Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Managing Colon cancer in the era of
molecular markers
Dr B.R.Das
President, Research and Innovation
SRL Ltd, Mumbai
INDIA
1
Top 3 cancers
Alarming cancer stats in India
Mortality Rate
In India, 70% of diagnosed patients die in first year due to late diagnostics.
India also has some of the highest incidences in the world for certain cancers
including: cervical, gall bladder, oral and pharynx.
Molecular markers: Role
Molecular markers in colon cancer
K/N RAS
BRAF
PIK3CA
Let’s understand their role in CRC
Anti-EGFR Therapy is given to patient’s
with Metastatic Colorectal Carcinoma
??
?
???
What happens to the remaining patients? Why they do not
respond???
KRAS, NRAS, BRAF, PIK3CA :
Clinical Significance
3-10%
BRAF Gene
Mutations – Non
Responders/Worst
Prognosis
30-50%
KRAS Gene
Mutations / 3%
NRAS mutations
– Non Responders
12% PIK3CA and
other Gene
Mutations – Non
Responders
Combined KRAS, NRAS, BRAF and PIK3CA gene mutations explains ~ 62% of the
non-responders
The American Society of Clinical Oncology (ASCO) and the NCCN) both recommend KRAS
mutation testing prior to prescribing EGFR antagonist therapy for patients with mCRC and state
that alternative therapy should be prescribed when mutations are detected.
J Clin Oncol. 2009;27:2091-2096
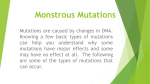
Suggested Algorithm for Testing
KRAS mutations
Negative
Positive
No Response
NRAS mutations
Negative
Positive
No Response
BRAF mutations
Negative
Positive
No Response
PIK3CA mutations
Positive
No Response
Negative
Response to anti-EGFR
likely
Specimen & Processing Steps
Paraffin Block
Unstained Sections on
Slides 3-4 nos
Tumor cells not
present
Sufficient Tumor cells
present
Test Not Performed
Cytology
DNA Extraction &
PCR
Pyrosequencing (kras)
BRAF, PIK3CA, MSI
Most Important critical point!!!
(Tumor heterogeneity)
Recommendation:
- Pathologists should determine the adequacy of specimens for
molecular testing by assessing cancer cell content and DNA quantity
and quality.
-Laboratories should test methods that are able to detect mutations in
specimens with at least 30-40% cancer cell content,
Tumor % and mutation detection
20% tumor
Expected mutation
Level (10%)
30% tumor
Expected mutation
Level (15%)
40% tumor
Expected mutation
Level (20%)
Technologies available
- 96 samples
- 20% mutant limit
- Laborious
- 9-12 hours
- Cheaper
Sanger Sequencing
- 96 samples
- 5% mutant limit
- Easy handling
- 3-4 hours
- Expensive
Real Time PCR
- 24 samples
- 5-10% mutant limit
- Easy workflow
- 10 to 40 mins
- Cost effective
Pyrosequencing
DNA quality assessment
DNA
Nucleic acid
PCR and Pyrosequencing
Pyrogram
Codon 12,13 (Not Detected)
GGT>GAT codon 12 (Detected)
Use of conventional molecular markers:
Is there a need to go beyond?
- KRAS extended panel
- NRAS extended panel
- MMR and MSI testing
- OncotypeDX (Upcoming)
- CTC/Liquid Biopsy (Upcoming)
KRAS/NRAS extended panel
What’s New and Different?
•
Currently, KRAS exon 2 (codon 12, 13) ; exon 3 (codon 61).
Extended-KRAS exons 3 (codon 59) and 4 (codons 117
and 146)
•
Currently, NRAS exon 2 (codon 12, 13) ; exon 3 (codon 61).
Extended -NRAS exons 3 (codon 59), and 4 (codons 117
and 146)
ASCO – 2015 Recommendations
KRAS/NRAS extended mutation screening is a must
before giving anti-EGFR therapy
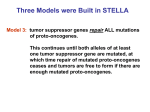
Why extended panels?
• 20% of the KRAS exon 2 non-mutated
tumors harbored one of the extended
RAS mutations
Anti-EGFR therapy
Progression Free Survival
Overall Survival
J Clin Oncol;33 (2015)
Multigene expression profile and
cancer treatment decision
The challenge: Which stage II colon cancer
patients should receive adjuvant chemotherapy?
Some facts to be known for stage II colon cancer
• Generally, Not all colon cancer patients are given chemotherapy,
especially early stage (II and IIIA,B)
• Because, they can be managed by simple surgery and
chemotherapy is not required (low risk of recurrence)
• However, some of them do need chemotherapy because they have
high risk of metastasis (high risk of recurrence)
• Chemo has significant toxicity and impacts quality of life
….This is the treatment dilemma
High Risk is based on MMR (Proficient), T stage (T4), Tumor grade (High),
No. of nodes examined (>12)
Low risk
•The continuous RS will have the greatest clinical utility for T3, MMRproficient patients, who constitute the majority of stage II colon cancer
(~70% of pts)
•New paradigm for quantitative assessment of recurrence risk in stage II colon cancer,
•emphasizing the role of three measures, Recurrence Score, MMR/MSI, and T stage
Circulating Tumour DNA (ctDNA)
• ctDNA is tumour DNA
that has been shed into
the bloodstream
• ctDNA can be present in
0.01% - >90% of the total
Cell Free DNA (cfDNA)
• The amount of ctDNA is
related to the tumour
burden and varies
between patients with
different clinical
presentations
Diaz and Bardelli, 2014 Journal of Clincial Oncology 32
Workflow
Blood sample taken
in Cell Save
preservative tubes
Set up:
Pyrosequencing
Next-generation
sequencing
Quantative PCR
BEAMing
Digital PCR
Sample arrives in lab
and spun to isolate the
plasma
ctDNA is
extracted from
the plasma using
the QIAamp
Circulating
Nucleic Acid on
the QIAVac
system
Plasma is stored at -80ºc
Sample is
extracted on the
same day as the
downstream
process set up
due to ctDNA
instability
Concluding remarks
• Molecular markers plays a critical role in therapeutic decision
making (~ 70% of non-responders)
• RAS mutational testing of colorectal carcinoma tissue should be
performed for patients who are being considered for anti-EGFR
therapy. This analysis must include KRAS and NRAS codons 12, 13
of exon 2; 59, 61 of exon 3; and 117 and 146 of exon 4 ("expanded"
or "extended" RAS).
• dMMR/MSI testing must be performed in all colorectal cancers for
prognostic stratification and identification of Lynch syndrome
patients.
And we are
here..
Many more to explore….
Thank you