Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
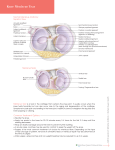
Guide for Meniscus Diagnosis By Daniel Bossen & Marcel Jurado Index Introduction ................................................................................ 3 Anatomy .................................................................................. 3 Vascular Anatomy ..................................................................... 4 Neuroanatomy .......................................................................... 5 Biomachanics .......................................................................... 5 Meniscal healing ....................................................................... 7 Mechanism of Meniscal and Ligamentous Knee Injuries.................. 7 Patient History............................................................................. 9 Instruction meniscus tests .......................................................... 11 Joint line tenderness (JLT)........................................................ 11 McMurray test......................................................................... 11 Apley (grind) test.................................................................... 12 The Thessaly Test at 5° and 20° of flexion ................................ 12 Ege’s Test ............................................................................. 14 Flowchart.................................................................................. 16 References................................................................................ 17 2 Introduction The various diagnostic tests are important to assess a menisculesion. The intake, however, is the most important tool of the assessment. A diagnosis can be made accurately in 75% of the meniscal injuries on the basis of the history alone. This guide lists the necessary points to guarantee a complete meniscus examination. It consists of essential background information about the menisci, shows the most important questions regarding the patient history and gives a description of the most common meniscus tests. Instantaneous damage to both ligamentous and meniscal structures is more common than isolated injury1 with the combination of meniscus and ACL as the most frequent one.2 Therefore this guide not only focuses on the meniscus, but also takes the significance of the knee ligaments into consideration. Why Is the Diagnosis Important? Ten percent to 15% of adults in the community report knee symptoms with over 3.3 million new visits made annually (USA).3,4 Overall, knee pain accounts for 3% to 5% of all visits to physicians and a substantial proportion result in referrals for diagnostic imaging and/or specialty care.5 A careful history taking and physical examination can assist the examiner in determining whether the knee pain is part of a systemic condition or whether it represents a local musculoskeletal problem. If the knee pain is part of a local regional musculoskeletal disorder, the clinician must decide whether the pain represents a torn meniscal or ligamentous structure and then whether nonoperative or operative intervention is indicated. Since torn meniscal or ligamentous structures can cause significant pain and disability, injuries to these structures may require expeditious repair. The physical examination can aid the primary care clinician in assessing the likelihood of a torn meniscal or ligamentous structure and whether a referral will be beneficial. Background information Anatomy 6 The menisci (Fig. 1) extend the superior tibial surface, improving its congruency with the femoral condyles. Both menisci are fibro-cartilaginous and wedge shaped in the coronal plane. The medial meniscus is more crescent shaped, and the lateral meniscus is more circular. The superior portions of the menisci are concave, enabling effective articulation with their respective convex femoral condyles, whereas the inferior surfaces are flat to conform to the tibial plateaus. Anterior and posterior meniscal horns attach to the intercondylar eminence of the tibial plateau. The coronary ligaments provide peripheral attachments between the tibial plateau and the perimeter of both menisci. The medial meniscus is also attached to the medial collateral ligament, which limits its mobility. 3 The lateral meniscus is connected to the femur via the anterior (ligament of Humphrey) and posterior (ligament of Wrisberg) meniscofemoral ligaments, which can tension its posterior horn anteriorly and medially with increasing knee flexion. The transverse ligament provides a connection between the anterior aspects of both menisci. The increased stability provided by the ligamentous attachments prevents the menisci from being extruded out of the joint during compression. Figure 1 Vascular Anatomy 6 Vascular supply is crucial to meniscal healing. The medial, lateral, and middle geniculate arteries, which branch off the popliteal artery, provide the major vascularization to the inferior and superior aspects of each meniscus.The middle geniculate artery is a small posterior branch that pierces the oblique popliteal ligament at the posteromedial corner of the tibiofemoral joint. A premeniscal capillary network arising from branches of these arteries originates within the synovial and capsular tissues of the knee along the periphery of the menisci. Only 10% to 30% of the peripheral medial meniscus border and 10% to 25% of the lateral meniscus border receive direct blood supply. Endoligamentous vessels from the anterior and posterior horns travel a short distance into the substance of the menisci and form terminal loops, providing another direct route for nourishment. The remaining portion of each meniscus (65% to 75%) receives nourishment only from the synovial fluid via diffusion. 4 Neuroanatomy 6 The knee joint is innervated by the posterior articular branch of the posterior tibial nerve and the terminal branches of the obturator and femoral nerves. Nerve fibers penetrate the joint capsule, along with the vascular supply, and service the substance of the menisci. Ruffini, Pacinian, and Golgi tendon mechanoreceptors have been identified in the knee joint capsule and in the peripheral menisci. Type I (Ruffini) mechanoreceptors are low threshold and slowly adapting to changes in static joint position and pressure. Type II (Pacinian) mechanoreceptors are low threshold and fast adapting to tension changes, signaling joint acceleration. Type III (Golgi) mechanoreceptors signal when the knee joint approaches the terminal range of motion (ROM) and are associated with neuromuscular inhibition. Concentrations of meniscal mechanoreceptors (especially Pacinian mechanoreceptors) are greatest in the meniscal horns, leading researchers to study their contributions to proprioception. Biomachanics 7 The main function of the menisci is one of load transmission. The majority of the collagen fibres are large and coarse and are arranged in a circumferential manner. These fibres are stabilised with radially running fibres acting as ties. This structure suggests the ability to bear load is by containment of the socalled ‘hoop stresses’ (Fig. 2). Figure 2 A compressive force (white arrow) is converted by the shape of the meniscus to a radially directed force (black arrow), which is taken up as tension force (dashed arrow) within the meniscus. It has been determined that approximately 50% of the body’s weight is transmitted through the menisci in extension and up to 85% in 90° of flexion. The menisci, however, are mobile structures that move anteriorly and posteriorly to allow maintenance of congruency throughout the range of flexion. The radius of curvature also changes to accommodate the reduced radius of the femoral condyles as flexion and rollback occurs. The medial meniscus is more restrained than the lateral meniscus, particularly in the postero-medial corner, and this may explain why tears of this area are more common. 5 It is now well accepted that loss of all or part of a meniscus increases point loading and results in premature wear of the knee due to altered mechanical forces. The rate at which arthrosis develops, however, depends on a number of factors and these may be regarded as knee factors and patient factors. The volume of meniscus lost has been considered. Total menisectomy has been estimated to reduce the joint surface contact area by 75%, increasing local peak contact pressure by 235%. Partial menisectomy also reduces contact area by 10% and increases point pressures by 65%. The nature of the tear is important. Radial tears extending to the periphery may not result in much volume loss but may completely defunction the meniscus through an inability to resist hoop stresses. Associated injuries either at the time of meniscal tear or subsequently, such as chondral damage and anterior cruciate ligament rupture, will also have a significant effect on the knee’s long-term prognosis. Patient factors include limb alignment, age at time of injury, activity level, weight and inherent genetic constitution. The menisci also act as secondary stability restraints in the knee. The effect in a stable knee remains controversial but in an ACL deficient knee there is no doubt that loss of a meniscus increases measurable joint laxity. In these situations, it is suggested that the intact posterior horn of the medial meniscus acts as a wedge or ‘stop’ to anterior translation of the tibia (Fig. 3). Figure 3 With ACL deficiency an anterioly force (white arrow) is partly resisted by an intact medial meniscus (black arrow). If the meniscus is also deficient then the tibia can move further anteriorly. Unfortunately, it is not uncommon to witness an ACL deficient knee in an active individual sequentially undergoing medial and lateral menisectomies with a rapid progression to premature arthrosis. Further biomechanical functions of the menisci have been postulated. These include shock absorption, lubrication, joint nutrition and proprioception. The menisci exhibit viscoelastic properties, which may serve to attenuate impacts sustained through the knee on loading. The improved congruity that they provide has been suggested to aid joint lubrication and cartilage nutrition by promoting fluid shifts in and out of the cartilage surface layers. Recent studies have shown the presence of mechano-receptors and free nerve endings in the peripheral, two thirds of the meniscus body and the horns, particularly the posterior horns. This suggests an important role of the menisci in proprioceptive feedback, the initiation of protective reflexes and joint pain. This may also explain why meniscal tears without a significant mechanical component can still be a source of painful symptoms. 6 Meniscal healing 7 The capacity of meniscus to heal is limited, particularly the central portions, which are largely avascular, aneural and alymphatic. However, in 1936, King showed that meniscal healing in dogs could occur providing there was communication with the peripheral blood supply. As with other soft and bony tissues, there is a need for a balance between blood supply, and hence associated cellular and tissue repair factors, and component stability to permit healing. The process would appear to be along the same lines as healing in other soft tissues and, in the vascular portion of the meniscus, it would appear that healing is largely complete by 10 weeks, although maturation of the scar may continue for many months. As indications for meniscal repair are extended, attempts to promote an environment more conducive to healing have been introduced. The vascular anatomy of the human meniscus has been well described by Arnoczky and Warren. The blood supply is by way of the superior and inferior medial and lateral geniculate arteries. The outer rim of the meniscus is vascularized up to 30% of its width on the medial side and 25% on the lateral side. In addition, there is a synovial fringe that extends some 3 mm over the surface of each meniscus adding further to the peripheral vascularity. The concept of ‘red-on-red’, red-on-white’ and ‘white-on-white’ tears, describing the vascular status of each tear location, is a useful classification. ‘Red-on-red’ tears are perhaps a misnomer as all tears must be ‘redonwhite’, as the central portion, by its nature, must have had its vascular supply disrupted. Nevertheless, it is a reflexion of the peripheral location and is a good indicator that healing should occur. ‘White-on-white’ tears are located within the avascular zone and hence have the least potential to heal. The majority of reports on meniscal repair address primarily longitudinal tears, which are indeed the commonest tear to be repaired. Current practice suggests that certain tears are incapable of healing although anecdotally this has not been our experience. As with any scarred tissue, it is likely, however, that even fully healed menisci will not regain normal biomechanical strength. Indeed, there is some evidence at 12 weeks after meniscal suture, meniscal strength may be significantly reduced at only 26% of the normal side. Mechanism of Meniscal and Ligamentous Knee Injuries The position of the joint at the time of the traumatic force dictates which anatomic structures are at risk for injury; hence, an important aspect of obtaining the patient history for acute injuries is to allow him/her to describe the position of the knee and direction of forces at the time it was injured. In full knee extension, the ACL and PCL limit the antero-posterior motion of the tibia on the femur. The ACL is often injured during traumatic twisting injuries in which the tibia moves forward with respect to the femur, often accompanied by valgus stress. No direct blow to the knee or leg is required, but the foot is usually planted and the patient may remember a "popping" sensation at the time of the injury. 7 Similar to the ACL, PCL injuries often occur during twisting with a planted foot in which the force of the injury is directed posteriorly against the tibia with the knee flexed. The most common collateral ligament injury results from an abduction and external rotation force applied on a knee in an extended or slightly flexed position. An intact MCL helps the ACL prevent posterior motion of the femur. An injury to the MCL may allow for anterior subluxation of the tibial plateau during flexion, especially in an ACL-deficient patient. Meniscal injuries typically occur through application of specific forces while the knee joint is in certain positions. During flexion, if the tibia is rotated internally, the posterior horn of the medial meniscus is pulled toward the center of the joint. This movement can produce a traction injury of the medial meniscus, tearing it from its peripheral attachment and producing a longitudinal tear of the substance of the meniscus. With aging, the meniscal tissue degenerates and can delaminate, thus making it more susceptible to splitting from shear stress, resulting in horizontal cleavage tears. Without the menisci, the loads on the articular surfaces are increased significantly leading to a greater potential for degenerative arthritis. Since the menisci are without pain fibers, it is the tearing and bleeding into the peripheral attachments as well as traction on the capsule that most likely produce a patient's symptoms of pain. In fact, 16% of asymptomatic patients have meniscal tears demonstrated on magnetic resonance imaging (MRI) with the incidence increasing to 36% for patients older than 45 years.8 With posterior horn tears, the meniscus can return to its anatomic position with extension. If the tear extends anteriorly beyond the MCL creating a bucket-handle tear, then the unstable meniscus fragment cannot always move back into an anatomic position. Such a meniscal tear can result in locking of the knee in a flexed position. The lateral meniscus, being more mobile, is less likely to be associated with locking when torn. The patient may also note a "clicking" sensation while walking due to traction against a torn medial or lateral meniscus. Locking of the knee is more common in younger patients with meniscal tears. Older patients are more likely to have degenerative meniscal tears with less mechanical symptoms and an insidious onset. 8 Patient History 9 These questions are important during the intake. The questions are specific for detecting meniscus laesies. The questions are indispensable during the patient’s history. 1. How did the injury occur or what was the mechanism of injury? The primary mechanisms of in the knee are valgus force (with or without rotation), hyperextension, flexion with posterior translation, and varus force. The first often results in injury to the medial collateral ligament, frequentlyaccompanied by injury to the posteromedial capsule, medial meniscus, and anterior cruciate (‘terrible triad’). 2. Did the injury occur during acceleration, during deceleration, or when the patient was moving at a constant speed? Acceleration and twisting injuries may involve the meniscus. Deceleration injuries often involve the cruciate ligaments. Constant speed with cutting may involve the anterior cruciate ligament. 3. Does the knee ‘give way’? This finding usually indicates instability in the knee, meniscus pathology, patellar subluxation (if present when rotation or stoping is involved), undisplaced osteochondritis dissecans, patellofemoral syndrome, plica or loose body. ‘Giving way’ when walking uphill or downhill is more likely the result of a retropatellar lesion. 4. Has the knee ever locked? True locking of the knee is rare. Loose bodies may cause recurrent locking. Locking must be differentiated from catching, which is the momentary locking or giving way as a result of reflex inhibition or pain. Locking in the knee usually means that the knee cannot fully extend with flexion often being normal, and is related to meniscus pathology. 5. Is the joint swollen? Does the swelling occur with activity or several hours after activity, or does the joint feel tight at rest? Swelling with activity may be caused by instability, and tightness at rest may be caused by arthritic changes or patellofemoral dysfunction. Is the swelling recurrent? If so, what activitiy causes it? Swelling with pivoting or twisting may be a result of meniscus problems or instability at the tibiofemoral joint. 9 Figure 4 Mechanisms of the knee and Possible Structures Injured 9 Varus or valgus contact without rotation 1. 2. 3. Collateral ligament Epiphyseal fracture Patellar dislocation or subluxation Varus or valgus contact with rotation 1. 2. Collateral or cruciate ligaments Collateral ligaments and patellar dislocation or subluxation Meniscus tear 3. Blow to patellofemoral joint, or fall on flexed knee, foot dorsiflexed 1. Patellar articular injury or osteochondral fracture Blow to tibial tubercle, or fall on flexed knee, foot plantar flexed 1. Posterior cruciate ligament Anterior blow to tibia, resulting in knee hyperextension 1. 2. Anterior cruciate ligament Anterior and posterior cruciate ligament 1. 2. Anterior cruciate ligament Posterior capsule 1. Anterior cruciate ligament 1. Anterior cruciate ligament Noncontact, quickly turning one way with tibia rotated in opposite direction 1. Patellar dislocation or subluxation Noncontact, rotation with varus or valgus loading 1. Meniscus injury 1. 2. Meniscus injury Osteochondral fracture Hyperflexion 1. 2. Meniscus (posterior horn) Anterior cruciate ligament Forced medial rotation 1. Meniscus injury (lateral meniscus) Forced lateral rotation 1. 2. 3. Meniscus injury (medial meniscus) Medial collateral ligament and possibly anterior cruciate ligament Patellar dislocation Flexion-varus-medial rotation 1. Anterolateral instability Flexion-varus-lateral rotation 1. Anteromedial instability Dashboard injury 1. 2. Isolated posterior cruciate ligament Posterior cruciate ligament and posterior capsule Posterolateral instability Posteromedial instability Patellar fracture Tibial fracture (proximal) Tibial plateau fracture Acetabular and pelvic fracture Noncontact hyperextension Noncontact deceleration Noncontact deceleration, with tibial medial rotation or femoral lateral rotation on fixed tibia Noncontact, compressive rotation 3. 4. 5. 6. 7. 8. 10 Instruction meniscus tests Tests for Meniscal Injuries 10 Meniscal tears occur commonly, however, their clinical diagnosis is often difficult, even for an experienced clinician. Because the menisci are avascular and have no nerve supply on their inner two thirds, an injury to the meniscus can result in little or no pain or swelling, which makes accurate diagnosis even more challenging. In 1803, Hey described “internal derangement of the knee,” and since then a significant literature on the clinical diagnosis of meniscal tears has evolved.11 Joint line tenderness (JLT) 10 Joint line palpation is among the most basic maneuvers, yet it often provides more useful information than the provocative maneuvers designed to detect meniscal tears. Flexion of the knee enhances palpation of the anterior half of each meniscus. The medial edge of the medial meniscus becomes more prominent with internal rotation of the tibia, allowing for easier palpation. Alternatively, external rotation allows improved palpation of the lateral meniscus. McMurray test 10 The McMurray test is among the primary clinical tests to evaluate for a meniscal tear. McMurray12 first described the test in 194013 The original description of the test, as described by McMurray, was: In carrying out the manipulation with patient lying flat, the knee is first fully flexed until the heel approaches the buttock; the foot is then held by grasping the heel and using the forearm as a lever. The knee being now steadied by the surgeon’s other hand, the leg is rotated on the thigh with the knee still in full flexion. During this movement the posterior section of the cartilage is rotated with the head of the tibia, and if the whole cartilage, or any fragment of the posterior section, is loose, this movement produces an appreciable snap in the joint. By external rotation of the leg the internal cartilage is tested, and by internal rotation any abnormality of the posterior part of the external cartilage can be appreciated. By altering the position of flexion of the joint the whole of the posterior segment of the cartilages can be examined from the middle to their posterior attachment… Probably the simplest routine is to bring the leg from its position of acute flexion to a right angle, whilst the foot is retained first in full internal, and then in full external rotation… When the click occurs with a normal but lax cartilage, the patient experiences no pain or discomfort, but when produced by a broken cartilage, which has already given trouble, the patient is able to state that the sensation is the same as he experienced when the knee gave way previously.10 11 Apley (grind) test 10 The Apley (grind) test was described by Apley in 1947.14,15 The original description of the test follows: For this examination the patient lies on his face. He should be on a couch not more than 2 feet high, or the tests become difficult, and he must be well over to the edge of the couch nearest the surgeon. To start the examination, the surgeon grasps one foot in each hand, externally rotates as far as possible, and then flexes both knees together to their limit. When this limit has been reached, he changes his grasp, rotates the feet inward, and extends the knees together again. . . . The surgeon then applies his left knee to the back of the patient’s thigh. It is important to observe that in this position his weight fixes 1 of the levers absolutely. The foot is grasped in both hands, the knee is bent to a right angle, and the powerful external rotation is applied. This test determines whether simple rotation produces pain. Next, without changing the position of the hands, the patient’s leg is strongly pulled upward, while the surgeon’s weight prevents the femur from rising off the couch. In this position of distraction, the powerful external rotation is repeated. Two things can be determined: (1) whether or not the maneuver produces pain and (2), still more important, whether the pain is greater than in rotation alone without the distraction. If the pain is greater, the distraction test is positive, and a rotation sprain may be diagnosed. Then the surgeon leans well over the patient and, with his whole body weight, compresses the tibia downward onto the couch. Again he rotates powerfully, and if addition of compression had produced an increase of pain, this grinding test is positive, and meniscal damage is diagnosed. The Thessaly Test at 5° and 20° of flexion 16 The Thessaly test is a dynamic reproduction of load transmission in the knee joint and is performed at 5° and 20° of flexion. It was named in honor of the county, or prefecture, in our country, where our hospital serves as an academic medical referral center and which has a continuous, uninterrupted ten-thousand-year history. The examiner supports the patient by holding his or her outstretched hands while the patient stands flatfooted on the floor. The patient then rotates his or her knee and body, internally and externally, three times, keeping the knee in slight flexion (5°). Then the same procedure is carried out with the knee flexed at 20° (Fig. 5). 12 Figure 5 Thessaly Test at 20° of flexion 16 Lateral view of Thessaly at 20° Frontal view in neutral position Frontal view in external rotation Frontal view in internal rotation Patients with suspected meniscal tears experience medial or lateral joint-line discomfort and may have a sense of locking or catching. The theory behind the test is that, with this maneuver, the knee with a meniscal tear is subjected to excessive loading conditions and almost certainly will have the same symptoms that the patient reported. The test is always performed first on the normal knee so that the patient may be trained, especially with regard to how to keep the knee in 5° and then in 20° of flexion and how to recognize, by comparison, a possible positive result in the symptomatic knee. 13 Ege’s Test 17 The test is performed with the patient in a standing position. The knees are in extension and the feet are held 30 to 40 cm away from each other at the beginning of the test. To detect a medial meniscal tear, the patient squats with both lower legs in maximum external rotation and then stands up slowly (Fig. 6A and B). The distance between the knees increases and each knee becomes externally rotated as the squatting proceeds (Fig. 6B). Figure 6 For lateral meniscal tears, both lower extremities are held in maximum internal rotation while the patient squats and stands up (Fig. 6C and D). A full squat in internal rotation is almost impossible even in healthy individuals. So a slightly less than full squat is required in internal rotation, and the patient is allowed to use an object nearby as a support. In contrast to the medial meniscal test, the distance between the knees decreases and each knee becomes internally rotated as the squatting proceeds (Fig. 6D). The test is positive when pain and/or a click is felt by the patient (sometimes audible to the physician) at the related site of the joint line.11 Further squatting is stopped as soon as the pain and/or click is felt; hereby a full squat is not needed in all of the patients. Sometimes pain and/or click may not be felt until maximum squat, but may be felt as the patient comes out of the squat. This finding is also accepted as a positive sign of the test. Pain and/or click are felt at around 90° of knee flexion. 14 Anteriorly located tears produce the symptoms in earlier knee flexion, whereas tears located on posterior horn of the menisci produce the symptoms in more knee flexion, as in other meniscal tests. Flexion-extension and internal-external rotation components of the test are similar to that of McMurray’s test. However, the most important difference is the weightbearing position of the patient. The test may also be called the weightbearing McMurray’s test. Varus and valgus stresses are also produced during internal and external rotation positions, respectively. 15 Flowchart 16 References 1. Solomon DH, Simel DL, Bates DW, Katz JN, Schaffer JL. Does This Patient Have a Torn Meniscus or Ligament of the Knee? Value of the Physical Examination. JAMA 2001; 286:1610-1620 2. Binfield PM, Maffulli N, King JB. Patterns of meniscal tears associated with anterior cruciate ligament lesions in athletes. Injury 1993 Sep;24(8):557-61. 3. Praemer A, Furner S, Rice DP. Musculoskeletal Conditions in the United States. Rosemont, Ill: American Academy of Orthopedic Surgeons 1999. 4. Cunningham LS, Kelsey JL. Epidemiology of musculoskeletal impairments and associated disability. Am J Public Health. 1984; 74:574-579. 5. Katz JN, Solomon DH, Schaffer JL, Horsky J, Burdick E, Bates DW. Outcomes of care and resource utilization among patients with knee and shoulder disorders treated by general internists, rheumatologists, or orthopedic surgeons. Am J Med 2000; 108:28-35. 6. Brindle T, Nyland J, Johnson DL. The Meniscus: Review of Basic Principles With Application to Surgery and Rehabilitation. J Athl Train 2001 Apr–Jun; 36(2): 160–169. 7. Boyd KT, Myers PT. Meniscus preservation; rationale, repair techniques and results. The Knee; Brisbane Orthopaedic and Sports Medicine Centre 2002. 8. Boden SD, Davis DO, Dina TS, et al. A prospective and blinded investigation of magnetic resonance imaging of the knee: abnormal findings in asymptomatic subjects. Clin Orthop. 1992;282:177-185. 9. Magee DJ. Orthopedic Physical Assessment. 2002; 4th edition 10.Malanga GA, Andrus S, Nadler SF, McLean J. Physical Examination of the Knee: A Review of the Original Test Description and Scientific Validity of Common Orthopedic Tests. Arch Phys Med Rehabil 2003; 84(4):592-603. 11.Hey W. Practical observations in surgery. Philadelphia: James Humphreys; 1805. 12.McMurray TP. The semilunar cartilages. Br J Surg 1942; 29:40713.Evans PJ, Bell GD, Frank C. Prospective evaluation of the Mc-Murray test. Am J Sports Med 1993; 21:604-8. 14.Gillis L. Diagnosis in orthopaedics. Toronto: Butterworth; 1969. 15.Gould JA, Dabies GJ. Orthopaedic and sports physical therapy. Toronto: CV Mosby; 1985. 16.Karachalios T, Hantes M, Zibis AH, Zachos V, Karantanas AH, Malizos KN. J Bone Joint Surg Am 2005; 87:955-962 17.Akseki D, Özcan Ö, Boya H, Pınar H. New Weight-Bearing Meniscal Test and a Comparison With McMurray’s Test and Joint Line Tenderness. Arthroscopy: The Journal of Arthroscopic and Related Surgery 2004; Vol 20; 9:951-958 17