Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
CANCER I N JAVA AND SUMATRA
C. BONNE
Batavia, Java, Netherland East Indies
The Netherlands East Indies, which forms the largest part of the
Malay Archipelago, has above 60,000,000 inhabitants ; 40,000,000 live in
Java, one of the most densely populated parts of the world, and the
others are spread out over Sumatra, Borneo, Celebes New Guinea, and
thousands of smaller islands. Nearly the whole population belongs t o
the Malay race, but the presence of a few million Chinese makes it
possible to compare the pathology of these two Eastern races.
It is not easy to collect reliable information about the incidence of
disease in tropical countries, where statistical reports, methods of
registration of deaths and births, and a medical organization on the
scale to which we are accustomed in Western countries are lacking.
Rumors or vague impressions are of no use, especially in studying
cancer. I n our own experience in the East, and the experience of
others elsewhere in the tropics, views of the past on the relative importance of different diseases have proved entirely incorrect. We
were formerly so impressed by the often dramatic outbreaks of smallpox, cholera, malaria, beri-beri, plague, etc., that these were considered
to be not only the characteristic feature but practically the only manif estation of tropical pathology. Gradually, however, with the introduction of Western methods of prevention, these epidemic diseases
have lost most of their importance in the better developed tropical
communities. I n Java, for example, and in certain parts of Sumatra,
tropical disease as we usually understand it, though still playing a
certain rhle, is no longer all-important. Small-pox and cholera have
disappeared entirely ; ankylostomiasis, though widespread, is only
locally important as a disease ; beri-beri has become rare among adults,
and although plague has a foothold in certain mountainous parts of
Java, it does not occur very frequently. Malaria and dysentery may
still occur, occasionally and locally, in the old-fashioned way. This
tropical pathology is grafted on a larger body of disease which on first
impression seems similar t o disease as we know it in colder climates.
We find the same problems of tuberculosis, cancer, rheumatic fever,
cirrhosis of the liver, cardiac and renal diseases, as elsewhere. More
accurate research, however, reveals certain differences, and of these
differences one or two bear upon cancer.
Snijders and Straub (1)pointed out in 1921 that cancer in general
was found to be about as prevalent among the registered Javanese and
Chinese laborers in the large tobacco and rubber plantation area of
Sumatra’s East Coast as in European countries if care were taken to
811
812
C. BONNE
compare the same age groups. Remarkable differences, however, appared in the site incidence of the tumors. The most striking phenomenon is the high frequency of primary cancer of the liver in both
races. Snijders and Straub's post-mortem statistics showed 30.8 per
cent of the cancers of the Chinese and 57.1 per cent of the cancers of
the Javanese to be primary carcinomata of the liver. I n the combined
hospital statistics of Sumatra's East Coast these figures were even
,higher. This primary carcinoma of the liver is nearly always a livercdl carcinoma developing in a cirrhotic liver, much like the sporadic
(VLSCS of this disease seen in colder climates and in other races. Hclminthic infections of the liver are totally out of the question as an
etiological factor, as they are unknown among the Javanese and occur
in Chinese only when imported from China. It is true that most of the
Chinese laborers in Sumatra are immigrants, but as will be seen later,
the same frequency of hepatic carcinoma occurs among the Chinese in
Java, who for the most part are born on that island and often live therc
for many generations, without any possibility of clonorchiasis, schistosomiasis o r any other hclminthic infestation affecting the liver.
Another striking feature observed by Snijders and Straub was the
scarcity of gastric carcinoma in the Javanese race, f o r this neoplasm
formed only 1per cent of all cancers found at autopsy in the combined
statistical figures of Sumatra's East Coast while among the Chinese
it took the second place (19 per cent), corning immediately after
primary carcinoma of the liver. These authors were also impressed
by the parallel difference in frequency of gastric ulcer between the two
races: among the Chinese this condition is very common, among the
Javanese it is rare.
Intestinal carcinomata were also frequently met with, an observation which is especially noteworthy in view of the frequency of inflammatory intestinal disease. Cancer of the uterus and cancer of the
penis were of rather frequent occurrence.
For the two most striking results of their investigation, the frequency of primary liver cancer in both races and the difference in
incidence of gastric carcinoma and gastric ulcer, the authors could find
no satisfactory explanations. They seriously tried to find a clue to
these problems in the different age compositions of the Javanese and
('hinese labor populations compared with each other, the Chinese being
a somewhat older class, and with European populations. Primary
liver cancer, they thought, might occur at an earlier age than most
other caneem They did not succeed, however, in finding aiiy age dis1rihutioii suitable to cover their percentages even approximately.
These classical researches by Snijders and Straub have been geiierally confirmed by other pathologists in the Netherlands East Indies,
and a number of publications in Netherlands Indian medical journals
have dealt with the subject. I n the departments of pathology in the
two medical schools a t Batavia and Surabaya and the Cancer Institute
at Bandoeng in Java, where for many years thousands of autopsies have
been performed, primary carcinoma of the liver is also thc most com-
813
CANCER IN JAVA A N D SUMATRA
mon type of cancer found and the same racial difference in the frequency of gastric cancer and of gastric ulcer is observed.
These observations, especially the difference in the behavior of the
Chinese and Javanese (Malay) races with regard to gastric disease,
seem to be of such importance, that it may be well to give some further
details on these more recent studies, and to set forth certain theories
that have been offered as explanations.
In the writer’s own laboratory (Department of Pathology, School
of Medicine, Batavia, Java) attached to a large general hospital, 6043
autopsies were performed between June 20, 1921, and July 1, 1935, in
all of which histologic studies were made. For various reasons three
periods will be distinguished and only the two largest racial groups
represented in the post-mortem records, uix. Malays and Chinese, will
be considered. Europeans, Arabs, and other groups are too infreTABLEI: DiStTibUtiOn of Tumor Deaths in Malays and Chinese
Number of
autopsies
MALAYMEN
June 20, 1921-July
July 1, 1927-July
July 1, 1932-July
MUAY WOMEN
June 20, 1921-July
July 1, 1927-July
July 1, 1932-July
CHINESEMEN
June 20, 1921-July
July 1, 1927-July
July 1, 1932-July
CHINESEWOMEN
June 20, 1921-July
July 1, 1927-July
July 1, 1932-July
1, 1927. . . . . . . . . . . . . .
1, 1932.. . . . . . . . . . . . .
1, 1935.. . . . . . . . . . . . .
1516
81 1
421
1, 1927.. . . . . . . . . . . . .
1, 1932.. . . . . . . . . . . . . .
1, 1935.. . . . . . . . . . . . . .
568
365
204
1, 1927.. . . . . . . . . . . . . .
1, 1932.. . . . . . . . . . . . . .
1, 1935.. . . . . . . . . . . . . .
687
502
364
1, 1927.. . . . . . . . . . . . . .
1, 1932.. . . . . . . . . . . . . .
1, 1935.. . . . . . . . . . . . . .
117
169
176
Number of tumors
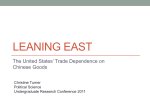
quently represented to be of statistical value. During these periods
254 malignant tumors were discovered as the cause of death; 243 of
these tumor deaths occurred in Malays and Chinese, being distributed
as shown in Table I. In this group are included all sorts of intracranial tumors.
A gradual increase of the percentages of tumor deaths is quite
obvious. It is not permissible, of course, t o draw the conclusion from
these figures that cancer is rapidly increasing. Like all proportionate
figures, they have only a relative value ; every decrease in incidence of
other diseases automatically causes an increase in the tumor figures.
There has been a gradual improvement in hygienic conditions in Java,
which is responsible f o r a decrease of infectious disease. The attitude
of the oriental population with regard to Western medicine is also
rapidly changing, and more and more patients come to the hospitals for
the internal diseases of the body. Increasing knowledge about cancer
814
C. BONNE
among the medical profession, who send in their patients, is also of a
certain importance. Older patients come to the hospitals now in larger
number than previously, a fact, which is offset, however, by the increasing number of children and babies who are brought in.
During the last three years the average tumor death rate was 6.0
per cent. While this percentage of tumor deaths in a given number of
post-mortem examinations may be lower than is met with in similar
TABLE
11: Site Incidence of 243 Tumors, Found at Autopsy in Batavia, 1921-1936,
as the Cause of Death
I
1
Site
Uterus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Breast . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Liver . . . . . . . . . . . . . .
Stomach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Esophagus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Duodenum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Jejunum, ileum. . . . . . . . . . . . . . . . . . . . . . . . . .
Colon.. .
Rectum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Tongue . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Lip, mouth, jaw.. . . . .
.................
Nasopharyngeal cavity. . . . . . . . . . . . . . . . . . . .
Pancreas . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Lung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Bladder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Skin , . . . . . . . . . . . . . . . . . . . . . . .
Neck . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Iritracranial . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Prostate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Larynx . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Thyroid . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Ovaries
..........................
Vulva. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Penis. . . . . . . . . . . . . . . . . . . . . . . . . .
Other localities. . . . . . . . . . . . . . . . . . . . . . . . . . .
___-
Sarcomata.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
TOTAL
Number of autopsies
I
1
Chinese
Malay
Total
Men
18
1
-
1
1
10
3
4
4
16
6
7
2
1
1
Women
Women
25
8
31
10
40
6
1
8
1
4
10
-
1
7
1
20
6
4
8
1
1
_.
7
1
5
2
-
18
15
10
2
3
2
3
2
1
6
-
1
3
2
-
-
1
3
1
_-
2o
6
39
99
2748
79
1137
50
1553
15
462
243
5900
Tumors in other races 11. Autopsies in other races 143.
statistics of Western countries, it must be borne in mind that the 9 . ~ 1 1 cral mortality of the population is greater (about 25 per cent) and t h c
higher age groups a r e less well represented, so that a lower percentage
of' tumor deaths may be expected. I n J a v a we do not have at our
disposal records for the various diseases giving the cause of death,
collected under medical supervision in a registered population, such as
we have in Western countries and such as Snijders and Straub and
others could collect under almost ideal conditions among the laborers
in the tobacco and rubber estate districts of Sumatra, where medical
CANCER IhT JAVA AND SUMATRA
815
supervision is excellent, where a very high percentage of the deaths
take place in the estate hospitals, and where autopsies are frequently
performed. From all we know about cancer in Java, however, there
seems t o be no reason why the cancer mortality should differ from that
in the Sumatran districts, where this mortality is of the same order as
in Western countries, when recalculated for a standard population.
Snijdcrs and Stranb in 1921 found a tumor death rate of 25.4 per
100,000 living Javanese males, whereas tlie figure for males in Holland
based on mortality figures f o r the period 1907-1912 and rccalculated for
the same age-composition is 24.3. F o r Javanese women and Chinese
males these comparative figures were 28.1 vs. 24.5 in Holland, and 44.1
vs. 40. 7 in Holland respectively. The Chinese labor group was older
than the Javanese group and therefore had more cancer.
Kouwenaar (2) in 1932, in the same district, found a cancer mortality of 36.1 f o r Javanese males compared with 33.8 for males in
Holland of the same age groups. F o r Chinese males the figure was
57.7 a s compared to 61.3. I n 1932 the average age of the Javanese aild
Chinese labor force was higher than in 1921, which makes the cancer
mortality higher in 1932 than in 1921.
I n his post-mortem records Kouwenaar found a tumor as the cause
of death in 5.4 per cent of Javanese males, 4.9 per cent of Javanese
females, and 8.4 per cent of Chinese males.
The site incidence of the 243 tumors discovered at autopsy i n my
department as the cause of death among Malays and Chinese is shown
in Table 11.
This tumor list is typical for any of the large hospitals in J a v a and
Sumatra. Although it is uncertain whether o r not the site incidence
of the tumors in the general population finds a reliable reflection in
statistics of this kind, we can not neglect some outstanding peculiarities. Among female patients the uterine and mammary tumors cause
a considerable part of the tumor deaths. A high incidence especially
of uterine tumors is found in general in the records of every hospital
in the Netherlands East Indies.
Liver carcinoma is the largest group among Malay and Chinese
males, and practically all these tumors a r e liver-cell carcinomata developing in cirrhotic livers. Cirrhosis of the liver is a very common
disease in Java and Sumatra. I n an extensive study ( 3 ) based on an
analysis of 12,957 autopsies and prepared by the four leading pathologists of these islands f o r the First International Congress of the Society for Geographic Pathology, cirrhosis of the liver of the Laennec
type was found to have been the cause of death in 3 per cent of all
autopsies on Malay men, 1.3 per cent of all autopsies on Malay women,
and 1.8 per cent of all autopsies on Chinese men, while primary liver
eancer had caused the death of the patieiit in 11 per cent of all autopsies
on Malay men, in 3 per cent of all autopsies on Malay women, and in
1.4 per cent of all autopsies on Chinese men.
Cirrhosis, whether causing the death of the patient o r found incidentally, whether combined with a neoplasm or not, was seen i n 6.9
816
0. BONNE
per cent of all autopsies on Malay men, in 3.5 per cent of all autopsies
on Malay women, and in 5.8 per cent of all autopsies on Chinese men.
A rough comparison of these figures with similar figures from other
localities, as f o r example California 5.5 per cent (Ophiils), Boston 5.0
per cent (Mallory), Geneva 4 per cent (Askanazy), Jena 1.5 per cent
(Rossle), Japan 2 per cent (Kachi), shows them to be large, especially
f o r the Malay men.
The general mortality of the population, its age-composition and
other factors influence these figures, but while it is impossible here to
enter into the statistical details of the problem, the fact remains that
the incidence of cirrhosis of the liver among the Malay population, if
studied from all sides, is still high, a remarkable thing for a race which
consumes very little if any alcohol. The figures do not seem t o be large
enough, however, to form in themselves a sufficient explanation for the
frequency of primary liver cancer, which in every country develops in
R small percentage of patients with cirrhosis.
Certain theories have been presented in explanation of this high
incidence of liver cancer. As mentioned before, the helminthic infestations of the liver are out of the problem. The very strongly spiced
food, especially of the Malays, has been considered to contain carcinogenic irritants. This, however, is merely a theoretical suggestion.
Any such irritants would be expected in the first place to irritate the
wall of the stomach, but, as has been pointed out, instead of being high
the incidence of carcinoma of the stomach is extremely low among the
Malays. The frequency of intestinal disorders has also been brought
forward, but here again, if any abnormal carcinogenic substance were
present, the intestinal wall would be the first place of contact, and
practically no carcinomata are seen in this site among the Malay race,
though sarcoma and lymphogranuloma of the intestine and carcinoma
of the rectum do occur. These theories therefore are mere suppositions without any sound basis.
In contrast to the frequency of primary liver cancer is the scarcity
of carcinoma of the stomach in the Malay race. Our list contains only
one case in a Javanese (Malay) man.
This is a very remarkable case. I n the stomach of this patient two ulcers were found
near each other and adjacent to the pylorus. One of them led into a kind of pouch or
recess about as big as a walnut, filled with a mucous substance. The posterior wall of
this pouch was formed by the transverse colon. On histologic examination a cancer of the
round-cell type waa discovered in the base of this last ulcer, which could not be interpreted as a cancer of the colon. It invaded the stomach wall and had to be accepted as a
true gastric cancer developing in a gastric ulcer. This Javanese man had emigrated to
French Caledonia as a contract laborer. After finishing his contract, he returned to Java
and died on his arrival in Batavia from gastric hemorrhage.
In Chinese men gastric carcinoma ranks second in frequency. This
difference between Malays and Chinese is a constant and most astounding phenomenon, met with in every list of autopsies of the Netherlands
Indian hospitals. It is paralleled by a similar difference in incidence
of gastric ulcer. My autopsy records from July 1,1927 to July 1,1935,
CANCER I N J A V A AND SUMATRA
817
show 9 deaths among the Chinese from gastric ulcer, but not a single
death from gastric ulcer among the Malays, except the case just mentioned, in which carcinoma developed in the ulcer. During this period
there were 1516 autopsies on Malay men, 568 on Malay women, 687 on
Chinese men, and 117 on Chinese women.
There is practically no surgery of the stomach done on the Malay
race, but there is ample opportunity for gastric surgery in Chinese
and Europeans living in Java and Sumatra. There is no imaginable
reason why'the Malays should stay away from the hospitals when
suffering from gastric ulcer or gastric carcinoma, while they present
themselves in large numbers for all kinds of other intestinal disorders,
or why they should not come to autopsy if these diseases have been the
cause of death.
Twenty-three tentative diagnoses of gastric or duodenal ulcer in
Chiiiese patients er ere traced in the records of the general civil hospital
of Ratavia for the years 1931 t o 1933 against three similar diagnoses on
native patients, of whom onc was known to have a Chinese mother.
Many of these clinical diagnoses are, of course, open to criticism, and
the presence of duodenal ulcers complicates the problem, but at all
events the proportion 23 :3 disagrees considerably with the proportion
of Chinese and native patients in general in the hospital, which was
about 1 : 3 for these same years, the exact figures being 5937 Chinese
and other foreign orientals against 17,292 native patients.
We do not know at present whether the prevalence or scarcity of
gastric carcinoma depends on constitutional genetic factors or on
external factors of irritation, or on both. Pathologists in Holland are
not as a rule very favorably inclined towards the view that an anatomical relationship exists between gastric ulcer and gastric cancer.
The peculiar behavior of these two conditions in Javanese and Sumatran natives may indicate, however, that they are both related to a
common factor of etiological importance. This factor may be an inborn
racial character o r may be something in the life habits of the Malays.
If the presence o r absence of gastric carcinoma depends largely on
the action of irritants, we have to look f a r these irritants in the diet.
There are substances in Chinese and European foods which are lacking
in Malay foods. The Malay food is much more predominantly vegetarian and the Malays are, besides, nearly all Mohammedans and hence
do not eat pork. There are many minor differences, also, in diet, but
Eastern diets like others are very complicated. The Mohammedan
Lent, which is rather strictly adhered to, may be of influence. The
consumption of alcoholic beverages among the Malays is certainly
smaller than among Europeans and Chinese.
When I brought these figures to the attention of Dr. Louis I. Dublin
of the Metropolitan Life Insurance Co. of New York, he saw at once
the importance of these observations for the problem of gastric carcinoma. He had the frequency of gastric carcinoma among the Jews
restudied by the statistical department of the Metropolitan Life Insurance Company, but although an extensive survey was made of the
818
C. BONNE
available literature, there did not seem to be any indication that the
disease was less prevalent among Jews than among Gentiles, an
observation which does not tend to give special weight t o the pork-eating habit. Figures of any reliability for vegetarians seemed to bc
unobtainable and all data with regard t o the possible influence of
alcohol consumption were extremely vague.
More statistical data on cancer mortality and site incidence especially in the F a r East are desirable if we are to be able by comparison
of racial customs to eliminate the possible etiological importance of
some of the factors mentioned above. Even proportionate figures such
as are presented here, preferably based on autopsy records, have
a certain value and in the immense unregistered populations of the Far
East any other than proportionate figures will probably not be availahlc in most countries f o r a long time.
(yitrciiioma of the esophagus is not represented in Table IT, but is a
rare condition generally. I observed a small carcinoma of the esopllztp i s , whi(~h,however, was not the cause of death, in a Chinese woman
and another removed by operation on a Malay woman. I n a combined
list of 6860 tumors, including 1155 in Europeans, 4823 in Malays, 733
in Chinese, and 149 in other races, collected during the years 19271932 by the pathologists of Medan (Sumatra), Batavia (Java), Bandoeng (Java), and Surabaya (Java) from autopsies and specimens submitted for histologic examination and published by Vos in the report of
the Netherlands India Cancer ‘Institute for 1934, there were 8 carcinomata of the esophagus in Chinese against 1 in a Malay. This may
indicate a difference in frequency between the two races similar to that
observed in the stomach.
No carcinomata in the small intestine have been found at autopsy
in my laboratory in Chinese or Malays, but I have several cases in
both races of sarcoma or lymphogranuloma. I have specimens removed
at operation from the colon in both races. The rectum is represented
by 5 Malay and 2 Chinese cases. I n Vos’ combined list there are 18
cases in Malay men, 12 in Malay women, 6 in Chinese men and 5 in
Chinese women. The frequency of rectal carcinoma seems to be that
usually recorded.
The oral mucosa, especially of the cheek, is a frequent site f o r carcinoma in the Malay, but not in the Chinese. There are 10 male and 10
female Malay cases in my list but none among the Chinese. Here again
a racial difference certainly presents itself. Vos mentions 33 tumors
in natives against 3 in Chinese. Whether this is due to betel-diewing
or not remains uncertain for the present.
Another peculiarity is the high figure for skin carcinomata in male
Malays. These tumors are nearly all carcinomata of the leg, developing on neglected skin ulcers below the knee. They invade the tibia or
the bones of the feet and lead to amputation or death tl~ronghmetastases or complications.
The last group calling f o r attention is constituted by tumors of tlic
cervical lymph nodes. Such tumors caused death 10 times in native
CdNCER I N J.4V.4 A N D SUMATRA
819
Malays and 4 times in Chinese, and are frequently removed at operation. A small proportion of these tumors of the neck, not included in
the above list, appear to be cases of lymphogranuloma; a certain number are readily classified as lymphosarcoma o r reticulum-cell sarcoma,
but a large percentage offer unusual difficulties of diagnosis. Many of
them resemble lympho-epitheliomata and transitional-cell carcinomata
histologically. However, no primary tumors in the nasopharyngeal
cavity were discovered on repeated clinical or post-mortem examinations. The subject is too complicated t o be casually entered into, but
the frequency of this type of tumor in comparison with other tumors
certainly forms a problem not only in J a v a and Sumatra but also in
other countries of the Far East.
TABLE
111:Site Incidence of Cancer in the Far East
BATAVIA
Native Malays
Chinese
Liver. . . . . . . . . .26
Uterus. . . . . . . . .25
Jaw and oral
mucosa . . . . . . . .20
Skin. . . . . . . . ..16
Neck.. . . . . . . . . 1 1
Intracranial
tumors.. . . . . . . 9
Breast.. . . . . . . . 8
Bladder.. . . . . . . 5
Rectum. . . . . . . . 5
Lung . . . . . . . . . . 4
Liver. . . . . . ,14
Uterus. . . . . . 6
Stomach. . . . 5
Neck . . . . . . . . 4
Lung.. . . . . . . 4
Pancreas. . . . 3
Breast. . . . . . . 2
Bladder. . . . . 2
Rectum. . . . . 2
S k in . . . . . . . . 2
SINQAPORE
Chinese
Liver. . . . . . . . .46
Stomach. . . . . .29
Esophagus. . . . .15
Lung.. . . . . . . . 8
Neck.. . . . . . . . 7
Rectum.. . . . . . 6
Breast.. . . . . . . 5
Pancreas. . . . . . 5
Intracranial
tumors . . . . . . . . 4
Nasophsrynx . . 3
TOKIO
(5)
Japanese
Stomach .42.68%
Liver.. . . . 6.71%
Esophag u s . . . . . . 5.45%
Lung.. . . . 5.45%
Uterus. . . 4.36%
Gallbladd e r . . . . . . 4.11%
Rectum . . 3.23%
Jaw.. . . . . 2.91%
Bile-ducts 2.78%
Pancreas. 2.60%
MANILA(4)
Filipinos
Liver and gallbladder. . . . . . . .67
Stomach and
duodenum. . . . .23
Uterus.. . . . . . . .19
Neck.. . . . . . . . .16
Pharynx and
esophagus. . . . . . 6
Head. . . . . . . . . . 6
Pancreas. . . . . . . 5
Retroperitoncal 4
Cheek, larynx
ovary and prostate each. . . . . . 3
This series shows a complete absence of carcinoma of the gallbladder, which may be due to the rarity of gall-stones. I n other laboratories occasional carcinomata of the gallbladder have been observed in
both races. Especially in the Malay race pathological conditions of the
gallbladder are great rarities, but here again we have a problem too
many-sided to be discussed in a few words.
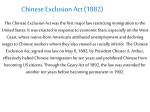
It is interesting to compare the site incidence of malignant tumors
as found at autopsies in native Malays and Chinese in Java and Sumutra with other tumor statistics of the Far East (Table TIT). Dr. Tull,
I’rofessor of Pathology of the King Edward College of Aledicine i n
Singapore, kindly gave me his figures f o r Singapore. Dr. V d d e r (4)
described his findings for Filipinos in Manila in 1927. F o r compurison I add a large Japanese collection of statistics compiled under the
supervision of Nagayo (5). For each race or locality only the teri
tumor sites of highest incidence are given.
The frequency of primary liver cancer is very obvious in Batavia,
Singapore and Manila. The stomach takes the second place or even
the first in every list except the Malay list from Batavia, which is
820
C . BONNE
representative for J a v a and Sumatra in general, where it drops out
entirely, and the Chinese list from Batavia, where it ranks third. I t
should be kept in mind that among the Chinese in Batavia and Singapore the number of males is much larger than the number of females,
which together with the usual factors present everywhere, such as
discharge to home after treatment, brings down the figure for uterine
and mammary carcinoma. Discharge after treatment naturally influences also the reported frequency of cancer of the buccal cavity, the
neck, the rectum, the breast, the skin, etc. The combined list of tumors,
collected by the four pathologists at Batavia, Bandoeng, Medan and
Surabaya in the period 1927-1932 from autopsies and specimens submitted for histologic examination, published by Vos (6), includes 1806
carcinomata in Malays and 404 in Chinese. The regional distribution
is a little different here, through the absence of this discharge factor.
The ten leading regions for each race are :
Yalays
Chinese
Skin ...............................
Uterus ..............................
538
195
Uterus
Liver
164
133
100
Skin
...............................
Liver
..............................
...............................
................................
Breast ..............................
Stomach ............................
Eye, orbit, etc. ......................
Breast ..............................
Jaw, oral mucosa . . . . . . . . . . . . . . . . . . 80 Penis ...............................
Penis ...............................
65 Pharynx ............................
Ovary ..............................
62 Neck ...............................
Neck ...............................
56 Rectum .............................
Eye, orbit ...........................
54
Salivary glands ......................
78
59
47
88
24
21
16
13
11
8
From these figures the prominent position of primary liver cancer
in certain tropical parts of the F a r East is undeniable and the special
position of the Malays as regards gastric cancer is again brought out.
The unusual frequency of lymphatic tumors of the neck shown here
offers another problem of importance.
SUMMARY
Outstanding features of tumor pathology in Java and Sumatra are
as follows :
(1) The extremely high incidence in native Malays and Chinese of
primary liver cancer. This form of cancer shows the highest incidence
in all statistics of autopsies in Netherlands India. It is nearly always
a liver-cell carcinoma, developing in a cirrhotic liver, cirrhosis of the
liver of the Laennec type and not due to parasites being prevalent
among both races but especially among native Malay males.
(2) The great rarity of gastric carcinoma among the native Malays
bnt not among the Chinese, associated with a similar difference in frequency for gastric ulcer in the two races.
( 3 ) A certain frequency of oral carcinoma, especially of the check,
in native men and women but not among the Chinese, which may or may
not depend on the betel-clicwing habit.
CANCER I N JA4VA AND SUMATRA
82 1
(4) The prevalence of carcinomata of the lower parts of the legs
in native Malay men, depending on the great number of ulcers present
on the legs of these natives.
(5) A peculiar frequency of malignant tumors of the cervical lymph
nodes in Malays and Chinese, a problem very complicated in its histologic aspects. Many of these tumors arise probably primarily from
the reticulo-endothelial elements of these glands.
(6) Rarity of carcinoma of the gallbladder associated with infrequency of gall-stones.
The most important of these peculiarities were pointed out by
Snijders and Straub in 1921. They have been confirmed and substantiated by all subsequent researches on these subjects.
Similar problems present themselves in other parts of the Far East.
The infrequency of gastric carcinoma and gastric ulcer, however, seems
to be a special feature of the Malay race inhabiting J a v a and Sumatra
and other islands of the Malay Archipelago.
There is much need of a comparative statistical investigation of
autopsy records in various Eastern countries with regard to frequency
and site incidence of cancer.
1. SNIJDERS
AND STRAUB:
Geneesk, tijdschr. v. Neder1.-Indie 61: 625, 1921. Trans. 5th
Congress of Far Eastern Association of Tropical Medicine, Singapore, 1923 (in
English).
W. : Geneesk. tijdschr. v. Neclerl.-IndiB 72 : 392, 1932.
2. KOUWENAAR,
3. Geneesk. tijdschr. v. Neder1.-Indie 71 : 506, 1931.
4. VEDDER,
E. B.: J. A. M. A. 88: 1627,1927.
5. NAGIFO: Congress of Internal Medicine, Madrid, 1933, Tome 111.
6. VOS,J. J. TH.: Report of Netherlands Indian Cancer Institute for 1934.