African‐American (5%) or biracial (8%). We collected data from mothers and fathers in family homes. Parents answered questions about their children’s ADH behavior (e.g., ‘he/she can’t stand to wait’), oppositional behavior (e.g., ‘he/she is defiant’), and CU behavior (e.g., ‘he/she shows a lack of guilt after misbehavior’). Parents also completed questionnaires assessing children’s anger/frustration, fear, ability to control their attention, guilt, moral understanding, and empathy towards others. We also collected questionnaire data from teachers who reported on children’s general behavior problems, as well as their proactive aggression (e.g., ‘he/she bullies others’) and reactive aggression (e.g., ‘when teased, he/she strikes back’). Finally, children participated in a 4‐hour laboratory session at a local preschool, during which they completed six tasks to assess their effortful control (e.g., ability to delay responses, ability to regulate their emotions) which was videotaped and then coded by researchers. To examine a measurement model for ADH, ODD, and CU behavior, we used confirmatory factor analysis. To test nomological networks and which dimension predicted future behavior problems, we used linear regression. Results: The best‐fitting measurement model using items from a commonly used parent‐reported behavior checklist was one where ADH, oppositional, and CU behavior were assessed as three separate factors 1 (see Figure 1). We found that each domain was linked to a specific and distinct nomological network: oppositional behavior was strongly related to parent reports of anger and frustration; ADH behavior was related to lower observed ability to delay responses and regulate emotions as well as lower parent‐reported attentional focus; and CU behavior was related to lower parent‐ reported moral regulation, guilt, and empathic concern (see Figure 2). We found that age 3 CU behavior predicted externalizing behavior problems and proactive aggression at age 6, as judged by teachers. This prediction was over and above earlier teacher‐reports of externalizing behavior and ADH and oppositional behaviors. Overall, results showed that consistent with theory, ADH behaviors were specifically associated with difficulty regulating attention and behavior control, oppositional behavior was associated with difficulty controlling anger and frustration, and CU behavior was related to difficulties with empathy, guilt, and moral development (data not shown). Importantly, CU behaviors were the best predictor of identifying which children had most behavior problems in schools 3 years later, even after taking into account their initial levels of behavior problems. 1 Statistically, this model fit significantly better than a model where ADH, oppositional, or CU behavior all loaded onto one ‘problem behavior’ factor sdfsfdsfdadsf Uniique associa ations of calllous‐unemo otional versuus oppositioonal and atteention‐deficcit/hyperactive behaviors amoong prescho ool children:: are there m multiple dom mains withinn early‐startting child beehavior probblems? Figure e 1. Measurementt of oppositional, attentio on‐deficitt/hyperacctive, and ca allous une emotional behaviors at ag ge 3 baseed on con nfirmatory factor analysis [Items aree based onn mother a and fatherr reports on a child b behavior questio onnaire; Co olored arro ows (—,— —,and —) i indicate th he questionnaire item ms that are inclluded in ea ach of the three sepa arate beha avior dimeensions. Bllack doublle‐ headed d arrows (↔ ↔) indicatte overlap between d dimensionss]. Figure e 2. Differrential asssociations of opp positionaal, attenttion‐ deficitt/hyperacctive, and d callouss unemottional beh haviors w with relevvant socioe emotiona al and cog gnitive co orrelatess suggestting distiinct nomollogical ne etworks of these behaviorral dimen nsions sdfsfdsfdadsf s Uniique associa ations of callous‐unemo otional versuus oppositioonal and atteention‐deficcit/hyperacttive behavio ors among prescho ool children: are there m multiple dom mains withinn early‐startting child beehavior probblems? Figure 3. Predicction of te eacher re eports off behavio or problems at age 6 by teacher reportss of behavvior prob blems at age 3 and parentt reports of opposittional, atttention‐‐deficit/h hyperactiive, and callous u unemotio onal behaviors at ag ge 3. Figure 3 Notte. All models a also controlled d for child gend der, child age ( (in months), faamily income, a and child verbal IQ. Teacher‐ reports of extern nalizing behavvior problems a at age 3 predictted teacher‐reeportes of exteernalizing behaavior problems, p proactive aggre ession, and reaactive aggression at age 6 (ppurple arrows → →). Parent rep ports of CU beh havior at age 3 also predicted teacher re eports of exterrnalizing behavior and proacctive aggressio on at age 6 (blu ue arrows →). Neither al nor ADH beh haviors at age 3 3 predicted teaacher‐reportedd outcomes att age 6 (no arro ows shown). oppositiona Implica ations forr Violencce Preven ntion The findings of this study have importan nt violence pre evention impliccations that arre relevant to p parents, teachers, and We showed tha at oppositionall, ADH, and CU U behaviors ca n be separately assessed am mong young children and clinicians. W that they ha ave separate nomological ne etworks: oppossitional (i.e., annger/frustratio on), ADH (i.e., low attentionaal and effortful con ntrol), and CU (i.e., deficits in n conscience, i including low g guilt and a lackk of empathic c concern) behaviors. We also found t that CU behavior (but not op ppositional or A ADH behavior)) uniquely pred dicted increasees in child behaavior problems att school. These findin ngs highlight t he need for strategies to ide entify the diffe rent types of e early behavior problems amo ong children in order to f facilitate accesss to appropriaate treatment. More broadly,, although we know that inteerventions that target parenting p practices and skkills are the mo ost effective fo or reducing chiildren’s behaviior problems, t the findings fro om this study suggest tha at we might have an even gre eater effect forr reducing childdren’s behavio or by personaliizing treatmen nts according to children’s preschool levvels of oppositional, ADH, an nd CU behavio rs. For examplle, because children with CU U behaviors athy for others, treatments could focus on increasing emotional saliencce of situationss to help seem to havve lower empa children mo odify their aggression. Treatm ment strategie es that have shhown promise in this area foccus on promotting warmth, affect and e eye contact bettween parentss and children ( (see Dadds et al., 2014; Hydee, Waller, & Bu urt, 2014). Other r resourcess for info ormation on this t topic This brief is a summary off research that has been published in the Joournal of Child Psychology an nd Psychiatry. T The paper is om/doi/10.1111/jcpp.12326/ppdf available at: http://onlinellibrary.wiley.co Unique associations of callous‐unemotional versus oppositional and attention‐deficit/hyperactive behaviors among preschool children: are there multiple domains within early‐starting child behavior problems? References Dadds, M.R., Allen, J.L., McGregor, K., Woolgar, M., Viding, E. & Scott, S. (2014). Callous‐unemotional traits in children and mechanisms of impaired eye contact during expressions of love: a treatment target? Journal of Child Psychology and Psychiatry, 55, 771–780. Dishion, T.J., Shaw, D., Connell, A., Gardner, F., Weaver, C., & Wilson, M. (2008). The Family Check‐Up with high‐risk indigent families: Preventing problem behavior by increasing parents' positive behavior support in early childhood. Child Development, 79, 1395‐1414. Frick, P.J., Ray, J.V., Thornton, L.C., & Kahn, R.E. (2014). Annual Research Review: A developmental psychopathology approach to understanding callous‐unemotional traits in children and adolescents with serious conduct problems. Journal of Child Psychology and Psychiatry, 55, 532‐548. Hyde, L.W., Waller, R. and Burt, S.A. (2014). Commentary: Improving treatment for youth with callous‐unemotional traits through the intersection of basic and applied science – reflections on Dadds et al. (2014). Journal of Child Psychology and Psychiatry, 55, 781–783. Reid, M. J., Webster‐Stratton, C., & Baydar, N. (2004). Halting the development of conduct problems in Head Start children: The effects of parent training. Journal of Clinical Child and Adolescent Psychology, 33, 279‐291. Waller, R., Hyde, L.W., Grabell, A., Alves, M.A., & Olson, S.L. (2014). Differential associations of early callous‐ unemotional, ODD, and ADH behaviors: multiple domains within early‐starting conduct problems? Journal of Child Psychology and Psychiatry, in press This brief is a summary of research presented at the 21st World Meeting of the International Society for Research on Aggression. Support for the development of this research brief was provided by the Centers for Disease Control and Prevention (CDC). The findings and conclusions in this brief are those of the authors and do not necessarily represent the official position of the CDC. This project was supported by Grant #2012‐JF‐FX‐0062 awarded by the Office of Juvenile Justice and Delinquency Prevention, Office of Justice Programs, U.S. Department of Justice. The opinions, findings, and conclusions or recommendations expressed in this publication are those of the author and do not necessarily reflect those of the Department of Justice.asadfsdf