Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
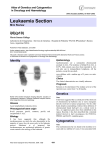
Case Report Early diagnosis of childhood Acute lymphoblastic leukemia Vanitha Pandey1, Mahesh Kumar K2, Indira3 1,2 Assistant Professor, 3Professor & Head, Department of Pathology, Malla Reddy Institute of Medical Sciences, Suraram, Hyderabad , Telangana, India. Address for Correspondence: Dr. Kandukuri Mahesh Kumar, Assistant professor, Department of Pathology, Malla Reddy Institute of Medical Sciences, Suraram, Hyderabad, Telangana, India. Email id: [email protected] ABSTRACT Acute lymphoblastic leukemia (ALL) is characterized by an overproduction of immature white blood cells, called lymphoblasts or leukemic blasts. These cells crowd the bone marrow, preventing it from making normal blood cells. They can also spill out into the blood stream and circulate around the body. Due to their immaturity, these cells are unable to function properly to prevent or fight infection. Inadequate numbers of red cells and platelets being made by the marrow cause anemia, and easy bleeding and bruising. ALL is the most common type of childhood leukemia, and the most common childhood cancer. It is more common in males than in females. The exact causes of ALL remain largely unknown but it is thought to result from mutations in one or more of the genes that normally control blood cell development. Chemotherapy is the main form of treatment for ALL. A combination of drugs, including steroids, is usually given in several cycles with a rest period of a few weeks in between. Initially, the aim of treatment is to destroy leukemic cells and induce a remission. Keywords: Acute Lymphoblastic Leukemia, Subleukemic leukemia, Atypical Lymphocytes, CD-20, Bone Marrow. INTRODUCTION Acute lymphoblastic leukemia (ALL) is a type of cancer of the blood and bone marrow, the spongy marrow tissue inside the bones where blood cells are made. Acute lymphoblastic leukemia, also known as acute lymphocytic leukemia or acute lymphoid leukemia (ALL), is an acute form of leukemia, or cancer of the white blood cells, characterized by the overproduction and accumulation of cancerous, immature white blood cells, known as lymphoblasts . The word "acute" in acute lymphoblastic leukemia comes from the fact that the disease progresses rapidly and creates immature blood cells, rather than mature ones. The word "lymphoblasts" in ALL refers to the white blood cells, which ALL affects. Acute lymphocytic leukemia is the most common type of cancer in children, and treatments result in a good chance for a cure. Acute lymphocytic leukemia can also occur in adults, though the chance of cure is greatly reduced. About 6,000 cases are reported in the United States every year 1. Internationally, ALL is more common in Caucasians than in Africans; it is more common in Hispanics and in Latin America2. Acute lymphocytic leukemia occurs when a bone marrow cell develops errors in 83 its DNA. The errors tell the cell to continue growing and dividing, when a healthy cell would normally stop dividing and eventually die. Signs and symptoms include recurrent infections, fever, bleeding gums, swollen lymph nodes, fatigue and organomegaly. We present a case of lymphoblastic leukemia in subleukemic phase with the total leukocyte count within normal range and with few atypical lymphocytes. CASE REPORT A 7 years old female child admitted with complains of fever more than a month, fatigue, loss of appetite, yellow discoloration of eyes and pain in the abdomen. Clinical examination showed massive hepatomegaly , pallor, continuous low grade fever and no enlarged lymph nodes. Investigations showed Hemoglobin 6.8 gm %, total leukocyte count (TLC) within normal limits and with 10 to 15 % of atypical lymphoid cells. Initial platelet count was 70,000 /cu.mm, later dropped to 20,000/cu.mm. Computerized Tomography (CT) scan abdomen showed hepatomegaly , splenomegaly , minimal ascites and collection in pouch of douglas (POD). Chest X-ray showed bilateral minimal pleural effusion. Provisional clinical diagnoses listed out were wilson’s disease, Non-Hodgkin’s lymphoma, viral hepatitis and dengue fever. Patient is been given supportive therapy and the pediatrician was asked to send daily sample for complete blood picture (CBP). On daily follow-up with CBP, we could find the atypical lymphoid cells increasing in number by 5- 10 % with the TLC within normal limits and bone marrow was advised. On day eight of the admission, bone marrow was done and the marrow showed more than 80% of the blasts (Figure 1). Diagnosis of Acute Lymphoblastic Leukemia (ALL- L2) was given. Further confirmation and CD-20 was done, which turned out to be positive in all the cells indicating B- cell origin (Figure 2). Figure 1:- Bone marrow aspirate showing Lymphoblasts Figure 2:- CD-20 Positive in bone marrow aspirate smears (Brown Color) Pandey, et al DISCUSSION Acute lymphoblastic leukemia (ALL) is a malignant (clonal) disease of the bone marrow in which early lymphoid precursors proliferate and replace the normal hematopoietic cells of the marrow. ALL may be distinguished from other malignant lymphoid disorders by the immunophenotype of the cells, which is similar to B- or T-precursor cells. The malignant cells of acute lymphoblastic leukemia (ALL) are lymphoid precursor cells (ie, lymphoblasts) that are arrested in an early stage of development. This arrest is caused by an abnormal expression of genes, often as a result of chromosomal translocations. The lymphoblasts replace the normal marrow elements, resulting in a marked decrease in the production of normal blood cells. Consequently, anemia, thrombocytopenia and neutropenia occur to varying degrees. The lymphoblasts also proliferate in organs other than the marrow, particularly the liver, spleen, and lymph nodes. A bone marrow study provides conclusive proof of ALL3. Although overall incidence is rare, leukemia is the most common type of childhood cancer. It accounts for 30% of all cancers diagnosed in children younger than 15 years. Epidemiologic studies of acute leukemias in children have examined possible risk factors, including genetic, infectious, and environmental, in an attempt to determine etiology. The environmental risk factors include ionizing radiation, nonionizing radiation, hydrocarbons, pesticides, alcohol use, cigarette smoking, and illicit drug use. Genetic conditions such as Down’s syndrome, Neurofibromatosis, Shwachman syndrome, Bloom syndrome, Ataxia telangiectasia are also found associated in many studies 4. Children with ALL are often divided into risk groups such as standard-risk, high-risk, or very high-risk, with more intensive treatment given to higher risk patients. Generally, children at low risk have a better outlook than those at very high risk. While all of the following are prognostic factors, only certain ones are used to determine which risk group a child falls into. (The first 2 factors – age at diagnosis and initial white blood cell count – are thought to be the most important.) It’s important to know that even children with some poor prognostic factors can often still be cured. Age at diagnosis: Children between the ages of 1 and 9 with B-cell ALL tend to have better cure rates. Children younger than 1 year and children 10 years or older are considered high-risk patients. The outlook in T-cell ALL isn’t affected much by age. Initial white blood cell (WBC) count: Children with ALL who have very high WBC counts (greater than 50,000 cells per cubic millimeter) when they are diagnosed are classified as high risk and need more intensive treatment. Typically, the higher the white blood cell count, the worse the prognosis5. Subtype of ALL: Children with pre-B, common, or early pre-Bcell ALL generally do better than those with mature B-cell leukemia. The outlook for T-cell ALL seems to be about the same as that for B-cell ALL as long as treatment is intense enough. 84 Gender: Girls with ALL may have a slightly higher chance of being cured than boys. Race/ethnicity: African-American and Hispanic children with ALL tend to have a lower cure rate than children of other races. Spread to certain organs: Spread of the leukemia into the cerebrospinal fluid, or to the testicles in boys, lowers the chance of being cured. Enlargement of the spleen and liver is usually linked to a high WBC count, but some doctors view this as a separate sign that the outlook is not as favorable. Number of chromosomes: Better prognosis observed in patients with hyperploidy. Chromosome translocations: Translocations occur when chromosomes swap some of their genetic material (DNA). Children whose leukemia cells have a translocation between chromosomes 12 and 21 are more likely to be cured. Those with a translocation between chromosomes 9 and 22 (the Philadelphia chromosome), 1 and 19, or 4 and 11 tend to have a less favorable prognosis6. Some of these “poor” prognostic factors have become less important in recent years as treatment has improved. Response to treatment: Children whose leukemia responds completely within 1 to 2 weeks of chemotherapy have a better outlook than those whose leukemia does not. Children whose cancer does not respond as well may be given more intensive chemotherapy. The earlier ALL is detected, the more effective the treatment. The aim is to induce a lasting remision, defined as the absence of detectable cancer cells in the body (usually less than 5% blast cells in the bone marrow).Treatment for acute leukemia can include chemotherapy, steroids, radiation therapy, intensive combined treatments (including bone marrow or stem cell transplants), and growth factors. CONCLUSION ALL is one of the commonest cancers of the childhood. It has good prognosis if diagnosed in the early stages of the disease. One should not ignore atypical lymphocytes which give us a clue and indication for bone marrow study. In this case the total leukocyte count was normal. This patient’s prognosis was good as the case was diagnosed in subleukemic phase and patient responded well with chemotherapy. REFERENCES 1. Inaba H, Greaves M, Mullighan CG. Acute lymphoblastic leukaemia. Lancet. 2013 June 1; 381(9881), 1943–55. 2. Greer, J. P., Arber, D. A., Glader, B., List, A. F., Means, R. T., Paraskevas, F., & Rodgers, G. M. Wintrobe's clinical hematology: Thirteenth edition (2013). 3. Longo D.L., Fauci A.S., Kasper D.L., Hauser S.L., Jameson J, Loscalzo J eds. Harrison's Principles of Internal Medicine, 18e. Pandey, et al 4. Belson M, Kingsley B, Holmes A. Risk Factors for Acute Leukemia in Children: A Review. Environ Health Perspect 2007; 115: 138-145. 5. Collier JAB. Oxford Handbook of Clinical. Specialties, Third Edition. Oxford;1991.p.810. 6. Seiter, K (5 February 2014). Sarkodee-Adoo, C; Talavera, F; Sacher, RA; Besa, EC, eds. "Acute Lymphoblastic Leukemia". Medscape Reference. WebMD. Retrieved 17 April 2014. Please cite this article as: Pandey V, Mahesh K, Indira. Early diagnosis of childhood Acute lymphoblastic leukemia. Perspectives in medical research 2017;5(1):83-85. Sources of Support: Nil,Conflict of interest:None declared. 85