Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
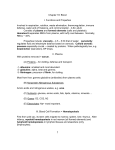
Clinical Studies Difference Between Human Red Blood Cell Na + -Li + Counter transport and Renal Na + -H + Exchange ANDREW M. KAHN Downloaded from http://hyper.ahajournals.org/ by guest on June 18, 2017 SUMMARY Several laboratories have reported that the activities of sodium-lithium countertransport are increased in red blood cells from patients with essential hypertension. Based on the many similarities between this transport system and the renal sodium-proton exchanger, a hypothesis has been put forth in the literature that increased red blood cell sodium-lithium counter-transport activity may be a marker for increased sodium-proton exchange activity in the renal proximal tubule. The present studies were designed to test the hypothesis that sodium-lithium countertransport in red blood cells from humans or rabbits is mediated by the same transport mechanism that mediates sodiumproton exchange in the renal brush border from those species. Similar to what has been reported for the rabbit, the present studies show that an amiloride-sensitive sodium-proton exchanger is present in human renal brush border vesicles. However, Na+-Li+ countertransport in human and rabbit red blood cells, assayed under several different conditions, was not inhibited by amiioride. In agreement with what has been reported for humans, the present studies show that extracellular proton-stimulated sodium efflux is inhibited by amiioride in rabbit red blood cells. These data demonstrate a difference (amiioride sensitivity) between the red blood cell sodium-lithium countertransporter and the renal brush border sodium-proton exchanger in humans and rabbits. These experiments detract from the hypothesis that increased red blood cell sodium-lithium countertransport activity in patients with essential hypertension is a marker for increased sodium-proton exchange activity In the renal brush border. (Hypertension 9: 7-12, 1987) KEY WORDS • amiioride • brush border vesicles • rabbit red blood cells M ANY studies have examined whether an abnormality in red blood cell (RBC) sodium transport is linked to essential hypertension.1"6 An underlying hypothesis in these studies is that an abnormality in a specific RBC sodium transport system may be a marker for a similar abnormality in the same transport system located in another tissue. For instance, elevated activity of a specific sodium influx pathway in RBCs from patients with essential hypertension could be a marker for increased sodium influx by that same pathway across the luminal membrane of certain renal tubular cells or the sarcolemma of vascular smooth muscle. Such a transport defect in From the Department of Medicine, University of Texas Medical School, Houston, Texas. Supported by a grant-in-aid from the American Heart Association, Texas Affiliate. Address for reprints: Andrew M. Kahn, M.D., 4.138 MSMB, University of Texas Medical School, P.O. Box 20708, Houston, TX 77025. Received January 6, 1986; accepted July 23, 1986. the cell membrane of these cell types could be related to the development or maintenance of hypertension. The cell membrane of RBCs from humans and a variety of mammals mediates Na + -Li + countertransport.7"9 This is an electroneutral transport system that can operate in a sodium-for-lithium or sodium-forsodium exchange mode.7"9 Several laboratories have reported that the activities of this transport system are elevated in RBCs from patients with essential hypertension.2' 5> 6 Since lithium is only present in very low concentrations in humans, this RBC transport system, or its equivalent in other cell types, would be expected to mediate Na + -Na + exchange.9 An increased activity of Na + -Na + exchange would not alter net sodium transport in any tissue. Aronson10 and Funder et al." have independently suggested that RBC Na + -Li + countertransport may be an operative mode of a sodium-proton exchange transport system. This hypothesis is based on the many similarities between RBC Na + Li + countertransport and renal brush border Na + -H + exchange. Both transport systems are quinidine-inhibi- 8 HYPERTENSION Downloaded from http://hyper.ahajournals.org/ by guest on June 18, 2017 table,7-12 electroneutral monovalent cation exchangers 89 ' 13 with affinities for sodium and lithium,7"9' l3~13 greater affinity for lithium than sodium,8' M and no affinity for choline, cesium, rubidium, or potassium.7' l3~15 Increased activity of Na+-Li+ countertransport in RBCs from hypertensive patients has been proposed as a marker for increased activity of renal brush border Na + -H + exchange.1'l0'16 Such an abnormality in the brush border membrane could be responsible for increased proximal tubular sodium reabsorption, which could contribute to the hypertensive state.17' " This is an attractive proposal that would be greatly strengthened if the aforesaid transport activities from both tissues were indeed mediated by the same system. These studies were designed to test the hypothesis that Na + -Li + countertransport in RBCs is mediated by the same transport system that mediates Na + -H + exchange in the renal brush border membrane. The results demonstrate a difference between these two transport systems. Materials and Methods Human Brush Border Vesicles Kidney tissue was obtained from fresh human kidneys immediately after surgical removal from patients Withrenalcancer. Brush border vesicles were prepared by a magnesium aggregation and differential centrifugation technique that was similar to the method used by this laboratory to prepare rat renal brush border vesicles." Normal portions of human renal cortex were minced with a razor blade and homogenized with 10 strokes in a glass-teflon homogenizer in (in mM) 200 mannitol, 50 Tris, 80 HEPES, pH 7.5 (4 ml/g tissue). Then, MgSO4 was added to the cortical homogenate to a final concentration of 10 mM, and the homogenate was incubated on ice for 20 minutes. The homogenate was centrifuged at 4340 g for 10 minutes, and the supernatant was centrifuged at 27,000 g for 25 minutes. The resultant pellet was resuspended in homogenizing solution with 10 mM MgSO4 and centrifuged at 5900 g for 10 minutes, and the supernatant was centrifuged at 27,000 g for 25 minutes. The resultant pellet was resuspended in homogenizing solution with 10 mM MgSO4 and centrifuged at 7710 g for 10 minutes. The resultant supernatant was centrifuged at 27,000 g for 25 minutes, and the pellet was resuspended in homogenizing solution with 10 mM MgSO4 to a final protein concentration of 10 to 15 mg/ml. Protein was measured by the method of Lowry.20 The activities of the brush border membrane marker alkaline phosphatase and the basolateral membrane marker Na+,K+-ATPase were determined for the cortical homogenate andfinalvesicles, as previously described." Alkaline phosphatase activity in the vesicles was enriched ninefold relative to the cortical homogenate, while Na+,K+-ATPase activity was enriched by only 25%. Hence, the human renal vesiclesrepresentedprimarily brush border membranes. The vesicles were preincubated with the desired solutions for 90 minutes at 22 °C before the sodium trans- VOL 9, No 1, JANUARY 1987 port experiments. The timed uptake of 1 mM ^Na was measured in triplicate by a rapid Millipore (Bedford, MA, USA) filtration and washing technique, as previously described.21 The composition of the preincubation and incubation media are given in the legend to Figure 1. This experiment was performed with at least three separate vesicle preparations. RBC Cation Transport To determine RBC cation transport, fresh blood was drawn into a heparinized syringe from the antecubital vein of a human volunteer or from the central ear artery of an adult male New Zealand White rabbit. The whole blood was centrifuged at 5000 g for 5 minutes at 4°C, and the plasma and buffy coat were removed. The efflux of lithium or sodium from human or rabbit RBCs was measured by methods modified from Canessa et al.2 and are described in entirety as follows. One volume of packed RBCs was incubated in a shaking water bath for 3 hours at 37 °C withfivevolumes of (in mM) 10 glucose, 10 Tris morpholinepropanesulfonic acid (MOPS), pH 7.4, and 150 LiCl or 150 NaCl plus 0.1 ouabain. The cells were centrifuged at 5000 g for 5 minutes at 4°C, and the packed cells were resuspended in ice-cold washing solution that contained (in mM) 75 MgCl2, 85 sucrose, 10 glucose, and 10 Tris MOPS, pH 7.4. This suspension was centrifuged at 5000 g for 5 minutes at 4°C, andfivesuccessive identical washing and centrifuging steps were performed to remove extracellular lithium or sodium. The hematocrit of the washed suspension was measured. The efflux of lithium or sodium from the preloaded washed RBCs was initiated by incubating cells at 37 °C with different external media. At time zero and at specified intervals thereafter, three 1-ml aliquots from each suspension were pipetted into individual ice-cold plastic centrifuge tubes. These tubes were immediately centrifuged at 5000 g for 3 minutes at 4°C, and the supernatants removed and stored in plastic tubes. The lithium or sodium concentrations of the supernatants were measured with a Corning 450flamephotometer (Corning Scientific Instruments, Medfield, MA, USA). The mean concentration of cation in the initial supernatants was subtracted from the mean concentrations in the subsequent supernatants, and the efflux of lithium or sodium into the different external media was calculated and expressed as millimoles per liter of RBCs. The effect of Na,, on lithium efflux was measured by incubating lithium-loaded RBCs with 150, 25, or 0 mM NaCl and 0.1 mM ouabain, pH 7.4. The effect of Li0 on sodium efflux was measured by incubating sodium-loaded RBCs with 5, 1, 0.5, or 0 mM LiCl and 0.1 mM ouabain, pH 7.4. In all cases, choline chloride was added where necessary to maintain extracellular salt concentration at 150 mM. The effect of extracellular acidity on Na efflux was measured by incubating Na-loaded RBC with (in mM) 150 choline chloride, 0.1 ouabain, 10 Tris MOPS, pH 7.4, or 10 Tris morpholineethanesulfonic acid, pH 6.0. In addition, 4,4'diisothiocyano-2,2'-disulfonic stilbene (DIDS) was present in the external media (0.125 mM) to help maintain the imposed pH gradients. All efflux expert- RED BLOOD CELL Na+-Li+ AND RENAL Na+-H+ COUNTERTRANSPORT/tfa/in ments were performed in the presence and absence of 1 mM amiloride. The exact composition of the external media is given in the legends to Figures 2 through 5. Each RBC transport experiment was performed on at least three separate occasions. Materials The n N a (200 AiCi/>g Na) was obtained from Amersham (Arlington Heights, IL, USA) and DIDS from Sigma Chemical (St. Louis, MO, USA). Amiloride HCl was a gift from Merck Sharp Dohme (West Point, PA, USA). All other chemicals were reagent grade. Downloaded from http://hyper.ahajournals.org/ by guest on June 18, 2017 Results Brush Border Na+-H+ Exchange In the presence of an outwardly directed proton gradient (pHta = 5.7, p H ^ = 7.4), the 10-second uptake of 1 mM H Na in human brush border vesicles was stimulated sevenfold as compared with the absence of a pH gradient (pH^ = p H ^ = 7.5). As shown in Figure 1, sodium uptake in the presence of an outwardly directed proton gradient was stimulated up to and including the 1-minute time point. At the 90-minute equilibrium time point, sodium uptake in control and acid-loaded vesicles was the same. When 1 mM amiloride was added to the incubation medium in the presence of an outwardly directed proton gradient, the stimulation of sodium uptake was inhibited. These data indicate that human renal brush border vesicles mediate Na + -H + exchange and that amiloride can inhibit the Na + -H + exchanger in these vesicles. RBC Na+-Li+ Countertransport The efflux of lithium from human RBCs into different external media was measured and plotted in Figure 2. The rates of lithium efflux into external media containing sodium were greater than the efflux rate into the sodium-free medium. The increment in lithium efflux rate caused by the presence of external sodium represents the activity of Na + -Li + countertransport. The rates of lithium efflux into media containing 150, 25, or 0 mM NaCl were not affected by 1 mM amiloride. Thus, the activity of Na + -Li + countertransport in human RBCs in the presence of 150 or 25 mM Nao was not inhibited by 1 mM amiloride. Rabbit RBCs were also preloaded with lithium, washed, and incubated with the same external media as the human RBCs. As shown in Figure 3, 1 mM amiloride did not inhibit rabbit RBC Na + -Li + countertransport in the presence of 150 or 25 mM external sodium. RBC Li+-Na+ Countertransport The Na efflux from rabbit RBCs was measured in the presence and absence of 1 mM amiloride and various concentrations of external lithium. The sodium efflux rate into lithium media minus the efflux rate into lithium-free media was taken as the activity of Li + Na + countertransport. As shown in Figure 4, the presence of 1 mM amiloride in the external media did not inhibit the activity of Li + -Na + countertransport in the presence of 5, 1, or 0.5 mM external lithium. Proton-Stimulated Na Efflux 7 4 0 / 5 7, Rabbit RBCs were preloaded with sodium and washed, and the efflux of sodium was measured in sodium-free and lithium-free external solutions at various pH concentrations, in the presence and absence of 06 £ 1 -. o m | 05 150 Na0 0.4 o I 0.3 125 chohne0 Minutes 150 cholineu 0.1 FIGURE 1. Effect of a pH gradient and amiloride on sodium uptake in human renal brush border vesicles (*). Vesicles were preincubatedfor 90 minutes at 22 °C in (in mM) 196 mannitol, 2 MgSO4, 50 Tris, 80 HEPES, pH 7.5, and the uptake of 1 mM u Na was assayed at 37"C in the presence of (in mM) 199 mannitol, 0.4 MgSO4, 50 Tris, 80 HEPES, pH 7.5. Vesicles were preincubated for 90 minutes at 22 "C with (in mM) 260 mannitol, 2 MgSO4, 10 Tris, 16 HEPES, 40 morpholineethanesulfonic acid (MES), pH 5.7, and the uptake of 1 mM ^Na was assayed at 37°C in the presence of (in mM) 212 mannitol, 0.4 MgSO4, 42 Tris, 67 HEPES, 8 MES, pH 7.4, with (A) or without (*) 1 mM amiloride. Data presented are the results from a representative experiment. 30 60 90 Minutes FIGURE 2. Effect of amiloride on Na + -Li* countertransport in human RBCs. Human RBCs were preloaded with lithium, and the efflux of lithium at 37"C was assayed by incubating the cells in media containing (in mM) 4 MgCl2, 4 sucrose, 10 glucose, 0.1 ouabain, 10 Tris morpholinepropanesulfonic acid, pH 7.4, and 150 NaCl (O •), 25 NaCl and 125 choline chloride (O, • ) , or 150 choline chloride (A, A), with (• • A.) or without (o, a, A) 1 mM amiloride. Data presented are the results of a representative experiment. HYPERTENSION 10 VOL 9, No 1, JANUARY 1987 1 5 80 | | Control Y/ \ 1 mM Amilonde 60 •S io tf>, 150 Na. §4.0 II o — I 0.5 20 5 mM L i . 1 mM L i . 0.5 mM LiD Minutes Downloaded from http://hyper.ahajournals.org/ by guest on June 18, 2017 FIGURE 3. Effect of amiloride on Na +-Li+ countertransport in rabbit RBCs. Lithium transport in rabbit RBCs was measured as described for human RBCs in the legend for Figure 2. Data presented are the results of a representative experiment. 1 mM amiloride. As shown in Figure 5, the efflux of sodium was stimulated when the external pH was lowered from 7.4 to 6.0. As also shown in Figure 5, the stimulation of sodium efflux by external protons was inhibited by 1 mM amiloride. Discussion In a number of studies, the activities of Na+-Li+ countertransport in RBCs from patients with essential hypertension were elevated.2'3> 6 The relation between thesefindingsand elevated arterial pressure is obscure. It has been suggested that RBC Na+-Li+ countertransport may be mediated by the same transport system as renal brush border Na + -H + exchange. 11016 If this were the case, increased RBC Na+-Li+ countertransport activity could be a marker for increased Na + -H + exchange activity in the brush border membrane of the proximal tubule. Such an abnormality could cause increased proximal tubular reabsorption of salt and water, which could lead to a series of events resulting in elevated blood pressure. "•" This attractive hypothesis would be strengthened if RBC Na+-Li+ countertransport and renal brush border Na + -H + exchange were indeed mediated by the same system. Much circumstantial evidence gives credence to this possibility. The purpose of the present studies was to test the hypothesis that Na+-Li+ countertransport in RBCs from humans and rabbits is mediated by the same transport system that mediates Na + -H + exchange in the renal brush border membrane from those species. Data are presented that demonstrate that renal brush border vesicles from the human kidney mediate amiloride-sensitive Na + -H + exchange. Previous studies with renal brush border vesicles from the rabbit have reached the same conclusion.1322 The present studies could not demonstrate the amiloride sensitivity of Na+-Li+ countertransport in RBCs from humans or rabbits. In the rabbit RBCs, inhibition of countertransport by amiloride was not observed when the transport FIGURE 4. Effect of amiloride on Li+-Na+ countertransport in rabbit RBCs. Rabbit RBCs were preloaded with sodium, and the efflux of sodium was assayed by incubating cells for 15 minutes at 37"C with external solutions containing (in mM) 4 MgCl2, 4 sucrose, 10 glucose, 0.1 ouabain, 10 Tris morpholinepropanesulfonic acid, pH 7.4, and 5, 1, 0.5, or 0 IACI, with or without 1 mM amiloride. Choline chloride was present such that external salt concentration was 150 mM. The Li+-Na + countertransport activity was calculated as the rate of sodium efflux into lithium media minus the rate into lithium-free media. Data are the means ± SE of three experiments. 30 a. 20 ^m 6 0 + amclonde 74 7.4 + amiloride 1.0 15 30 Minutes 45 60 FIGURE 5. Effects of extracellular acidity and amiloride on sodium efflux in rabbit RBCs. The RBCs were preloaded with sodium, and the efflux of sodium was measured by incubating the cells in media containing (in mM) either 4 MgCl2, 4 sucrose, 10 glucose, 150 choline chloride, 0.1 ouabain, 0.125 4,4' -diisothiocyano-2,2' -disulfonic stilbene, and 10 Tris, morpholinepropanesulfonic acid, pH 7.4 (o, 9), or 10 Tris morpholineethanesulfonic acid, pH 6.0 (O, *), with C, U) or without (o, O) 1 mM amiloride. Data presented are the results of a representative experiment. system operated in a Lita for Na^ mode or a Nata for Li^, mode. These findings suggest that RBC Na+-Li+ countertransport and renal brush border Na + -H + exchange are different transport systems. Nevertheless, the same system may indeed be responsible for these RED BLOOD CELL Na+-Li+ AND RENAL Na+-H+ COUNTERTRANSPORT/tfaAn Downloaded from http://hyper.ahajournals.org/ by guest on June 18, 2017 two transport activities, but amiloride is not able to effectively inhibit cation transport in the RBC membrane. This possibility seems unlikely since an amiloride-sensitive Na + -H + exchanger has been found in the RBC membrane from humans, dogs, and amphiuma.23-2* Although Na + -H + exchange is not demonstrable under normal conditions in these cells, an elevation in intracellular calcium24 or a decrease in cell volume23-M clearly brings out this amiloride-sensitive cation translocation pathway. The present studies demonstrate that amiloride can also inhibit sodium transport in the rabbit RBC membrane. As shown in Figure 5, sodium efflux, which was stimulated by external protons, was abolished by 1 mM amiloride. Amiloride is a competitive inhibitor of Na + -H + exchange in the renal brush border membrane.22 An inherent property of a competitive inhibitor is that a fixed concentration of inhibitor will become less effective as the substrate concentration is raised. It is important to consider whether the failure of 1 mM amiloride to inhibit RBC Na + -Li + countertransport in these studies was due to such kinetic restraints, rather than to an actual lack of sensitivity to amiloride. Indeed, amiloride is not an effective inhibitor of the Na + -H + exchanger in the presence of physiological concentrations of sodium.27 The \DK of amiloride for the human RBC Na + -H + exchanger has been estimated to be about 17 /iM. 24 If human RBC Na + -Li + countertransport and human RBC Na + -H + exchange are mediated by the same process, then Michaelis-Menton inhibition kinetics predict that 1 mM amiloride should inhibit Na + -Li + countertransport by about 97% when the external sodium concentration equals its Km value (25 mM). 8 Figure 2 shows that amiloride did not inhibit human RBC Na + -Li + countertransport activity under these conditions. Figure 5 shows that about 90% of external proton-stimulated sodium efflux from rabbit RBCs was inhibited by 1 mM amiloride. Thus, the KK of amiloride for this process is less than 0.11 mM. If rabbit RBC Na + -Li + countertransport and external proton-stimulated sodium efflux are mediated by the same process, then 1 mM amiloride should inhibit Na + -Li f countertransport by at least 82% when the external sodium concentration is less than its Km value (50 mM). 9 Figure 3 shows that amiloride did not inhibit rabbit RBC Na + -Li + countertransport activity under these conditions. Thus, the failure of amiloride to inhibit RBC Na + -Li + countertransport probably was not due to kinetic restraints imposed by the external sodium and amiloride concentrations used in these studies. One must consider the possibility, however, that Na + H + exchange and Na + -Li + countertransport are indeed mediated by the same system, but that the affinity for amiloride is absent or greatly reduced when the system operates in a sodium for lithium exchange mode. The present studies have not ruled out this possibility. Jennings et al.28 recently reported studies designed to determine whether the rabbit RBC Na + -Li + countertransport system can also mediate Na + -H + exchange. These authors found that Na + -Na + exchange, an operative mode of the Na + -Li + countertransport system,9 occurred at a velocity over 10 mmol Na/L 11 RBC/hr in rabbit RBCs. Despite this brisk transport rate, little stimulation of sodium efflux into sodiumfree media was observed when extracellular pH was reduced from 7.5 to 6.9. These authors concluded that rabbit RBC Na + -Na + (or Na + -Li + ) countertransport does not function appreciably in a Na + -H + exchange mode.28 The experimental conditions and results of the present study are different from those of Jennings et al.28 In the present study, amiloride-inhibitable sodium efflux from rabbit RBCs was stimulated by reducing extracellular pH from 7.4 to 6.0. The difference in the ability of external protons to stimulate sodium efflux in the present studies and those of Jennings et al.28 is not known, but it may be related to the larger increase in external proton concentration in the present study. Despite the differences in experimental conditions between the present study and that of Jennings et al. ,M the conclusions are the same: the RBC Na + -Li + countertransport system probably is not the Na + -H + exchanger. The hypothesis that elevated Na + -Li + countertransport activity in RBCs from patients with essential hypertension is a marker for elevated Na + -H + exchange activity in the renal brush border membrane1'i0> 16 would be a more attractive possibility if the two transport activities were mediated by the same system. The present studies detract from this hypothesis. Since Na + -H + exchange in sarcolemmal vesicles from vascular smooth muscle is inhibitable by amiloride,29 the present data also detract from the recent suggestion by Funder et al." that elevated Na + -Li + countertransport activity may be a marker for increased vascular smooth muscle Na + -H + exchange activity." On the other hand, a physicochemical disturbance may exist in cell membranes throughout the bodies of patients with essential hypertension. Such a global membrane abnormality might increase the activities of both RBC Na + Li + countertransport and renal brush border Na + -H + exchange, even if the two transport systems were distinct. If this were the case, RBC transport activity would be a marker for renal brush border transport activity. In support of this possibility, Weder30 recently has reported that RBC Na + -Li + countertransport activity was increased and renal fractional lithium clearance was decreased in patients with essential hypertension. The finding that renal lithium clearance was decreased suggests that proximal tubular sodium reabsorption by the brush border Na + -H + exchanger was increased in the hypertensive patients described by Weder.30 Further studies are necessary to confirm the relation between RBC Na + -Li + countertransport and renal brush border Na + -H + exchange. The present studies demonstrate a difference between these two transport systems. The relation between RBC Na + -Li + countertransport and the hypertensive process remains obscure. Acknowledgments The author expresses gratitude to Drs. Michael Boileau and Stuart Flechner for the provision of human kidneys. The author acknowledges the excellent technical assistance of Brian Lee and the secretarial assistance of Ms. Nhung Le. 12 HYPERTENSION References Downloaded from http://hyper.ahajournals.org/ by guest on June 18, 2017 1. Blaustein MP. Sodium transport and hypertension: where are we going? Hypertension 1984;6:445-453 2. Canessa M, Adragna N, Solomon H, Connolly T, Tosteson DC. Increased sodium-lithium countertransport in red cells of patients with essential hypertension. N Engl J Med 1980; 302:772-776 3. Davidson J, Opie L, Keding B. Sodium-potassium cotransport activity as a genetic marker in essential hypertension. Br Med J 1982284:539-541 4. Garay R, Meyer P. A new test showing abnormal net Na + and K + fluxes in erythrocytes of essential hypertensive patients. Lancet 1979; 1:349-352 5. Smith JB, Ash KO, Hunt SC, et al. Three red cell sodium transport systems in hypertensive and normotensive Utah adults. Hypertension 1984;6:159-166 6. Woods JW, Falk RJ, Pittman AW, Klemmer PJ, Watson BS, Namboodiri K. Increased red-cell sodium-lithium countertransport in normotensive sons of hypertensive parents. N Engl J Med 1982;3O6:593-595 7. Panday GN, Sarkadi B, Haas M, Gunn RB, Davis JM, Tosteson DC. Lithium transport pathways in human red blood cells. J Gen Physiol 1978;72:233-247 8. Sarkadi B, Alifimoff JK, Gunn RB, Tosteson DC. Kinetics and stoichiometry of Na-dependent Li transport in human red blood cells. J Gen Physiol 1978;72:249-265 9. Duhm J, Becker BF. Studies on lithium transport across the red cell membrane: on the nature of the Na+-dependent Li + countertransport system of mammalian erythrocytes. J Membr Biol 1979:51:263-286 10. Aronson PS. Red-cell sodium-lithium countertransport and essential hypertension. N Engl J Med 1983;307:317 11. Funder J, Wieth JO, Jensen HA, Ibsen KK. The sodium/lithium exchange mechanism in essential hypertension: is it a sodium/proton exchanger? In: Villarreal H, Sambhi MP, eds. Topics in pathophysiology of hypertension. The Hague, The Netherlands: Nijhoff 1984:147-161 12. Mahnensmith RL, Louklis P, Aronson PS. Quinidine inhibition of the Na-H exchanger in renal microvillus membrane vesicles. Kidney Int 1984;25:309 13. Kinsella JL, Aronson PS. Properties of the Na + -H + exchanger in renal microvillus membrane vesicles. Am J Physiol 1980; 238:F461-F469 14. Kinsella JL, Aronson PS. Interaction of N>L,+ and Li + with the renal microvillus membrane Na + -H + exchanger. Am J Physiol 1981;241:C220-C226 VOL 9, No 1, JANUARY 1987 15. Duhm J, Eisenried F, Becker BF, Greil W. Studies on lithium transport across the red cell membrane: Li uphill transport by the Na-dependent Li countertransport system of human erythrocytes. Pfluegers Arch 1976;364:147-155 16. Mahnensmith RL, Aronson PS. The plasma membrane sodium-hydrogen exchanger and its role in physiological and pathophysiological processes. Circ Res 1985^57:773-788 17. de Wardener HE, MacGregor GA. Darn's hypothesis that a saluretic substance may be responsible for a sustained rise in arterial pressure: its possible role in essential hypertension. Kidney Int 1980;18:l-9 18. Haddy FJ. Mechanism, prevention and therapy of sodiumdependent hypertension. Am J Med 198O;69:746-758 19. Kahn AM, Branham S, Weinman EJ. Mechanism of urate and p-aminohippurate transport in rat renal microvillus membrane vesicles. Am J Physiol 1983;245:F151-F158 20. Lowry OH, Rosebrough NJ, Farr AL, Randall RJ. Protein measurement with the Folin reagent. J Biol Chem 1951; 193:265-275 21. Aronson PS, Bounds SE. Harmaline inhibition of Na-dependent transport in renal microvillus membrane vesicles. Am J Physiol 1980;238:F210-F217 22. Kinsella JL, Aronson PS. Amiloride inhibition of the Na+-H+ exchanger in renal microvillus membrane vesicles. Am J Physiol 1981;241:F374-F379 23. Escobales N, Canessa M. Evidence for a Na-H exchange system in human red cells [Abstract]. Biophys J 1985;47:157a 24. Escobales N, Canessa M. Ca-activated Na fluxes in human red cells, amiloride sensitivity. J Biol Chem 1985;260: 11914-11923 25. Parker JC, Castranova V. Volume-responsive sodium and proton movements in dog red blood cells. J Gen Physiol 1984; 84:379-401 26. Cala PM. Volumeregulationby amphiuma red blood cells: the membrane potential and its implicationsregardingthe nature of the ion-flux pathways. J Gen Physiol 1980;76:683-708 27. Benos DJ. Amiloride: a molecular probe of sodium transport in tissues and cells. Am J Physiol 1982;242:C131-C145 28. Jennings ML, Lackey MA, Cook KW. Absence of significant sodium-hydrogen exchange by rabbit erythroevte sodium-lithium countertransporter. Am J Physiol 1985;249:C63-C68 29. Kahn AM, Shelat H, Allen JC. Na+-H+ exchange is present in sarcolemmal vesicles from dog superior mesenteric artery. Am J Physiol 1986;250:H313-H319 30. Weder AB. Red cell lithium-sodium countertransport and renal lithium clearance in hypertension. N Engl J Med 1986;314: 198-201 Difference between human red blood cell Na+-Li+ countertransport and renal Na+-H+ exchange. A M Kahn Hypertension. 1987;9:7-12 doi: 10.1161/01.HYP.9.1.7 Downloaded from http://hyper.ahajournals.org/ by guest on June 18, 2017 Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1987 American Heart Association, Inc. All rights reserved. Print ISSN: 0194-911X. Online ISSN: 1524-4563 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://hyper.ahajournals.org/content/9/1/7 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Hypertension is online at: http://hyper.ahajournals.org//subscriptions/