Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
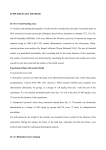
Chronic renal failure in a mouse model of human adenine phosphoribosyltransferase deficiency MICHAEL G. STOCKELMAN,1 JOHN N. LORENZ,2 FROST N. SMITH,3 GREGORY P. BOIVIN,3 AMRIK SAHOTA,4 JAY A. TISCHFIELD,4 AND PETER J. STAMBROOK1 Departments of 1Cell Biology, Neurobiology, and Anatomy, 2Molecular and Cellular Physiology, and 3Pathology and Laboratory Medicine, University of Cincinnati, College of Medicine, Cincinnati, Ohio 45267; and 4Department of Medical and Molecular Genetics, Indiana University School of Medicine, Indianapolis, Indiana 46202-5251 chronic kidney failure; purine metabolism; kidney calculi; allopurinol; sex factors enine (DHA) via an 8-hydroxyadenine intermediate (40). Adenine and DHA are excreted in the urine. However, the very low solubility of DHA can lead to its precipitation in the tubules of the kidney (8). APRT deficiency occurs in the human population as an autosomal recessive trait. The major clinical consequence associated with the defect is development of DHA nephrolithiasis, characterized by kidney stones, crystalluria, hematuria, dysuria, and urinary tract infections (29). The appearance of this condition is highly variable. APRT-deficient patients may develop severe renal problems in early childhood or may remain asymptomatic throughout life (28). Allopurinol, an XDH inhibitor (9), reduces DHA formation from adenine. Allopurinol treatment is effective in the control of DHA lithiasis in APRT-deficient patients (30). We have used gene targeting in embryonic stem cells to generate a mouse model of APRT deficiency. In our first report (12), we described the production of a germ-line mutation in Aprt via embryonic stem cells. We reported that mice homozygous for the targeted null mutation have disturbances of purine composition in the urine, including the excretion of macroscopic crystals of DHA, exhibit deposition of crystals in the kidney, and are prone to deterioration in health. In the present study, we investigated extent of renal lesion in the mice and functional consequences of renal pathology resulting from APRT deficiency. We found that, as in human cases of APRT deficiency, severity of symptoms varied widely among mice homozygous null for APRT. We report a sex difference in the severity of symptoms and show an amelioration of pathology in mice treated with allopurinol. METHODS phosphoribosyltransferase (APRT, EC 2.4.2.7) is a highly conserved (5) purine salvage enzyme that catalyzes the conversion of adenine and 5-phosphoribosyl-1-pyrophosphate to AMP. In mammals, APRT is present in all tissues and provides the only known mechanism for the metabolic salvage of adenine (29). Intracellular adenine is produced as a by-product of polyamine biosynthesis (38); dietary sources high in purines can also contribute significantly to adenine levels (17). Normally, adenine is efficiently salvaged by APRT and is present at very low levels in blood and urine (12, 29). In mammalian metabolism, when adenine is present in excess, it becomes a significant substrate for xanthine dehydrogenase (XDH, EC 1.2.3.2), which can oxidize adenine to 2,8-dihydroxyad- ADENINE F154 Mice. APRT-deficient mice were produced from an embryonic stem cell line carrying a targeted disruption of the Aprt locus in one allele (12). The colony used in these experiments was founded by a cross of 129/Sv chimeras with Black Swiss breeders, and later generations were bred by sibling matings. Mice were genotyped at age 2 wk from tail biopsies. To determine Aprt genotypes, genomic DNA isolated from collected tissue (21) was amplified in a three-primer PCR reaction, in which the 58 primer (58 CCACAACCTTCCCTCCTT 38) matched sequence within Aprt intron 2 and two alternative 38 primers matched a portion of the neo transgene insertion (58 GAGAACCTGCGTGCAATCCATCTTG 38) or the 38-untranslated region of Aprt (58 CCACCAAGCAGTTCCTAGTG 38). DNA from homozygous wild-type mice produced only a 700-bp PCR product from the two Aprt-specific primers. DNA from homozygous null mice produced only a 300-bp 0363-6127/98 $5.00 Copyright r 1998 the American Physiological Society Downloaded from http://ajprenal.physiology.org/ by 10.220.33.4 on June 18, 2017 Stockelman, Michael G., John N. Lorenz, Frost N. Smith, Gregory P. Boivin, Amrik Sahota, Jay A. Tischfield, and Peter J. Stambrook. Chronic renal failure in a mouse model of human adenine phosphoribosyltransferase deficiency. Am. J. Physiol. 275 (Renal Physiol. 44): F154– F163, 1998.—In humans, adenine phosphoribosyltransferase (APRT, EC 2.4.2.7) deficiency can manifest as nephrolithiasis, interstitial nephritis, and chronic renal failure. APRT catalyzes synthesis of AMP from adenine and 5-phosphoribosyl-1pyrophosphate. In the absence of APRT, 2,8-dihydroxyadenine (DHA) is produced from adenine by xanthine dehydrogenase (XDH) and can precipitate in the renal interstitium, resulting in kidney disease. Treatment with allopurinol controls formation of DHA stones by inhibiting XDH activity. Kidney disease in APRT-deficient mice resembles that seen in humans. By age 12 wk, APRT-deficient male mice are, on average, mildly anemic and smaller than normal males. They have extensive renal interstitial damage (assessed by image analysis) and elevated blood urea nitrogen (BUN), and their creatinine clearance rates, which measure excretion of infused creatinine as an estimate of glomerular filtration rate (GFR), are about half that of wild-type males. APRT-deficient males treated with allopurinol in the drinking water had normal BUN and less extensive visible renal damage, but creatinine clearance remained low. Throughout their lifespans, homozygous null female mice manifested significantly less renal damage than homozygous null males of the same age. APRT-deficient females showed no significant impairment of GFR at age 12 wk. Consequences of APRT deficiency in male mice are more pronounced than in females, possibly due to differences in rates of adenine or DHA synthesis or to sex-determined responses of the kidneys. RENAL FAILURE IN MICE WITH DEFECTIVE ADENINE SALVAGE Fig. 1. Simultaneous clearance of infused creatinine and FITCinulin in mice. Mice (n 5 7) were infused with both creatinine and FITC-inulin, and clearance of each was determined at four time points. Mice were untreated during the first two sampling periods and were treated with cimetidine during the first two sampling periods. A: inulin clearance and creatinine clearance. B: ratio of creatinine clearance (Ccr ) to inulin clearance (Ci ) at each data point. observed to decrease the secretion of creatinine (26), possibly improving its performance as a marker for GFR. Figure 1A shows average Ccr and Ci in the four periods (n 5 7). Figure 1B shows the ratio of Ccr to Ci in each period. These data demonstrate that, although Ccr does overestimate GFR somewhat (as expected), the relationship between Ccr and Ci is quite consistent and supports the validity of Ccr differences as an accurate reflection of differences in GFR. Mice in the third to fifth generation of sibling mating from 129/Sv crossed with Black Swiss founders were used in Ccr measurements. The mice were 12 wk of age, weighed 25–35 g, had not been bred previously, and were apparently in normal health. Mice were transported to the physiology laboratory 1 day prior to the procedure and kept overnight, with food and water ad libitum. On the following day, at ,3 h into the light cycle, mice were anesthetized with an injection of Inactin (thiobutabarbital, 100–150 µg/g ip) and, after 15 min, were placed ventral side up on a heated surgical table, fitted with a rectal thermometer to monitor and maintain body temperature, and surgically instrumented with a tracheotomy tube and catheters to the femoral artery, the femoral vein, and the urinary bladder. Blood losses from surgery were replaced with 100 µl of donor blood or 6% bovine serum albumin in saline immediately after the instrumentation was complete. After surgery, blood pressure and heart rate were monitored through the arterial line. At the same time, creatinine (5% in saline) was infused through the femoral vein. Mice were given Downloaded from http://ajprenal.physiology.org/ by 10.220.33.4 on June 18, 2017 PCR product from the 58 Aprt-specific primer and the 38 neo primer. DNA of heterozygous animals produced both PCR products. Mice received ad libitum water and Teklad LM-485 mouse/ rat sterilizable diet (Harlan-Teklad, Madison, WI) and were kept on a 14:10-h light-dark cycle in microisolator cages. In allopurinol experiments, ad libitum water contained 62 µg/ml allopurinol (Sigma Chemical, St. Louis, MO). The rate of water consumption by the mice was not affected by the presence of allopurinol. Water bottles were weighed at the time of filling, and the rate of water consumption per cage and the number of mice in each cage were used to estimate allopurinol dosage. Adult mice drank in the range of 10 ml water/day, resulting in a dose of ,25 mg · kg body wt21 · day21 for a typical 25-g mouse. Mating pairs were started on this regimen at weaning. Offspring raised from birth on allopurinol were examined for changes in kidney structure and function in comparison with normal and untreated APRTdeficient mice. Histology and measurement of renal pathology. All specimens were fixed in neutral-buffered Formalin and processed through a gradient of alcohols for paraffin embedding. Fourmicrometer sections, at intervals of 250 to 500 µm through the kidney, were stained with hematoxylin and eosin (20). Samples were viewed in bright-field or polarized light with an Olympus BH2 microscope (Olympus, New Hyde Park, NY). Kidneys were evaluated using general histological criteria for renal damage. Lesions were limited to tubular changes (tubular dilation, tubular degeneration, tubular necrosis, and loss of tubules) with secondary interstitial changes (fibrous tissue infiltration and lymphocyte and plasma cell infiltration). Images of kidney cross sections were captured, using a Sony video camera and video printer (Sony, Tokyo, Japan) and a Scion Frame Grabber (Scion, Frederick, MD), then imported to the public domain software NIH Image (developed at National Institutes of Health, Bethesda, MD; http:// rsb.info.nih.gov/nih-image) on a Macintosh Quadra computer (Apple Computers, Cupertino, CA). Lesioned areas in kidney sections were visually identified and outlined on screen, and their area in pixels were determined by NIH Image. Histological lesions quantified included areas of crystal deposition, inflammation, tubule loss with replacement fibrosis, tubule dilation, and tubule damage with regeneration of tubular epthelium. The total area of the kidney cross section in the image was outlined on the basis of its relative darkness in the image (density slicing), and its area in pixels was determined by NIH Image. Protocol for determination of creatinine clearance. Because of technical limitations at the time of these experiments prevented the use of inulin, the clearance of infused creatinine was used to estimate glomerular filtration rate (GFR). To minimize the effect of creatinine secretion on the measured clearance by saturating the secretion mechanism, we infused very large amounts of creatinine. To validate this approach, we later compared the clearance of creatinine (Ccr ) to the simultaneous clearance of fluorescein-labeled inulin (FITCinulin) (Ci ). (A microassay of FITC-inulin requiring 3 µl plasma had not yet been standardized in the laboratory for the experiments reported here but became available later.) The results of these comparison studies are shown in Fig. 1. Animals were prepared as described below, except that an infusion containing both creatinine and FITC-inulin was maintained. Inulin and creatinine were determined in parallel during four consecutive periods. The first two periods were control periods. During the second two periods, cimetidine was infused. Under some circumstances, cimetidine has been F155 F156 RENAL FAILURE IN MICE WITH DEFECTIVE ADENINE SALVAGE RESULTS Structural damage in the kidneys of APRT-deficient mice. The kidneys of APRT-deficient mice exhibit DHA deposition and consequent pathological changes (12). Figure 2 shows representative sections of kidney from wild-type and homozygous null mice, as well as from allopurinol-treated homozygous null males. A brightfield image from the kidney of a homozygous null male (Fig. 2A) illustrates the extensive renal interstitial pathology resulting from APRT deficiency, whereas the same field viewed in polarized light (Fig. 2B) reveals the deposition of crystals in the renal interstitium. APRT-positive animals have no apparent kidney damage (Fig. 2C) and no crystals visible in polarized light (not shown). Untreated homozygous null males were more severely affected than homozygous null females, based on the extent of renal tubular damage seen in kidney sections (see Tables 1 and 2; Fig. 2D). Because kidney damage is expected to progress over time in affected mice, the extent of renal lesions in histological samples from mice of various ages was determined. The incidence of kidney damage in homozygous null mice compared with normal animals of wild-type or heterozygous genotypes is shown in Table 1. As early as 4 wk of age, 50% of homozygous null male mice excreted crystals in their urine (data not shown) and had tubular damage with dilation, fibrosis, tubular necrosis, and lymphoplasmacytic infiltration. Of homozygous null males ages 12 wk or greater, 85% had renal tubular damage visible in histological preparations. Representative lesions are shown in Fig. 3. Lymphocyte infiltration (Fig. 3A) was associated with diffuse crystal deposition (Fig. 3B). Other lesions in the kidney included fibrosis (Fig. 3C), dilation of tubules (Fig. 3D), and atrophy and collapse of tubules (Fig. 3E). Homozygous null female mice had a much lower incidence of kidney pathology, a pattern that appeared to hold true throughout the animals’ lives. Crystals were also occasionally observed in other tissues, including muscle and testes, of homozygous null males ages 20–40 wk (Fig. 4), whereas similar deposits were not detected in mice with APRT activity. The extent of renal damage and crystal deposition observed in cross sections from kidneys of 12-wk-old animals is quantified in Table 2. Although there was no significant difference in the number of sites of crystal deposition observed in sections from null males and females, the extent of damage was considerably greater in sections examined from the APRT-deficient males than their female counterparts. No crystal deposition or other pathology were observed in kidney sections from wild-type or heterozygous animals. Renal histopathology of allopurinol-treated homozygous null males. Microscopic analysis of the kidneys of 12-wk-old allopurinol-treated, APRT-deficient males suggested that allopurinol decreased the severity of kidney pathology compared with untreated null males. Tubule pathology was observed in four of five kidney sections from treated null males that were examined (Table 1; Fig. 2E). However, the area of involvement in those sections was significantly less than that observed in comparable sections from untreated APRT-deficient males (Table 2). Similarly, the formation of crystals was reduced in allopurinol-treated null males. Crystals were observed in a lower proportion of sections from allopurinol-treated homozygous null males (2 of 5) than sections from untreated homozygous null males (6 of 7), and the number of sites of crystal deposit per section examined was significantly lower (Table 2). Because consequences of APRT deficiency were mild in un- Downloaded from http://ajprenal.physiology.org/ by 10.220.33.4 on June 18, 2017 a priming dose of 1.3 µl/g body wt, then continuously infused throughout the procedure at a rate of 0.1 µl·g body wt21 ·min21, using a model 200 pump from KD Scientific (Boston, MA) and a 1-ml syringe (Becton-Dickinson, Franklin Lakes, NJ). Ccr was measured in four 30-min sampling periods beginning 30 min after surgery. The first two sampling periods established the baseline for the animal, followed by treatment (volume expansion) and two periods of experimental measurement. Volume expansion consisted of increasing the maintenance infusion from 0.1 to 1.0 µl · g body wt21 · min21, with the appropriate decrease in creatinine concentration to keep the rate of creatinine infusion constant. A 30-min stabilization time was allowed following the switch to the volume challenge, during which the urine flow rate typically increased markedly. During each sampling period, urine was quantitatively collected, and, at the midpoint of the sampling period, a blood sample of 60 µl was collected into an NH4heparin hematocrit capillary (Fisher Scientific, Pittsburgh, PA) from the arterial line. Blood volume was restored after each sampling by infusion of donor mouse blood. The volume of the urine sample was determined by weight, and the urine was stored at 4°C in a polyethylene microcentrifuge tube. Blood was fractionated in a hematocrit centrifuge for determining the blood cell fraction, then the plasma was collected into a polyethylene microcentrifuge tube. Urine and plasma samples were overlaid with mineral oil and assayed within a week for creatinine. After two baseline measurements and two volume expansion measurements were obtained, the experiment was terminated by infusion of concentrated potassium chloride. The kidneys were removed, individually weighed, and fixed in 10% neutral-buffered Formalin. Biochemical determinations. Urine and plasma samples were assayed for creatinine, using a spectrophotometric assay modified from Folin and Wu (13). For the assay, urine was diluted 1:50 in water. Three microliters plasma or diluted urine and 300 µl picric acid reagent (consisting of saturated aqueous picric acid diluted 5-fold in 0.25 M NaOH) were dispensed in duplicate, using a MicroLab dilutor (Hamilton, Reno, NV) into wells of a microtiter plate. After incubation for 15 min at room temperature, absorbance was read at 515 nm in a microplate reader. Ccr in milliliters of plasma per minute was calculated by Ccr 5 (Cu/Cp ) 3 V, where Cu is the concentration of creatinine in urine, Cp is the concentration of creatinine in plasma at the midpoint of urine collection, and V is the urine flow rate in milliliters per minute. Measurement of blood urea nitrogen (BUN) was used as an alternative assay of kidney function. This assay measures plasma levels of the nitrogenous waste product urea, which accumulates in blood with the development of kidney failure. Blood samples for BUN determination were collected in sodium heparin capillaries from the orbital sinus. BUN values were measured spectrophotometrically in an enzymebased assay (Sigma Chemical). Statistics. Because of the differences in standard deviations among the groups for some variables, statistical results were evaluated by analysis of variance. F157 RENAL FAILURE IN MICE WITH DEFECTIVE ADENINE SALVAGE treated APRT-deficient females, the effects of allopurinol treatment on APRT-deficient females were not studied. Creatinine clearance rates and kidney function in APRT-deficient mice. By 12 wk of age, homozygous null male mice but not female mice differed significantly from normal counterparts. As shown in Table 3, APRTdeficient male mice had smaller average body sizes and kidney weights than normal males and had lower hematocrits. Body weights, kidney weights, and hematocrits of allopurinol-treated, APRT-deficient males were intermediate between those of normal males and untreated homozygous null males, although the differences from either group were not statistically significant. Ccr in 12-wk-old homozygous null males was significantly lower than Ccr rates in control animals Table 1. Occurrence of histologically observable lesions in kidneys of APRT-deficient mice at various ages Fraction of Mice With Lesions Group Male, 2/2 Male, 1/1, 1/2 Allopurinol male, 2/2 Female, 2/2 Female, 1/1, 1/2 Age, wk n Dilation Degeneration Regeneration Fibrosis Inflammation Any Lesion 12 15–20 30–40 12 15–20 30–40 12 12 15–20 30–40 12 15–20 30–40 10 9 7 7 5 5 5 11 10 6 10 6 6 0.70 0.78 0.86 0 0 0 0.40 0.45 0.30 0.33 0 0 0.17 0.70 0.89 0.86 0 0 0 0.60 0.64 0.70 0.17 0 0 0 0.50 0.78 0.86 0 0 0 0.40 0.18 0.20 0.17 0 0 0 0.60 0.89 0.86 0 0 0 0.60 0.64 0.70 0.17 0 0 0 0.50 0.89 0.86 0 0 0 0.60 0.64 0.40 0.33 0 0 0 0.80 0.89 0.86 0 0 0 0.80 0.64 0.70 0.50 0 0 0.17 Three longitudinal sections from left kidney and three cross sections from right kidney of each mouse (at intervals of 250 µm) were examined for the lesions indicated. Results are the fraction of mice with observable lesions in any section. APRT, adenine phosphoribosyltransferase. Downloaded from http://ajprenal.physiology.org/ by 10.220.33.4 on June 18, 2017 Fig. 2. Hematoxylin and eosin stain of renal cortex from adenine phosphoribosyltransferase (APRT)-deficient and normal mice. A: APRT-deficient male mouse, age 10 wk. Fibrosis, inflammation, and tubular dilation are evident in bright-field view. B: same field of view as A; illumination with polarized light emphasizes deposition of crystals in tubules and interstitium. C: wild-type male mouse, age 13 wk. No lesions are visible. D: APRT-deficient female mouse, age 14 wk. Single interstitial crystal is seen (arrow). E: APRT-deficient male mouse, age 12 wk, treated with allopurinol. * Large dilated tubule containing several crystals. Magnification, 350. F158 RENAL FAILURE IN MICE WITH DEFECTIVE ADENINE SALVAGE Table 2. Morphometric analysis of lesions in the kidneys of 12-wk-old transgenic mice Group Area of Involvement n Crystal Sites/ Kidney Section n Male, 2/2 Male, 1/1 Allopurinol male, 2/2 Female, 2/2 Female, 1/1 18.8 6 7.9 0 4.4 6 2.7 1.6 6 0.5* 0 7 6 5 6 9 7.7 6 2.7 0 261 9.8 6 5.3 0 6 5 2 4 4 (51% of values in wild-type males), and continuous treatment with allopurinol resulted in only marginally improved Ccr in homozygous null males, as shown in Fig. 5. The kidneys’ capacity to regulate urine output was tested by increasing the flow of creatinine infusion. This volume expansion did not significantly alter Ccr in Fig. 3. Pathology of 2,8-dihydroxyadenine (DHA) nephropathy in APRT-deficient mice. A: lymphocytic infiltration into renal interstitium, in association with diffuse crystal deposition; 10-wk-old null male; magnification, 3200. B: same field as in A, viewed in polarized light. C: fibrosis of renal parenchyma; 10-wk-old null male; magnification, 3200. D: dilation of tubules and formation of casts in tubular lumina; 12-wk-old null male; magnification, 3100. E: condensation of renal cortex. Loss of tubules leads to high density of glomeruli in affected region; 20-wk-old null male; magnification, 3100. Downloaded from http://ajprenal.physiology.org/ by 10.220.33.4 on June 18, 2017 Values are means 6 SE. Digital micrographs of cross sections of kidneys (3 sections/mouse at 250-µm intervals) were analyzed. Lesions including tubular dilation, fibrosis, necrosis, and regeneration were traced by hand. Results are lesion area as percent of total cross-sectional area, as calculated using NIH Image software. Number of sites of crystal deposition visible in polarized light were counted. Some samples from APRT-deficient mice had no crystals visible. Only sections with crystals were measured here. * Three other samples examined from homozygous null females had no lesions in the sections observed. Only sections with lesions were measured here. any group (Fig. 5). We did not specifically measure urine concentrating ability, but observations from the volume expansion suggested that homozygous null males may have a poor capacity to conserve water. When mice were receiving the high-volume infusion, the urine flow rates were not significantly different (14.9 6 6.2 µl/min in homozygous null males vs. 13.0 6 8.6 µl/min in wild-type males), but when receiving the low rate of infusion, the homozygous null males had a significantly higher flow rate (7.5 6 1.9 µl/min vs. 3.6 6 2.2 µl/min in wild-type males). Homozygous null males also tended to have higher rates of urine excretion and water consumption rates, which is consistent with the hypothesis that the affected mice have impaired ability to concentrate urine. BUN levels in normal, homozygous null, and allopurinol-treated homozygous null animals are shown in Fig. 6. Consistent with histology and Ccr data, the only group that was significantly affected was the homozygous null males, in which BUN levels, although highly variable, were two to three times higher than in normal animals of the same age. In older homozygous null males, ages 30–50 wk, there is an apparent improvement in BUN values, compared with homozygous null males ages 10–20 wk. This may be due to early death of RENAL FAILURE IN MICE WITH DEFECTIVE ADENINE SALVAGE F159 severely affected mice and greater survival to advanced age of mildly affected individuals, with few severely affected mice surviving as long as 30 wk. The data are consistent with this hypothesis. In the younger homozygous null male group, 50% of the mice examined had BUN values .100 mg/dl, whereas, in the older homozygous null male group, one individual, which had severely damaged kidneys and was sick at the time of sample collection, had a BUN of 265 mg/dl, whereas the remaining samples all had values of 65 mg/dl or less. Table 3. Characteristics of 12-wk-old mice used in measurement of creatinine clearance Group Male, 1/1 Male, 1/2 Male, 2/2 Allopurinol male, 2/2 Female, 1/1 Female, 1/2 Female, 2/2 n Body Wt, g Kidney Wt, mg Relative Kidney Wt, % body wt Hematocrit 5 30.4 6 7.37 428.8 6 82.6 1.4 6 0.06 46.4 6 2.3 7 31.6 6 3.61 511.7 6 62.4 1.6 6 0.08 49.0 6 3.6 7 24.9 6 1.77† 306.5 6 49.4* 1.2 6 0.06* 40.4 6 3.9* 4 5 7 6 26.3 6 2.87 25.0 6 1.41 23.4 6 1.40 23.3 6 4.37 346.5 6 33.9† 409.0 6 24.3 382.3 6 35.0 327.9 6 89.0 1.3 6 0.04† 1.6 6 0.06 1.6 6 0.07 1.4 6 0.08 41.5 6 5.7† 47.8 6 3.0 49.9 6 3.6 48.3 6 1.9 Values are means 6 SE. * P , 0.05 by ANOVA: statistically significant difference vs. male 1/1, 1/2; † statistically significant difference vs. male 1/2. Fig. 5. Creatinine clearance in APRT-deficient and normal mice. Creatinine clearance was measured in anesthetized, surgically instrumented 12-wk-old mice (see Table 3) receiving infused creatinine (5% creatinine in saline, 0.1 µl · g body wt21 · min21 ). Untreated males and females of all genotypes were tested, as were homozygous null males that had been raised on drinking water containing 62 µg/ml allopurinol (M 2/2, allopurinol). Solid bars, female groups according to genotype; open bars, male groups according to genotype and treatment. Hatched bars, results from volume expansion experiments on each group. Sample sizes are indicated in Table 3. Results are means 6 SE, expressed in ml plasma cleared · min21 · g body wt21. * P , 0.05, statistically significant difference vs. heterozygous or wild-type males. Downloaded from http://ajprenal.physiology.org/ by 10.220.33.4 on June 18, 2017 Fig. 4. Crystal deposits in nonrenal tissue of APRT-deficient mice. Examination under polarized light of tissues from APRT-deficient mice occasionally revealed isolated crystals (identified by arrows) resembling urinary crystals previously identified as DHA (12). A and B: skeletal muscle (magnification, 3400). C and D: testis (magnification, 3200). Sections from a 20-wk-old homozygous null male, viewed under polarized (A and C) and bright-field (B and D) optics. F160 RENAL FAILURE IN MICE WITH DEFECTIVE ADENINE SALVAGE Allopurinol-treated null males did not have elevated BUN levels compared with normal males at 12 wk. Allopurinol treatment apparently helped preserve kidney function in this respect. This is consistent with the significant decrease in renal histological lesions seen in allopurinol-treated homozygous null males compared with untreated null males. DISCUSSION In this and a previous report (12), we describe some phenotypic characteristics of transgenic mice that lack functional APRT. The absence of APRT activity in mice homozygous for an Aprt null allele results in a phenotype much like that seen in APRT-deficient humans (29). Specifically, the mice have high levels of urinary adenine and adenine metabolites, including DHA, and they develop pathological changes in the kidney following the formation of stones in the lumina of renal tubules and in the renal interstitium (12). The current study was intended to establish the extent of renal pathology and some of the functional consequences of kidney damage suffered by the APRTdeficient mice. Creatinine clearance in wild-type, heterozygous, and homozygous null mice was measured and related to the extent of kidney damage in normal and mutant mice. The efficacy of allopurinol in controlling the renal pathology associated with APRT deficiency was evaluated. The ability of a simple noninvasive assay (BUN determination) to measure kidney function in this system was also assessed. Mice were markedly affected by APRT deficiency. The consequences of APRT deficiency manifested as kidney lesions typical of chronic interstitial nephritis (7) and were apparent in homozygous null mice at all ages examined (Table 1 and Figs. 2 and 3). Female APRTdeficient mice were much less severely affected than Downloaded from http://ajprenal.physiology.org/ by 10.220.33.4 on June 18, 2017 Fig. 6. Blood urea nitrogen (BUN) in APRT-deficient and normal mice. BUN was measured in plasma samples from mice at ages 10–20 and 30–50 wk. Hatched bars, normal males (Aprt 1/1 and 1/2). Latticed bars, homozygous null males. Light shaded bars, allopurinol-treated null males. Darkly shaded bars, normal females (Aprt 1/1 and 1/2). Solid bars, homozygous null females. Open bars, allopurinol-treated null females. Results are means of BUN (mg/dl) 6 SE; sample sizes indicated at bottom. * P , 0.05, statistically significant difference compared with other groups by ANOVA. males. Consistent with the kidney histopathology was physiological impairment of renal function. Twelveweek-old homozygous null males had an average GFR about half that of normal animals (Fig. 5). At 12 wk of age, the homozygous null males suffered moderate chronic renal failure (1), manifesting as low GFR, depressed hematocrit, azotemia (indicated by elevated BUN values, Fig. 6), and possible reduced urine concentrating ability. The severity of the phenotype in homozygous null males was highly variable, with creatinine clearance values ranging from 10 to 90% of normal. Homozygous null females may also have had a slight trend toward lower creatinine clearance, compared with heterozygous and wild-type females, although this difference was not statistically significant. The results from BUN measurement were similar to the creatinine clearance results (Figs. 5 and 6). Compared with creatinine clearance, however, BUN has the advantage of being relatively noninvasive; animals may be sampled regularly without impairing health. Thus this assay will allow sequential determinations of the progression of renal disease as a function of time in this model system and may prove especially useful for genetic mapping of modifier loci, which determine the severity of renal pathology in APRT-deficient mice. A striking observation is the sex difference in the severity of kidney damage and dysfunction in homozygous null mice (Tables 1 and 2 and Fig. 5). Homozygous null female mice had comparatively mild symptoms of tubule pathology. Their GFRs were not significantly lower than normal. Histologically, less than 2% of kidney cross-sectional area was affected in 12-wk-old females, and, even at 30–40 wk, only three of six animals had notable kidney damage in sections examined. In contrast, homozygous null male mice developed more severe renal lesions at a much earlier age. At 12 wk of age, null males had a significant reduction in GFR, and 80% of kidneys examined had visible lesions, affecting on average 18.8% of kidney cross-sectional area. The sex-related differences in the severity of the phenotype may simply reflect an increased susceptibility of males to a range of renal pathology, a pattern seen both in humans and in many model systems. This issue is reviewed extensively by Silbiger and Neugarten (27). They suggest that intrinsic sex-based differences in kidney structure and function, as well as blood pressure or hormonal environment, may account for the higher frequency and greater severity of kidney dysfunctions seen in males. Similarly, renal stone disease in humans occurs in males at four times the frequency seen in females (summarized in Ref. 34). However, this observation cannot be generalized to all types of renal stone disease. For example, 75% of calcium oxalate stones, which account for 50–80% of all cases of nephrolithiasis, occur in males. In contrast, two-thirds of magnesium ammonium phosphate stones are in females (15, 34), whereas uric acid stones are equally distributed among females and males (34). The factors determining sex-based differences in susceptibility to kidney stones are probably individual to each stone RENAL FAILURE IN MICE WITH DEFECTIVE ADENINE SALVAGE Allopurinol treatment appeared to provide partial protection from the nephrotoxic consequences of APRT deficiency. Allopurinol, an inhibitor of XDH (11), was added to drinking water at 62 µg/ml H2O to inhibit production of DHA, with the intent of lessening the severity of renal disease in APRT-deficient mice. Based on water consumption, the mice received ,25 mg · kg body wt21 · day21; the presence of allopurinol in the drinking water did not appear to inhibit water consumption by the mice. Allopurinol is used routinely to control DHA nephrotoxicity in APRT-deficient patients (28), as well as to manage gout and hyperuricemia in humans with excessive production of uric acid (14). Allopurinol has also been shown to inhibit XDH activity in mice. Early studies in mice found that single oral doses of 12.5–25 mg/kg body wt effectively suppressed the catabolism of oxypurines by XDH (10). Continuous administration of allopurinol in drinking water has been shown to be effective in controlling hyperuricemia and urate nephropathy in uricase-deficient mice (39). Effective doses, in terms of increased survival of neonates and decrease in serum uric acid, ranged from 45 to 150 µg/ml. In the present study, 12-wk-old male mice treated with a similar dose of allopurinol exhibited a significant decrease in lesioned area in the kidney (4.4% of cross-sectional area vs. 18.8% in untreated homozygous null male mice; see Table 2) and an apparent decrease in the number of sites of crystal deposition in the kidneys of treated animals. However, the majority of the sections examined contained at least one lesion. The lesions included tubule dilation, fibrosis, and one group of large crystals (Fig. 2E). The allopurinol-treated males had GFR values that were intermediate between those of wild-type and homozygous null males (Fig. 5) and had normal BUN values (Fig. 6). Because visible lesions were not completely prevented and creatinine clearance may be impaired in allopurinol-treated APRT-deficient male mice, it may be that XDH activity was not sufficiently inhibited at the administered allopurinol dose to prevent formation of DHA. Alternatively, allopurinol may have had beneficial effects in control of DHA nephrotoxicity, as reflected in normal BUN values and less extensive structural damage and crystal deposition, while exerting its own deleterious effect on creatinine clearance. In normal rats, allopurinol treatment (400 µg/ml H2O) for 15 wk resulted in minor kidney lesions and a 30% lower GFR compared with untreated rats (33). However, 400 µg allopurinol/ml H2O in drinking water is probably a toxic dose. In our own observations (unpublished), mice continuously receiving 310 µg/ml H2O allopurinol in drinking water sometimes developed bladder stones composed of xanthine and oxipurinol (a poorly soluble metabolite of allopurinol). Another study (36) gave daily subcutaneous injections of allopurinol at ,12.5– 100 mg/kg body wt to healthy male rats; at 25 mg · kg21 · day21, 74–100% of animals had slight kidney lesions after 10 days. The mechanism for allopurinolinduced nephrotoxicity is not known. There is evidence to suggest that oxidative damage may be involved, a Downloaded from http://ajprenal.physiology.org/ by 10.220.33.4 on June 18, 2017 type. APRT deficiency in humans can result in severe pathology in both males and females. Sixty percent of symptomatic APRT-deficient humans are males; however, the significance of this observation has not been statistically validated. In the case of APRT deficiency, the more serious pathology observed in males may be a result of males producing more DHA than females. The kidney has a threshold tolerance to DHA. In adenine toxicity studies, intravenous administration of adenine at doses of ,10 mg/kg resulted in elevation of excreted adenine and adenine metabolites, including DHA and 8-hydroxyadenine. Doses that exceeded the capacity to metabolize or excrete the administered adenine resulted in the deposition of progressively more DHA, first in the distal tubules and then the proximal tubules and the kidney interstitium. Very high doses led to acute renal failure and death. After subacute doses, subjects recovered with minimal permanent damage (3, 4, 6, 23). It is possible that more adenine is generated in males than in females. In mammals, the major source of free adenine is polyamine biosynthesis, of which adenine is a by-product (29). The 58-methylthioadenosine that is generated in the synthesis of the polyamines spermidine and spermine is rapidly cleaved to produce molar equivalents of adenine and 5-methylthioribose. There is a suggestion that males produce more polyamines in both their urogenital tissues and some other organs. In the male, the prostate gland produces a high level of polyamines (32, 37). The kidney of the male mouse also contains higher levels of polyamines than that of the female; this difference is testosterone dependent (16). The liver, on the other hand, is a major polyamineproducing organ, which, in the rat, shows no sex differences (24, 25). If male mice produce more polyamines and consequently more adenine, this could predispose male APRT-deficient mice to more severe renal disease. Because DHA is produced by the oxidation of adenine by XDH, higher XDH activities in males would also predispose them to disease. Although there is evidence that XDH activity, found at high levels in the liver (35) and in the small intestine in mice (22), may be higher in males than in females, studies of XDH activity in mice have produced contradictory findings. In one case, XDH was 25% higher in the livers of males and 12.5% higher in male small intestine (22). Another study (19) showed no significant difference between males and females. The variations in reported XDH activity in mice may be due to differences in genetic background (18). This might also account for the variations in the severity of symptoms that we see in our mice, since they are of mixed genetic background (129/Sv and Black Swiss). If males do have higher XDH activity than females, a higher proportion of adenine would be converted to DHA, resulting in more extensive deposition and a greater burden on the kidney. As noted, in humans, 60% of reported clinical cases of symptomatic APRT deficiency occur in males (29). It is not clear whether similar mechanisms account for the sex difference in mice and humans. F161 F162 RENAL FAILURE IN MICE WITH DEFECTIVE ADENINE SALVAGE We thank David Hellard of the Molecular Physiology Core Facility at the University of Cincinnati for expert technical assistance. This work was supported by National Institute of Diabetes and Digestive and Kidney Diseases Grant DK-38185 and by National Institute of Environmental Health Sciences Grants ES-05652 and ES-06096. Address for reprint requests: P. J. Stambrook, Dept. of Cell Biology, Neurobiology, and Anatomy, Univ. of Cincinnati College of Medicine, Cincinnati, OH 45267-0521. Received 25 August 1997; accepted in final form 27 February 1998. REFERENCES 1. Abuelo, J. G. Renal Pathophysiology: The Essentials (1st ed.). Baltimore, MD: Williams and Wilkins, 1989, p. 322. 2. Ansari, N. H., and S. Rajaraman. Allopurinol-induced nephrotoxicity: protection by the antioxidant, butylated hydroxytoluene. Res. Commun. Chem. Pathol. Pharmacol. 75: 221–229, 1992. 3. Bartlett, G. R. Metabolism by man of intravenously administered adenine. Transfusion 17: 367–373, 1977. 4. Bartlett, G. R. Metabolism by the rabbit of intravenously administered adenine. Transfusion 17: 351–357, 1977. 5. Broderick, T. P., D. A. Schaff, A. M. Bertino, M. K. Dush, J. A. Tischfield, and P. J. Stambrook. Comparative anatomy of the human APRT gene and enzyme: nucleotide sequence divergence and conservation of a nonrandom CpG dinucleotide arrangement. Proc. Natl. Acad. Sci. USA 84: 3349–3353, 1987. 6. Cameron, J. S., H. A. Simmonds, A. Cadenhead, and D. Farebrother. Metabolism of intravenous adenine in the pig. Adv. Exp. Med. Biol. 76A: 196–205, 1977. 7. Cotran, R. S., V. Kumar, and S. L. Robbins. Robbins’ Pathological Basis of Disease. Philadelphia, PA: Saunders, 1989. 8. De Vries, A., and O. Sperling. Implications of disorders of purine metabolism for the kidney and the urinary tract. Ciba Found. Symp. 48: 179–206, 1977. 9. Elion, G. B. Enzymatic and metabolic studies with allopurinol. Ann. Rheum. Dis. 25: 608–614, 1966. 10. Elion, G. B., F. M. Benezra, I. Canellas, L. O. Carrington, and G. H. Hitchings. Effects of xanthine oxidase inhibitors on purine catabolism. Israel J. Chem. 6: 787–796, 1968. 11. Elion, G. B., A. Kovensky, and G. H. Hitchings. Metabolic studies of allopurinol, an inhibitor of xanthine oxidase. Biochem. Pharmacol. 15: 863–880, 1966. 12. Engle, S. J., M. G. Stockelman, J. Chen, G. Boivin, M.-N. Yum, P. M. Davies, M. Y. Ying, A. Sahota, H. A. Simmonds, P. J. Stambrook, and J. A. Tischfield. Adenine phosphoribosyltransferase-deficient mice develop 2,8-dihydroxyadenine nephrolithiasis. Proc. Natl. Acad. Sci. USA 93: 5307–5312, 1996. 13. Folin, O., and H. Wu. A system of blood analysis. J. Biol. Chem. 38: 81–110, 1919. 14. Frayha, R. A. Allopurinol. A review. Lebanese Med. J. 24: 463–71, 1971. 15. Gault, M. H., L. Chafe, P. Parfrey, and W. G. Robertson. The kidney-ureter stone sexual paradox: a possible explanation. J. Urol. 141: 1104–1106, 1989. 16. Goldstone, A., H. Koenig, and C. Lu. Testosterone-dependent sexual dimorphism of the mouse kidney is mediated by polyamines. Biochem. Biophys. Res. Commun. 104: 165–172, 1982. 17. Greenwood, M. C., M. J. Dillon, H. A. Simmonds, T. M. Barratt, J. R. Pincott, and C. Metreweli. Renal failure due to 2,8-dihydroxyadenine urolithiasis. Eur. J. Pediatr. 138: 346–349, 1982. 18. Henderson, J. F., G. Zombor, M. M. Johnson, and C. M. Smith. Variation in erythrocyte purine metabolism among mouse strains. Comp. Biochem. Physiol. B Biochem. Mol. Biol. 76: 419–422, 1983. 19. Huh, K., I. Yamamoto, E. Gohda, and H. Iwata. Tissue distribution and characteristics of xanthine oxidase and allopurinol oxidizing enzyme. Jpn. J. Pharmacol. 26: 719–724, 1976. 20. Humason, G. L. Animal Tissue Techniques. San Francisco, CA: Freeman, 1979. 21. Laird, P. W., A. Zijderveld, K. Linders, M. A. Rudnicki, R. Jaenisch, and A. Berns. Simplified mammalian DNA isolation procedure (Abstract). Nucleic Acids Res. 19: 4293, 1991. 22. Lee, P. C. Developmental changes of adenosine deaminase, xanthine oxidase, and uricase in mouse tissues. Dev. Biol. 31: 227–233, 1973. 23. Lindblad, G., G. Jonsson, and J. Falk. Adenine toxicity: a three week intravenous study in dogs. Acta Pharmacol. Toxicol. 32: 246–256, 1973. 24. McAnulty, P. A., and J. P. Williams. Polyamines and their biosynthetic decarboxylases in various tissues of the young rat during recovery from undernutrition. Biochem. J. 162: 109–121, 1977. 25. Neish, W. J., and L. Key. Polyamines and glutathione in livers of normal rats of different ages and in livers of pregnant rats. Biochem. Pharmacol. 17: 497–502, 1968. 26. Olsen, N. V., S. D. Ladefoged, B. Feldt-Rasmussen, N. Fogh-Andersen, H. Jordening, and O. Munck. The effects of cimetidine on creatinine excretion, glomerular filtration rate and tubular function in renal transplant recipients. Scand. J. Clin. Lab. Invest. 49: 155–159, 1989. 27. Silbiger, S. R., and J. Neugarten. The impact of gender on the progression of chronic renal disease. Am. J. Kidney Dis. 25: 515–533, 1995. Downloaded from http://ajprenal.physiology.org/ by 10.220.33.4 on June 18, 2017 surprising conclusion, since XDH is a source of reactive oxygen species, and the inhibition of XDH activity might be predicted to have antioxidant effects. Nonetheless, butylated hydroxytoluene, an antioxidant, has been shown to protect from allopurinol toxicity (2). Furthermore, allopurinol treatment increases renal xanthine oxidase activity and decreases renal activity of superoxide dismutase and catalase in rats (31), thereby increasing an activity that generates reactive oxygen species and decreasing an activity which eliminates them. The present data show that APRT-deficient mice can develop chronic renal failure in association with nephrolithiasis and that this pathology is reflected in lower GFR. As a murine model that closely mimics the known features of human APRT deficiency, this system provides an opportunity to address questions of clinical interest, such as the biochemical consequences of APRT deficiency in multiple tissues not available from human subjects and the role of genetic modifier loci in the development of the APRT-deficient phenotype. In mice, the consequences of APRT deficiency on enzymes and substrates of nucleotide metabolism may be studied in specific tissues and organs, such as the brain and bone marrow, which may be particularly dependent on purine salvage reactions for nucleotides (35). The genetics of APRT deficiency also may be more fully studied in mice than in humans. APRT-deficient humans manifest considerable differences in the age of onset and the severity of disease. Although diet and environment may contribute to this variability, it is likely that genetic factors in addition to Aprt also modulate the progression of the disease. Initial results with APRTdeficient mice indicated that mice of C57Bl/6 background were affected earlier and more severely by APRT deficiency than mice of Black Swiss derivation (12). Appropriate breeding of APRT deficiency into different murine genetic backgrounds will provide a valuable tool for the characterization of loci, whose alleles modify the severity of renal disease in APRT deficiency. RENAL FAILURE IN MICE WITH DEFECTIVE ADENINE SALVAGE 35. 36. 37. 38. 39. 40. Prevention and Treatment, edited by C. Y. C. Pak. Boston, MA: Martinus Nijhoff, 1987, p. 85–120. Watts, R. W. Molecular variation in relation to purine metabolism. J. Clin. Pathol., Suppl. 8: 48–63, 1974. Wexler, B. C., and B. P. Greenberg. Allopurinol-induced myocardial and renal damage in nonarteriosclerotic (virgin) and arteriosclerotic (breeder) Sprague-Dawley rats. Proc. Soc. Exp. Biol. Med. 157: 541–549, 1978. Williams-Ashman, H. G., A. E. Pegg, and D. H. Lockwood. Mechanisms and regulation of polyamine and putrescine biosynthesis in male genital glands and other tissues of mammals. Adv. Enzyme Regul. 7: 291–323, 1969. Williams-Ashman, H. G., J. Seidenfeld, and P. Galletti. Trends in the biochemical pharmacology of 58-deoxy-58-methylthioadenosine. Biochem. Pharmacol. 31: 277–288, 1982. Wu, X., M. Wakamiya, S. Vaishnav, R. Geske, C. Montgomery, Jr., P. Jones, A. Bradley, and C. T. Caskey. Hyperuricemia and urate nephropathy in urate oxidase-deficient mice. Proc. Natl. Acad. Sci. USA 91: 742–746, 1994. Wyngaarden, J. B., and J. T. Dunn. 8-hydroxyadenine as the metabolic intermediate in the oxidation of adenine to 2,8dihydroxyadenine by xanthine oxidase. Arch. Biochem. Biophys. 70: 150–6, 1957. Downloaded from http://ajprenal.physiology.org/ by 10.220.33.4 on June 18, 2017 28. Simmonds, H. A. 2,8-Dihydroxyadenine lithiasis. Clin. Chim. Acta 160: 103–108, 1986. 29. Simmonds, H. A., A. Sahota, and K. J. Van Acker. APRT deficiency: 2,8-dihydroxyadenine lithiasis. In: The Metabolic and Molecular Bases of Inherited Disease (7th ed.), edited by J. B. Stanbury, J. B. Wyngaarden, and D. G. Fredrickson. New York: McGraw-Hill, 1995. 30. Simmonds, H. A., K. J. Van Acker, J. S. Cameron, and A. McBurney. Purine excretion in complete adenine phosphoribosyltransferase deficiency: effect of diet and allopurinol therapy. Adv. Exp. Med. Biol. 76B: 304–311, 1977. 31. Suzuki, Y., and J. Sudo. Possible mechanism responsible for allopurinol-nephrotoxicity: lipid peroxidation and systems of producing- and scavenging oxygen radicals. Jpn. J. Pharmacol. 45: 271–279, 1987. 32. Tabor, H., and C. W. Tabor. Biosynthesis and metabolism of 1,4-diaminobutane, spermidine, spermine, and related amines. Adv. Enzymol. Relat. Areas Mol. Biol. 36: 203–268, 1972. 33. Trachtman, H., E. Valderrama, and S. Futterweit. Nephrotoxicity of allopurinol is enhanced in experimental hypertension. Hypertension 17: 194–202, 1991. 34. Wainer, L., V. A. Resnick, and M. I. Resnick. Nutritional aspects of stone disease. In: Renal Stone Disease: Pathogenesis, F163