Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neuropsychopharmacology wikipedia , lookup
Dual consciousness wikipedia , lookup
Neuroscience and intelligence wikipedia , lookup
Neuroeconomics wikipedia , lookup
Temporoparietal junction wikipedia , lookup
Biology of depression wikipedia , lookup
Neuropsychology wikipedia , lookup
Lateralization of brain function wikipedia , lookup
Eyeblink conditioning wikipedia , lookup
Executive functions wikipedia , lookup
Neurophilosophy wikipedia , lookup
Cortical cooling wikipedia , lookup
Persistent vegetative state wikipedia , lookup
Affective neuroscience wikipedia , lookup
Human brain wikipedia , lookup
History of neuroimaging wikipedia , lookup
Aging brain wikipedia , lookup
Neuroplasticity wikipedia , lookup
Neural correlates of consciousness wikipedia , lookup
Neurolinguistics wikipedia , lookup
Semantic Web wikipedia , lookup
Broca's area wikipedia , lookup
Embodied language processing wikipedia , lookup
Neuroanatomy of memory wikipedia , lookup
Time perception wikipedia , lookup
Emotional lateralization wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
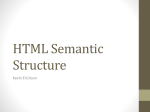
doi:10.1093/brain/awh423 Brain (2005), 128, 797–810 New insights into the anatomo-functional connectivity of the semantic system: a study using cortico-subcortical electrostimulations Hugues Duffau,1 Peggy Gatignol,2 Emmanuel Mandonnet,1 Philippe Peruzzi,3 Nathalie Tzourio-Mazoyer4 and Laurent Capelle1 Departments of 1Neurosurgery and 2Neurology, Hôpital de la Salpêtrière, 47–83 Bd de l’Hôpital, 75651 Paris, Cedex 13, 3Department of Neurosurgery, Hôpital Maison Blanche, Reims and 4UMR 6194 CNRS, CEA Universités de Caen et Paris 5, GIP Cyceron BP 5222, Bld Henri Becquerel, 14074 Caen Cedex, France Correspondence to: Hugues Duffau, MD, PhD, Department of Neurosurgery U 678, Hôpital Salpêtrière, 47–83 Bd de l’Hôpital, 75651 Paris, Cedex 13, France E-mail: [email protected] Summary Despite a better understanding of the organization of the cortical network underlying the semantic system, very few data are currently available regarding its anatomofunctional connectivity. Here, we report on a series of 17 patients operated on under local anaesthesia for a cerebral low-grade glioma located within the dominant hemisphere. Prior to and during resection, intraoperative electrical stimulation was used to map sensorimotor and language structures so that permanent neurological deficits could be avoided. In a number of cases, cortical and subcortical stimulation caused semantic paraphasias. Using postoperative MRI, we correlated these functional findings with the anatomical locations of the sites where semantic errors were elicited by stimulation, especially at the subcortical level, with the aim of studying the connectivity underlying the semantic system. In temporal gliomas, cortical sites involved in semantic processing were found around the posterior part of the superior temporal sulcus, with subcortical pathways reproducibly located under the depth of this sulcus. In insular gliomas, although stimulation elicited no semantic disturbances at the cortical level, such semantic paraphasias were generated at the level of the anterior floor of the external capsule. In frontal tumours, cortical regions implicated in semantics were detected in the lateral orbitofrontal region and dorsolateral prefrontal cortex, with subcortical fibres located under the inferior frontal sulcus. All these eloquent structures were systematically preserved, thereby avoiding permanent postoperative deficits. Our results provide arguments in favour of the existence of a main ventral subcortical pathway underlying the semantic system, within the dominant hemisphere, joining the two essential cortical epicentres of this network: the posterior and superior temporal areas, and the orbitofrontal and dorsolateral prefontal regions. Such a ventral stream might anatomically partly correspond to the inferior fronto-occipital fasciculus. Keywords: semantic; connectivity; language; electrical stimulation; glioma surgery Abbreviations: BA = Brodmann area; BDAE = Boston Diagnostic Aphasia Examination; DTI = diffusion tensor imaging; DLPFC = dorsolateral prefrontal cortex; IFC = inferior frontal cortex Received July 13, 2004. Revised December 20, 2004. Accepted December 23, 2004. Advance Access publication February 10, 2005 Introduction Recent progress in neurofunctional imaging methods has allowed an improved knowledge of the cortical organization of the semantic system. Indeed, two regions within the left hemisphere have been regularly reported as playing a major role: the left posterior temporal regions and the left inferior frontal cortex (IFC) (Mesulam, 1990; Papathanassiou et al., 2000; Davis and Johnsrude, 2003; Friederici et al., 2003; Heim et al., 2003a). Regarding the left temporal lobe, in which semantic content has been described as highly organized and spatially segregated (Bookheimer, 2002), the regions around the posterior part of the superior temporal sulcus (superior and # The Author (2005). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: [email protected] 798 H. Duffau et al. middle temporal gyri) were reproducibly found to be activated during comprehension tasks (Wise et al., 1991, 2001; Démonet et al., 1992; Tulving et al., 1994; Stromswold et al., 1996; Müller et al., 1997; Bookheimer et al., 1998; Schlosser et al., 1998; Mummery et al., 1999; Crinion et al., 2003; Davis and Johnsrude, 2003; Devlin et al., 2003; Hamberger et al., 2003; Tyler et al., 2003), whatever the modalities of presentation of information (oral, visual or somesthetic), supporting the supramodal feature of this region in semantic processing (Michael et al., 2001; Booth et al., 2002; Decety et al., 2002; Saygin et al., 2003). Moreover, visual tasks such as reading or naming might recruit additional basal inferior temporal areas that are involved in lexical retrieval (Lüders et al., 1991; Nobre et al., 1994; Damasio et al., 1996; Schäffler et al., 1996; Price, 2000; Jobard et al., 2003). Concerning the semantic role of the IFC (Mazoyer et al., 1993; Thompson-Schill et al., 1997, 1998; Wagner et al., 1997, 2001; Chee et al., 1998; Bookheimer, 2002; Homae et al., 2002), it would seem that its inferior and anterior parts, i.e. the pars orbitalis [Brodmann area (BA) 47] (Gabrieli et al., 1998; Poldrack et al., 1999; Bookheimer, 2002; Noppeney and Price, 2002), pars triangularis (BA 45) (Desmond et al., 1995; Gabrieli et al., 1996; Friederici et al., 2000b) and even the dorsolateral prefrontal cortex (DLPFC) (BA 46/9) (Kapur et al., 1994; Demb et al., 1995; Warburton et al., 1996; Szatkowska et al., 2000; Noesselt et al., 2003) might be more specifically implicated in the executive aspects of semantic processing, while its more posterior areas (notably the pars opercularis, BA 44) could be preferentially involved in syntactic (Dapretto and Bookheimer, 1999; Kang et al., 1999; Embick et al., 2000; Friederici et al., 2000a; Moro et al., 2001; Heim et al., 2002, 2003b) and phonological processings (Démonet et al., 1992; Zatorre et al., 1992; Paulesu et al., 1993; Fiez, 1997; Fiez and Peterson, 1998; Poldrack et al., 1999). Despite the better understanding of this cortical network organization, very few data are currently available about the anatomo-functional connectivity underlying the semantic system (Scott et al., 2000; Brugge et al., 2003), in contrast to the phonological system, for which a ‘phonological loop’ was both modelled (Baddeley, 1992, 2003) and described anatomically and functionally in vivo (Duffau et al., 2003a). Here, we report on a series of 17 patients operated on under local anaesthesia for a cerebral low-grade glioma located within the dominant hemisphere, with intraoperative sensorimotor and language mapping in order to avoid postoperative definitive deficit, using cortical and subcortical electrical stimulation, which all induced transient semantic paraphasia. On the basis of the data of postoperative MRI, we correlated these functional findings with the anatomical locations of the sites where semantic errors were elicited by stimulation, especially at the subcortical level, with the aim of studying the connectivity underlying the semantic system. Materials and methods Subjects Among a series of 150 patients operated on awake for a low-grade glioma located within the dominant hemisphere in our institution between 1996 and 2003, 17 patients who presented transitory semantic errors generated by the intraoperative electrical mapping were reviewed retrospectively. These patients are not the same as those described in our previous report of subcortical language pathway stimulation (Duffau et al., 2002). Preoperatively, all patients had had a neurological examination. Language was tested by a speech therapist using the Boston Diagnostic Aphasia Examination (BDAE) (Goodglass and Kaplan, 1972). Hemispheric dominance was assessed using a standardized questionnaire (Edinburgh inventory) (Oldfield, 1971) and functional MRI using a protocol previously reported (Léhericy et al., 2000). The topography of the tumour was analysed accurately on a preoperative MRI (T1-weighted and spoiled-gradient images obtained before and after gadolinium enhancement in the three orthogonal planes, and T2-weighted axial images). Intraoperative mapping All patients underwent surgery under local anaesthesia so that functional cortical and subcortical mapping could be carried out using direct brain stimulation. This method, including the electrical parameters and the intraoperative clinical tasks, has been described previously (Duffau et al., 2002, 2003b). A bipolar electrode with 5 mm spaced tips delivering a biphasic current with parameters nondeleterious for the CNS (pulse frequency of 60 Hz, single pulse phase duration of 1 ms, amplitude from 2 to 8 mA) (Ojemann Cortical Stimulator 1, Radionics*, Inc., Burlington, MA) was applied to the brain of awake patients. In a first stage, cortical mapping was performed, after tumour and sulci/gyri identification using ultrasonography, and before resection, in order to avoid any eloquent area damage. Sensorimotor mapping was performed first, with the goal of obtaining a positive response (e.g. the induction of movement and/or paraesthesia in the contralateral hemibody when the primary sensorimotor areas were stimulated in a patient at rest), since the bone flap allowed good exposure of the central region in all patients. Under local anaesthesia, the current intensity adapted to each patient was determined by progressively increasing the amplitude from 1 to 1 mA, from a baseline of 2 mA, until a sensorimotor response was elicited, with 8 mA as the upper limit, with the goal of avoiding the generation of seizures. Once this threshold was defined for sensorimotor mapping, the same intensity was used for both cortical and subcortical language mapping. Then, the patient was asked to perform an automatic task such as counting (regularly from 1 to 10 over and over), in order to confirm that the selected current amplitude allowed performance of reliable language mapping, by inducing a typical speech arrest/anarthria during stimulation of the region of Broca/ventral premotor cortex. Indeed, the essential cortical language sites are known to be inhibited by electrical stimulation (Berger, 1996; Ojemann et al., 1989; Duffau et al., 2002, 2003b). At this time, we systematically used the task most often reported during intraoperative language mapping (Ojemann et al., 1989; Berger, 1996), i.e. picture naming, preceded by a short sentence to read (the French translation of ‘this is a . . . ’), in order to check that there were no seizures generating complete speech arrest when the patient was not able to name, i.e. that he was still capable of pronouncing ‘this is a . . . ’. For the naming task, Connectivity of the semantic system we used the DO 80, which consists of 80 black and white pictures selected according to variables such as frequency, familiarity, age of acquisition and level of education (Metz-Lutz et al., 1991). The patient was never informed when the brain was stimulated. The duration of each stimulation was 4 s. At least one picture presentation without stimulation separated each stimulation, and no site was stimulated twice in a row in order to avoid seizures. Each cortical site (size: 5 mm 3 5 mm, due to the spatial resolution of the probe) of the entire cortex exposed by the bone flap was tested three times. Indeed, since the seminal publication of Ojemann et al. (1989), nowadays it is admitted that three tasks are sufficient to be sure whether or not a cortical site is essential for language, e.g. generating speech disturbances during two or three stimulations out of three, with normalization of language as soon as the stimulation is stopped. It is worth noting that this limitation of trials is required by the timing of the surgical procedure; recall that the patient was awake—thus also explaining the need to limit the number of language tasks. The type of language disturbances was detailed by a speech therapist who was always present in the operating room during the functional mapping. Each eloquent area was marked using a sterile number tag on the brain surface, and its location correlated to the anatomical landmarks (sulci/gyri/tumour boundaries) previously identified by ultrasonography. A photograph of the cortical map was systematically made before resection. During a second surgical stage, the glioma was removed, by alternating resection and subcortical stimulations. The functional pathways were followed progressively from the cortical eloquent sites already mapped, to the depth of the resection. The patient had to continue to count or name when the resection became close to the subcortical language structures (including both white matter pathways and deep grey nuclei), which were also identified by language inhibition during stimulation at the cortical level (Skirboll et al., 1996; Duffau et al., 2002, 2003b). In order to perform the best possible tumour removal while sparing functional areas, all resections were pursued until eloquent pathways were encountered around the surgical cavity, then followed according to functional boundaries. Thus, there was no margin left around the cortico-subcortical eloquent areas. Postoperative functional outcome was assessed both during the immediate postoperative stage and 3 months after the surgery. It was performed by the same neurosurgeons and speech therapist who carried out the preoperative functional evaluation, using the same tasks, including the BDAE. A control MRI was performed in all cases, immediately and 3 months after the surgery. This imaging allowed us first to evaluate the quality of glioma removal, and secondly to analyse accurately the anatomical location of the language pathways, i.e. at the periphery of the cavity, where the resection was stopped according to the functional responses eliciting by intraoperative stimulation, a methodology that we used previously (Duffau et al., 2002). Analysis of the intraoperative naming disturbances Naming disorders, which can reflect a weakness of lexical access or loss of the semantic system, may include linguistic deviations called paraphasias. Phonetic paraphasias These affect the articulatory realization from one to several phonemes, by excess or failure of articulatory precision or related to motor difficulties, e.g. simplification of substitution of a phoneme. 799 Phonemic paraphasias These affect the phonological forms of the word. The target word is transformed by substitutions, elision, addition or transposition from one to several phonemes. Generally, the word target remains recognizable but, when errors are very frequent (>50%), one speaks about neologisms which constitutes a phonemic ‘jargon’. Semantic paraphasias These are connected to the meaning of the word target. The word target and the false production in oral meaning belong to the same semantic field. Hence, there are three correlations: the same category of meaning (e.g. orange/lemon), the opposite (e.g. low/high) and usual proximity (e.g. cigarette/lighter). For example, for the word ‘apple’, it can be a hyperonym production such as ‘fruit’ (generic term), a co-hyponym such as ‘peach’ (same category ‘fruit’ but with visual error), hyponym or categorizations such as ‘pippin’, contextual relationships such as ‘tart’, more specific attributes such as ‘pips’ or functional access such as ‘can be eaten’. In the present study, we analysed the patients who experienced transient and reproducible semantic paraphasias during intraoperative electrical stimulation. Although there was usually only one senior speech therapist in the operating room, each error induced by stimulations was also classified intraoperatively by a student in speech therapy and by the neurosurgeon. Moreover, each site, in particular if eliciting language disturbances when stimulated, was systematically tested at least three times, with the presentation of three different objects to name. Thus, the classification of the different types of paraphasic errors became unambiguous, particularly concerning semantic paraphasias, since the word produced by the patient was always perfectly understandable as a ‘real’ word (which is not true for phonetic and/or phonemic paraphasias), but was systematically wrong—while connected to the meaning of the word target, which differed for each new task in order to confirm the exact nature of the disorder. In addition, each error was recorded, then analysed postoperatively by at least two speech therapists: the one present during the surgery and one colleague. Results The clinical, radiological and surgical characteristics of the 17 patients are summarized in Table I. Subjects The series consisted of 11 males and six females, ranging in age from 17 to 52 years (mean 33 years). Fourteen patients were right-handed and three left-handed, as assessed by neuropsychological examination. The presenting symptoms were seizures in the 17 cases (four generalized, 13 partial with transient speech disturbances). The preoperative clinical testing was normal in all patients, in particular without any semantic disturbances on the BDAE. The preoperative MRI showed in all cases a T1-weighted hypointense and T2-weighted hyperintense corticosubcortical lesion, without enhancement after gadolinium injection. 9 2 6 Frontal lobe Insular lobe Temporal lobe 4 M/2 F; 26 (17–43) 2 M; 32 and 33 5 M/4 F; 37 (25–52) Sex and age (years) 4 right-handed/ 1 left-handed No deficit 2 right-handed No deficit 7 right-handed/ 2 left-handed No deficit Preoperative examination Cortical language mapping: semantic sites around the anterior part of the IFS in five patients Subcortical language mapping: semantic pathways under the IFS in all cases Cortical language mapping: no insular cortical semantic sites detected Subcortical language mapping: semantic pathways within the anterior floor of the external capsule Cortical language mapping: semantic sites around the posterior part of the STS in four patients Subcortical language mapping: semantic pathways under STS in all cases Intraoperative electrical mapping semantic paraphasias M = male; F = female; IFS = inferior frontal sulcus; STS = superior temporal sulcus. No. of patients Glioma location Transient semantic disturbances then recovery within 3 months in all cases Transient semantic disturbances then recovery within 3 months in all cases Infero-lateral boundary: IFS Transient semantic disturbances then recovery within 3 months in all cases Infero-mesial boundary: supero-lateral temporal horn of the ventricle Deep boundary: temporal part of the inferior frontooccipital fasciculus Superior boundary: STS Deep boundary: frontal part of the inferior fronto-occipital fasciculus Deep boundary: median part of the inferior frontooccipital fasciculus Postoperative anatomical MRI Postoperative examination Table 1. Clinical, radiological and surgical characteristics of the 17 patients operated on for a low-grade glioma near the inferior fronto-occipital fasciculus (dominant hemisphere) 800 H. Duffau et al. Connectivity of the semantic system Three different groups of tumour locations were found. (i) In six patients, the lesion was located in the dominant temporal lobe (five left and one right lesion), immediately inferior and/or anterior to the posterior part of the superior temporal gyrus: one within the mid-part of the middle temporal gyrus, one within the posterior part of the middle temporal gyrus and four involving the mid- and posterior parts of the middle and inferior temporal gyri, and the fusiform gyrus (three left, one right) (Fig. 1A). (ii) In two patients, the glioma invaded the entire left insular lobe (Fig. 2A). (iii) In the nine other patients, the lesion was located immediately above and/ or medially to the dominant IFC: four lesions within the fronto-mesial structures (superior frontal gyrus, three left and one right glioma), four lesions within the middle frontal gyrus (three left, one right), and one tumour involving both left superior and middle gyri (Fig. 3A). Operative findings Temporal gliomas At the cortical level. In four patients with left tumour, semantic paraphasias were reproducibly elicited by cortical stimulations. These ‘semantic’ sites were located in the four cases around the posterior part of the left superior temporal gyrus, i.e. in the superior temporal gyrus immediately above the superior temporal sulcus in one case, in the middle temporal gyrus immediately below the superior temporal gyrus in one case, and in both gyri in two patients. In these four patients, these language areas constituted the postero-superior functional boundary of the glioma resection (Fig. 1B). In the two other patients, one with a left mid-temporal glioma within the middle temporal gyrus and one with a right glioma, cortical stimulations within the posterior part of the middle temporal gyri (posterior limit of the tumour removal) elicited hesitations/slowness of naming, but without any semantic paraphasia. However, following the opening of the superior temporal gyrus in both patients, during the resection, other stimulations of this buried cortex, at the postero-superior part of the tumour, then elicited semantic paraphasias. At the subcortical level. In the second surgical stage, stimulations of the white subcortical pathways were systematically performed all along the tumour resection, as previously reported (Duffau et al., 2002, 2003b). Interestingly, they induced semantic disturbances in the six patients, in all cases during stimulations of the white bundle located under the superior temporal sulcus, above the temporal horn of the ventricle (opened in four patients). From anterior to posterior, this pathway was identified from the occipito-temporal junction posteriorly (posterior and deep functional boundary of the resection), up to the junction between the anterior temporal third and the mid-temporal third anteriorly, just below the anterior part of the insular cortex, which generated articulatory but not semantic disorders when stimulated (Fig. 1C), as we already observed (Duffau et al., 2000). At this level, it was not possible to continue to follow this pathway, which seemed 801 to run under the anterior insula (antero-superior limit of the resection in the depth). Insular gliomas At the cortical level. There was no language disturbance elicited by the stimulations of the left insular cortex in the two patients, due to the glioma invasion, while language sites were detected within frontal (speech arrest) and temporal opercula (anomia) not invaded by the tumour, as previously described (Duffau et al., 2001). At the subcortical level. Following resection of the anterior part of the insula, stimulations of the deep white fibres, i.e. corresponding to the anterior part of the external capsule (as confirmed by postoperative MRI, see below), reproducibly induced semantic paraphasias in both patients (Fig. 2B). Frontal gliomas At the cortical level. While frontal cortical language sites were identified by stimulation in the nine patients before resection, systematically generating production disorders such as anarthria and/or speech arrest and/or anomia, as we already reported (Duffau et al., 2003c), only five patients presented semantic paraphasia during cortical electrical mapping (four left gliomas, one right). In these five patients, the ‘semantic sites’ were located within the orbito-frontal cortex (i.e. the anterior and inferior part of the inferior frontal gyrus, in front of the sites which generated articulation disturbances when stimulated) or within the DLPFC [i.e. the middle fontal gyrus, in front of the dorsal premotor cortex which elicited anomia during stimulation, as previously described (Duffau et al., 2003c)] (Fig. 3B). It is worth noting that all four patients without any semantic site detected by cortical stimulation harboured a posterior frontal lesion, immediately in front of the precentral gyrus, i.e. within the dorsal premotor cortex (two in the posterior part of the superior frontal gyrusand two in the posterior part of the middle frontal gyrus; three left gliomas, one right). At the subcortical level. As in the two first groups of patients (with temporal and insular lesions), subcortical stimulation reproducibly elicited semantic paraphasia in the nine patients with frontal gliomas. Concerning patients with resection involving the middle frontal gyrus, these semantic disorders were generated by stimulation of the white fibres under the inferior frontal sulcus, above the anterior part of the superior insulo-opercular sulcus, in front of the pathways involved in language production that we previously detailed (Duffau et al., 2002). Concerning patients with resection involving only the superior frontal gyrus, the semantic paraphasias were induced by stimulation of the deep white matter, at the level of the antero-lateral edge of the cavity, laterally and above the anterior part of the head of the caudate nucleus (frontal horn opened in four patients), in front of the fibres coming from 802 H. Duffau et al. A B Skull base P D A Vertex C Skull base P E A Vertex Fig. 1 (A) Preoperative axial and coronal T1-weighted enhanced MRI, showing a low-grade glioma involving the mid- and posterior part of the left temporal lobe: the middle and inferior gyri, and the fusiform gyri. Note, especially on the coronal slice, that despite sparing of the temporo-mesial structures and of the superior temporal cortex, the tumour begins to invade the subcortical white matter between the supero-lateral edge of the temporal horn of the ventricle (below) (curved arrow) and the depth of the superior temporal sulcus (above) (straight arrow). (B) Intraoperative photograph before tumour resection. The eloquent cortical sites identified using electrical stimulations were marked by numbers as follows: 1, primary motor area of the face; 10, ventral premotor cortex inducing anarthria during stimulations; 20, 21, 22, sites within the posterior part of the superior temporal gyrus (20, 21) or the middle temporal gyrus (22) eliciting semantic paraphasia when stimulated; 23, non-reproducible hesitation. The letters correspond to the limits of the tumour identified using intraoperative ultrasonography. Small arrow = superior temporal sulcus; large arrow = posterior part of the sylvian fissure; A = anterior; P = posterior. (C) Intraoperative photograph after tumour resection, showing that the posterior and deep boundaries of the cavity were represented by language cortical sites and subcortical pathways, as follows: 20, 21, 22, cortical semantic sites, which constituted the posterior limit of the resection (the area under 23 was removed because the hesitation was not reproduced during re-stimulations, and because of an invasion of this site by the glioma); 33, 32, 30, 31 (from posterior to anterior), subcortical pathway eliciting reproducible semantic paraphasia when stimulated, running in a postero-anterior direction, located between the depth of the superior temporal sulcus (above) and the temporal horn of the ventricle which was opened (below). Interestingly, this bundle continued anteriorly, by passing under the anterior insular cortex, which was surgically identified then stimulated; it elicited articulation disorders, but no semantic disturbances (29). Examples of semantic paraphasia during electrical mapping: ‘brush’ instead of ‘comb’; ‘zebra’ instead of ‘giraffe’; ‘pan’ instead of ‘ladle’; and ‘sideboard’ instead of ‘dresser’.The patient presented transient postoperative language semantic disturbances, which recovered within 2 months, following speech rehabilitation. (D) Postoperative coronal T1-weighted enhanced MRI (two slices: one posterior, one anterior), showing the resection of the left middle and inferior temporal gyri, and the fusiform gyrus. The boundaries of the cavity were: the superior temporal sulcus (superiorly, with preservation of the superior temporal gyrus) (straight arrow); and the latero-superior part of the horn of the ventricle (inferiorly, with preservation of the amygdalo-hippocampal structures) (curved arrow). Between these two limits, a postero-anterior white bundle runs, which constituted the deep functional boundary of the resection, since it elicited semantic paraphasia when stimulated. This is the reason why a tumoral residue was left at this level (T1 hyposignal, visible on both posterior and anterior slices). (E) Postoperative axial T1-weighted enhanced MRI, showing the deep residual glioma (antero-posterior rim of hyposignal in the depth of the cavity) (arrows), and the similarity of its location within the white matter in comparison with a tractography of the anterior part of the temporo-occipital portion of the inferior fronto-occipital fasciculus; from Catani et al. (2002). Connectivity of the semantic system 803 B A C Fig. 2 (A) Preoperative coronal T1-weighted enhanced MRI, showing a low-grade glioma involving the left insular lobe. Note that the tumour begins to invade the subcortical white matter at the level of the anterior part of the external capsule, since the signal abnormality comes into contact with the lateral part of the lentiform nucleus (arrow). (B) Intraoperative photograph following tumour resection. The eloquent cortical sites identified using electrical stimulations were marked by numbers as follows: 1, 13, speech arrest (Broca’s area); 10, 11, 12, ventral premotor cortex inducing anarthria during stimulations. After opening of the sylvian fissure, because of no identification of the functional site in the insular cortex, the glioma was removed, until eloquent areas were encountered within the white matter in the depth of the cavity: at this level, stimulations elicited semantic paraphasias (tags 2 and 45). A = anterior; P = posterior. The patient presented transient slight postoperative language semantic disturbances, which recovered within 1 month, following speech rehabilitation. (C) Postoperative coronal T1-weighted enhanced MRI, showing partial resection of the left insular glioma. The boundaries of the cavity were superiorly, the subcortical part of Broca’s area, still functional despite its tumoral infiltration (curve arrow); and deeply, the anterior part of the external capsule, eliciting semantic paraphasia when stimulated; this is the reason why a thin rim of tumoral residue was left at this level (T1 hyposignal, straight arrow). the posterior part of the middle frontal gyrus (i.e. the dorsal premotor cortex), eliciting anomia during stimulation (Duffau et al., 2003c) (Fig. 3C). In the 17 patients, cortico-subcortical eloquent structures identified by stimulations were systematically preserved, constituting the functional boundaries of the surgical resection. Independent of the tumour location, the semantic paraphasias elicited most frequently were (i) use of a generic term (‘bird’ for ‘eagle’ or ‘woodpecker’; ‘animal’ for ‘lion’ or ‘tiger’; ‘flower’ for ‘rose’); and (ii) use of a co-hyponym (‘brush’ instead of ‘comb’; ‘horse’ for ‘donkey’; ‘zebra’ instead of ‘giraffe’; ‘pan’ instead of ‘ladle’; ‘sideboard’ instead of ‘dresser’; or ‘Little Red Riding Hood’ for ‘Father Christmas’). Postoperative course Postoperatively, the 17 patients presented transient semantic paraphasias which resolved within 7 days to 3 months, whatever the temporal, insular or frontal location of the tumour. All patients had speech rehabilitation, which allowed a complete functional recovery systematically evaluated using the same BDAE as preoperatively, and showing a normalization of the scores. All patients returned to a normal socioprofessional life. Histological examination revealed a low-grade glioma in all cases. Radiological results In temporal lesions, the cavity came into contact superiorly with the superior temporal sulcus in six patients, up to the depth of this sulcus; and deeply, with the latero-superior part of the temporal horn of the ventricle which was opened (the middle, inferior temporal and fusiform gyri were removed, with preservation of the amygdalo-hippocampal structures since they were not invaded by the tumour). Between these two boundaries runs a postero-anterior white matter fibre bundle that constituted the deep functional boundary 804 H. Duffau et al. A B D C E Fig. 3 (A) Preoperative axial and coronal T1-weighted enhanced MRI, showing a low-grade glioma involving the left fronto-mesial structures. Note that the tumour invades the subcortical white matter up to the antero-superior part of the head of the caudate nucleus (straight arrow). (B) Intraoperative photograph before tumour resection. The eloquent cortical sites identified using electrical stimulations were marked by numbers as follows: 1, 3, primary motor area of the hand; 12, dorsal premotor cortex inducing anomia during stimulations; 10, 11, ventral premotor cortex inducing anarthria during stimulations; 13, speech arrest site, within the pars opercularis; 14, site within the pars orbitaris of the inferior frontal gyrus, eliciting semantic paraphasia when stimulated. The letters correspond to the limits of the tumour identified using intraoperative ultrasonography. Small arrows = precentral gyrus; large arrow = sylvian fissure; curved arrow = inferior frontal sulcus; A = anterior; P = posterior. (C) Intraoperative photograph after tumour resection, showing that the posterior, inferior and deep boundaries of the cavity were represented by language cortical sites and subcortical pathways, as follows: 14, cortical semantic site, which constituted the inferior limit of the resection; 48, subcortical pathway eliciting reproducible semantic paraphasia when stimulated, running under the inferior frontal sulcus with was opened anteriorly (since the anterior part of the middle frontal gyrus was removed in addition to the superior frontal gyrus), and under the inferior frontal gyrus. These fibres run laterally and anteriorly to the head of the caudate nucleus, marked by the tag 46 under the retractor, since the lateral horn of the ventricle was opened (curved arrow). Note that more posteriorly and superiorly to this head of the caudate, subcortical stimulations elicited anomia (tag 47), at the level of pathways corresponding to the cortical site found within the dorsal premotor area (tag 12), thus constituting the postero-lateral boundary of the resection. The patient presented transient postoperative language semantic disturbances with slowness of speech, which recovered within 3 months, following speech rehabilitation. (D) Postoperative axial and coronal T1-weighted enhanced MRI, showing the resection of the left superior frontal gyrus, and the anterior part of the middle frontal gyrus, with opening of the inferior frontal sulcus (axial slice). The subcortical bundle which runs under the depth of this inferior frontal sulcus, in a postero-anterior and infero-superior direction, corresponds to the white fibres which converge in front of and laterally to the head of the caudate nucleus (between the antero-lateral striatum and the anterior part of the superior insulo-opercular sulcus) (curve arrows): this pathway induced semantic paraphasia when stimulated, and thus represented the deep functional boundary of the resection. (E) Postoperative sagittal T1-weighted enhanced MRI, with projection of the surgical cavity (blue line) on a similar MRI view, which visualizes the entire fronto-occipital fasciculus in green using diffusion tensor magnetic resonance tractography (from Catani et al., 2002): such a superimposition shows the similarity of the location of the deep inferior eloquent sites which elicited semantic paraphasias during stimulations (i.e. functional boundaries of the resection) with the tractography of the anterior part of the inferior fronto-occipital fasciculus. Connectivity of the semantic system of the resection, since they corresponded to the subcortical pathways eliciting semantic paraphasia when stimulated: this is the reason why a tumoral residue was left on the entire surface of the deep wall of the cavity in two patients, as shown by the immediate postoperative MRI (abnormal antero-posterior rim of the T1 hyposignal in the depth) (Fig. 1D). Interestingly, this subcortical bundle corresponds to the temporal part of the inferior fronto-occipital fasciculus, with radiations coming from the middle, inferior temporal and fusiform gyri within posterior temporal and occipital cortex, then running medially in the temporal lobe and continuing antero-superiorly to the frontal lobe via the anterior floor of the external capsule under the insular lobe (Crosby et al., 1962; Nieuwenhuys et al., 1988; Gloor, 1997; Catani et al., 2002), as shown by a comparison between the residual tumour on postoperative MRI and a similar MRI slice with delineation of the posterior part of this fronto-occipital fasciculus using diffusion tensor imaging (DTI) tractography (from Catani et al., 2002) (Fig. 1E). In insular lesions, the (anterior) deep boundary of the cavity was the anterior part of the external capsule, since it also elicited semantic paraphasias during electrical stimulation. Postoperative MRI showed the preservation of the white pathways running at the junction of the temporal and frontal lobes, i.e. at the level where the fibres of the inferior frontooccipital fasciculus compact and pass through the anterior floor of the external capsule (no claustrum was still visible at depth) (Fig. 2C). In frontal gliomas, the infero-lateral limits of the cavity were by the infero-lateral and dorso-lateral frontal cortex and their corresponding white fibres, which converged in front of and laterally to the head of the caudate nucleus, in order to run posteriorly under the anterior insula. This point of convergence constituted the deep inferior and lateral boudary of the resection, since white fibres at this level induced semantic paraphasia when stimulated (Fig. 3D): they correspond to the frontal part of the inferior fronto-occipital fasciculus, as shown by the projection of the surgical cavity on a similar MRI view with visualization of the entire frontooccipital fasciculus using DTI (from Catani et al., 2002) (Fig. 3E). Discussion The results of the present study appears to provide new insights into the anatomo-functional connectivity of the semantic network. Cortical organization of the semantic system Numerous lesion, stimulation and neuroimaging works have allowed a better understanding of the cortical organization of the semantic system that is based on two essential ‘epicentres’: the dominant posterior temporal areas and the IFC/DLPFC. 805 Posterior temporal areas As mentioned in the Introduction, implication of left posterior temporal areas in semantic processing is supported by neurofunctional imaging (Wise et al., 1991; Bookheimer et al., 1998; Tyler et al., 2003), lesion studies in aphasic patients (Hart and Gordon, 1990; Mummery et al., 1999; Saygin et al., 2003), as well as reports of cortical stimulation (Lüders et al., 1991; Boatman et al., 2000; Ilmberger et al., 2001; Hamberger et al., 2003; Gatignol et al., 2004). Interestingly, in our study, electrical stimulation identified cortical sites involved in semantic processing in four patients with a temporal glioma. In all four cases, sites were located around the posterior part of the left superior temporal sulcus, i.e. in the superior temporal gyrus immediately above it (one case), or in the middle temporal gyrus immediately below it (one case), or both (two cases). Thus, our intraoperative results support data recently provided by functional neuroimaging. The lack of detection of a cortical ‘semantic area’ in two cases could be explained first by the fact that, due to the location of the lesions within the mid-part of the temporal lobe in the two patients (one left, one right), the cortical exposure has not been sufficient posteriorly to map the semantic cortical sites. Secondly, since the ‘epicentre’ for comprehension seems to be represented by the superior temporal sulcus, according to neurofunctional imaging studies, we can consider that a major part of this cortex is not accessible to a cortical electrical stimulation before resection, due to the fact that this semantic cortex is buried within the sulcus, and not located at the surface of the brain. This hypothesis was verified in the two patients in which the lesion came in contact with the superior temporal sulcus. In these case, the sulcus was opened in order to perform the tumour resection, and stimulation of the buried cortex then elicited semantic paraphasias. IFC Numerous lesion (Alexander et al., 1989; Otsuki et al., 1998), stimulation (Schäffler et al., 1993, 1996; Devlin et al., 2003) and neuroimaging (Poldrack et al., 1999; Bookheimer, 2002) studies have supported the notion that there are separate subsystems within the IFG responsible for different aspects of language: phonological, syntactic and semantic processing. As detailed in the Introduction, it would seem that phonological (Poldrack et al., 1999) and syntactic (Embick et al., 2000) regions (particularly recruited in cases of syntactic complexity) (Stromswold et al., 1994; Just et al., 1996; Caplan et al., 1998) are centred around the posterior superior IFG at the border of BA 44 and BA 6, both mutually interactive (Keller et al., 2001). Conversely, semantic areas cluster around the antero-inferior IFG (BA 47) (Noppeney and Price, 2002), the pars triangularis (BA 45) (Friederici et al., 2000b) and the DLPFC (BA 46) (mid-part of the middle frontal gyrus) (Noesselt et al., 2003). BA 45/46/47 appear important for executive aspects of semantic processing that 806 H. Duffau et al. involve semantic working memory, directing semantic search or drawing comparisons between semantic concepts in working memory (Bookheimer, 2002). This region seems to be both modality and content independent. In our experience, we identified cortical sites involved in semantic processing in five patients using electrical stimulations. Interestingly, in the five cases, these ‘semantic sites’ were located within the infero-lateral frontal cortex (i.e. the anterior and inferior part of the inferior frontal gyrus, in front of the sites which generated production disorders when stimulated) or within the dorso-lateral prefrontal cortex (i.e. the middle frontal gyrus, in front of the dorsal premotor cortex which elicited anomia when stimulated). Thus, our intraoperative results support the data recently provided by functional neuroimaging. However, the lack of induction of semantic disorders during frontal mapping in the other four patients could be explained by the fact that all harboured a posterior frontal lesion, immediately in front of the precentral gyrus and thus within the dorsal premotor cortex (three left, one right). Consequently, it is likely that the cortical exposure has not been sufficient antero-laterally (i.e. at the level of the IFC and/or the lateral prefrontal cortex) to map the semantic cortical areas. Therefore, we elicited only anomia or dysarthria during stimulations of the premotor cortex, as previously reported (Duffau et al., 2003c). Moreover, similar to the temporal epicentre, it is possible that at least a part of the cortex implicated in the semantic processing was buried within the sulci, and thus not accessible to the stimulation before resection (Rutten et al., 1999). Subcortical anatomo-functional connectivity of the semantic system Despite recent improvement of our understanding of the intra-cortical organization of semantic processing, little is currently known concerning the anatomo-functional connectivity of this system. This can be explained by the fact that functional neuroimaging methods (PET, fMRI and MEG) up until recently have been unable to study the white matter bundles. Due to the recent development of DTI, it now becomes possible to track non-invasively in vivo the subcortical fibres (Conturo et al., 1999; Jones et al., 1999; Basser et al., 2000). An excellent illustration is given by the work of Catani et al. (2002), who defined in healthy volunteers the main white pathways of the brain. However, studies using DTI are currently limited only to the identification of the anatomy of the bundles, i.e. they allow the direct study of the anatomical connectivity but they do not allow the direct study of the functional connectivity. Conversely, the recent use of computational algorithms applied to quantities on types of functional imaging data that vary in spatial, temporal and other features have permitted the study of functional connectivity (Horwitz et al., 1998; Newman et al., 2002). Nevertheless, these methods are not able simultaneously to provide information regarding anatomical connectivity. Consequently, despite the first experience with fusion of these complementary methods, Horwitz (2003) mentions in a recent review concerning brain connectivity, that ‘until it is understood what each definition means in terms of an underlying neural substrate, comparisons of functional and/or effective connectivity across studies may appear inconsistent and should be performed with great caution’. The use of intraoperative cortical and subcortical electrical stimulation currently gives a unique opportunity to study directly both the anatomical and functional connectivity at the same time, as previously described (Duffau et al., 2002, 2003a,b). Indeed, in spite of the invasive feature of this method, direct brain stimulation offers the advantage of identifying with accuracy and reliability the corticosubcortical structures essential for language (and not only those involved in this function), by eliciting language disturbances when these areas are stimulated (Ojemann et al., 1989; Berger, 1996; Duffau et al., 2002, 2003a). Thus, it is possible to perform an on-line evaluation of the functional consequences of each focal stimulation on awake patients (i.e. to analyse precisely the type of language disturbances transitorily induced), and to correlate each eloquent site to its exact anatomical location on the postoperative MRI—since the edges of the surgical cavity are the functional pathways, due to the fact that the resection was systematically stopped according to functional boundaries. This anatomo-functional study can help to determine different eloquent subregions within a wider area. Although all our patients had structural lesions, language disorders only occurred when stimulating at specific electrode positions. In addition, motor responses to stimulation had a distribution (hand/finger superior, face/ mouth inferior) appropriate for primary motor cortex, systematically found at least in patients operated on for a frontal lesion—since the bone flap did not expose the whole central region in cases of temporal tumours. Consequently, these findings strongly suggest that our observations accurately reflect the functional anatomy of the regions tested, particularly at the subcortical level, where brain plasticity phenomena induced by tumour growth seem less than at the cortical level (Duffau et al., 2003d ). Note, nevertheless, that subcortical mapping is time consuming, and thus there is a limitation on the number of (language) tasks which can be performed by the awake patient during the surgical procedure. Interestingly, using this method, we were able to identify subcortical sites eliciting semantic disorders when stimulated, both within the temporal lobe and near the IFC. Temporal lobe In the six cases of intraoperative mapping of the dominant temporal lobe, semantic disturbances were systematically induced during stimulations of the white matter located under the superior temporal sulcus. Due to the fact that the removed lesions involved the mid- and posterior parts of the temporal lobe, it was possible to detect several subcortical Connectivity of the semantic system sites eliciting semantic errors, from the occipito-temporal junction posteriorly to the junction between the anterior temporal third and the mid-temporal third anteriorly (approximately below the anterior part of the insula). Thus, we could hypothesize that we have identified several sites of the same bundle, running in a longitudinal direction under the superior temporal sulcus, with an inferior limit just above the temporal horn of the ventricle (since this ventricle was opened without inducing any language disorders in four patients), and a superior limit under the superior temporal gyrus. Such a white bundle implicated in the semantic network would seem in accordance with the literature about the locations of the cortical sites involved in semantic processing (discussed above), i.e. concordant with a possible convergence of fibres coming from the posterior temporal regions (basal infero-temporal area, posterior part of the middle and superior gyri) and from the mid-part of the superior temporal gyrus, in particular concerning its cortex buried within the temporal superior sulcus. IFC While no patient in this series had a lesion directly involving the IFC, all patients harboured a frontal tumour coming into contact with the ‘semantic pathways’, since in the nine patients, subcortical stimulations generated semantic paraphasias. In the patient with a glioma invading the middle frontal gyrus, the semantic disorders were elicited by the stimulations of the white fibres under the inferior frontal sulcus, above the anterior part of the superior insulo-opercular sulcus, in front of the pathways involved in speech production. In the patients with a fronto-mesial glioma, the semantic disturbances were systematically generated by the stimulation of the white matter at the level of the antero-infero-lateral edge of the cavity, laterally and in front of the anterior part of the head of the caudate nucleus (frontal horn opened in found patients), and thus in front of the fibres coming from the posterior part of the middle frontal gyrus (the dorsal premotor cortex, inducing anomia when stimulated). The locations of these subcortical ‘semantic sites’ are in accordance with the current literature regarding the cortical organization of the semantic system, since all these sites were situated around the IFC, at the level of the superior (medial) and anterior deep boundaries of the DLPFC and pars orbitaris, i.e. converging laterally and in front of the head of the caudate nucleus, and running to the anterior portion of the external capsule, under the anterior part of the insular lobe. Indeed, in the two patients operated on for an insular lowgrade glioma, while there was no language site detected at the surface of this lobe using electrical mapping, despite the contribution of this structure to motor aspects of speech (Duffau et al., 2000; Ackermann and Riecker, 2004), probably due to cortical functional reshaping induced by the glioma (Duffau et al., 2001), semantic paraphasias were reproducibly elicited during stimulation of the anterior floor of the external capsule, at the end of the resection. 807 In summary, our results provide arguments in favour of the existence of a main pathway underlying the semantic system, within the left or right dominant hemisphere, and joining the two essential epicentres of this network: the posterior and superior temporal areas and the IFC/DLPFC. Interestingly, anatomical studies (Crosby et al., 1962; Nieuwenhuys et al., 1988; Gloor, 1997) and more recent DTI studies (Catani et al., 2002) identified a bundle which connects infero-lateral and dorso-lateral frontal cortices with the posterior temporal cortex and the occipital lobe: the inferior fronto-occipital fasciculus. This fasciculus runs posteriorly from mainly prefrontal cortical areas immediately superior to the uncinate in the frontal lobe. At the junction of the frontal and temporal lobes, the fasciculus narrows in section as it passes through the anterior floor of the external capsule. As the uncinate hooks away anteromedially, the inferior fronto-occipital fasciculus continues posteriorly before running medially in the temporal lobe above and internal to the lateral ventricle, and radiating to the occipital lobe. These radiations terminate in the middle and inferior temporal gyri and in the lingual and fusiform gyri. Due to the concordance between the anatomy of this fasciculus and the semantic pathway defined using intraoperative subcortical stimulation in our study, we suggest that the inferior fronto-occipital fasciculus might constitute the anatomic support for what could be called the ‘semantic loop’. Indeed, this bundle allows the connection between two essential epicentres of the semantic network, i.e. the IFC/DLPFC and the temporal posterior regions within the dominant hemisphere, known to work together in comprehension (Mesulam, 1990; Papathanassiou et al., 2000; Davis and Johnsrude, 2003; Friederici et al., 2003; Heim et al., 2003a), with likely interactive top-down and bottom-up modulation (Tomita et al., 1999; Noesselt et al., 2003). However, it is important to note that in addition to the inferior fronto-occipital fasciculus, primate anatomical studies have indicated at least one other tract in the temporal lobe, connecting mid-temporal and frontal regions (Petrides and Pandya, 1988). Consequently, it is possible that this bundle may also participate in subserving semantic processing. Further studies combining intraoperative subcortical stimulations and perioperative DTI are thus mandatory, in order to take a multiple pathway view underlying semantic networks. Conclusions On the basis of our findings, we can hypothesize the existence of a dual route in language connectivity: (i) a ventral semantic stream, connecting the IFC/DLPFC and the posterior temporal regions, via the inferior fronto-occipital fasciculus (6other fronto-temporal tracts); and (ii) a dorsal phonological stream, connecting the IFC/ventral premotor cortex (Duffau et al., 2003c) and the supramarginalis gyrus/posterosuperior temporal cortex, via cortico-cortical connections (Duffau et al., 2003a) and the arcuate fasciculus (Duffau et al., 2002). 808 H. Duffau et al. Interestingly, this model is in accordance with the diagram recently proposed by Gold and Buckner (2002), showing common prefrontal regions co-activated with dissociable posterior regions during controlled semantic (posterior middle temporal gyrus) and phonological (supramarginalis gyrus) tasks. Such an organization of the anatomo-functional connectivity might support the hypothesis put forward by TzourioMazoyer (2003), which consists of applying the hierarchical perception/action sensorimotor model of Fuster (1998) to the organization of language, on the basis of the classification of the cortical architecture suggested by Mesulam (1985) at three levels: processing and production of language sounds via the primary auditive and motor areas; a phonological network including the superior temporal areas and the IFC/ ventral premotor cortex (unimodal associative areas); and a semantic network constituted by the posterior part of the superior temporal sulcus and pars triangularis and orbitaris of IFC (multimodal associative areas). Finally, a better knowledge of the anatomo-functional organization of these distributed subnetworks of language may have important implications concerning the planning of brain surgery of lesions involving these structures. Acknowledgements We wish to thank Bernard Mazoyer for helpful comments on the manuscript. References Ackermann H, Riecker A. The contribution of the insula to motor aspects of speech production: a review and a hypothesis. Brain Lang 2004; 89: 320–8. Alexander MP, Benson DF, Stuss DT. Frontal lobes and language. Brain Lang 1989; 37: 656–91. Baddeley A. Working memory. Science 1992; 255: 556–9. Baddeley A. Working memory: looking back and looking forward. Nat Rev Neurosci 2003; 4: 829–39. Basser P, Pajevic S, Pierpaoli C, Duda J, Aldroubi A. In vivo fiber tracking using DT-MRI data. Magn Reson Med 2000; 44: 625–32. Berger MS. Minimalism through intraoperative functional mapping. Clin Neurosurg 1996; 43: 324–37. Boatman D, Gordon B, Hart J, Selnes O, Miglioretti D, Lenz F. Transcortical sensory aphasia: revisited and revised. Brain 2000; 123: 1634–42. Bookheimer S. Functional MRI of language: new approaches to understanding the cortical organization of semantic processing. Annu Rev Neurosci 2002; 25: 151–88. Bookheimer SY, Zeffiro TA, Blaxton TA, Gaillard WD, Malow B, Theodore WH. Regional cerebral blood flow during auditory responsive naming: evidence for cross-modality neural activation. Neuroreport 1998; 9: 2409–13. Booth JR, Burman DD, Meyer JR, Gitelman DR, Parrish TB, Mesulam M. Modality independence of word comprehension. Hum Brain Mapp 2002; 16: 251–61. Brugge JF, Volkov IO, Garell PC, Reale RA, Howard MA III. Functional connections between auditory cortex on Heschl’s gyrus and on the lateral superior temporal gyrus in humans. J Neurophysiol 2003; 90: 3750–63. Caplan D, Alpert N, Waters G. Effects of syntactic structure and propositional number on patterns of regional cerebral blood flow. J Cogn Neurosci 1998; 10: 541–52. Catani M, Howard RJ, Pajevic S, Jones DK. Virtual in vivo interactive dissection of white matter fasciculi in the human brain. NeuroImage 2002; 17: 77–94. Chee MW, O’Craven KM, Bergida R, Rosen BR, Savoy RL. Auditory and visual word processing studied with fMRI. Hum Brain Mapp 1998; 7: 15–28. Conturo TE, Lori NF, Cull TS, Akbudak E, Snyder AZ, Shimony JS, et al. Tracking neuronal fiber pathways in the living human brain. Proc Natl Acad Sci USA 1999; 96: 10422–7. Crinion JT, Lambon-Ralph MA, Warburton EA, Howard D, Wise RSJ. Temporal lobe regions engaged during normal speech comprehension. Brain 2003; 126: 1193–201. Crosby EC, Humphrey T, Lauer EW. Correlative anatomy of the nervous system. New York: Macmillian; 1962. Damasio H, Grabowski TJ, Tranel D, Hichwa RD, Damasio AR. A neural basis for lexical retrieval. Nature 1996; 380: 499–505. Dapretto M, Bookheimer SY. Form and content: dissociating syntax and semantics in semantic comprehension. Neuron 1999; 24: 427–32. Davis MH, Johnsrude IS. Hierarchical processing in spoken language comprehension. J Neurosci 2003; 23: 3423–31. Decety J, Chaminade T, Grezes J, Meltzoff AN. A PET exploration of the neural mechanisms involved in reciprocal imitation. Neuroimage 2002; 15: 265–72. Demb J, Desmond J, Wagner A, Vaidya C, Glover G, Gabrieli J. Semantic encoding and retrieval in the left inferior prefrontal cortex: a functional MRI study of task difficulty and process specificity. J Neurosci 1995; 15: 5870–8. Démonet JF, Chollet F, Ramsay S, Cardebat D, Nespoulos JL, Wise R, et al. The anatomy of phonological and semantic processing in normal subjects. Brain 1992; 115: 1753–68. Desmond JE, Sum JM, Wagner AD, Demb JB, Shear PK, Glover GH, et al. Functional MRI measurement of language lateralization in Wada-tested patients. Brain 1995; 118: 1411–9. Devlin JT, Matthews PM, Rushworth MFS. Semantic processing in the left inferior prefrontal cortex: a combined functional magnetic resonance imaging and transcranial magnetic stimulation study. J Cogn Neurosci 2003; 15: 71–84. Duffau H, Capelle L, Lopes M, Faillot T, Sichez JP, Fohanno D. The insular lobe: physiopathological and surgical considerations. Neurosurgery 2000; 47: 801–11. Duffau H, Bauchet L, Lehéricy S, Capelle L. Functional compensation of the left insula dominant for language. Neuroreport 2001; 12: 2159–63. Duffau H, Capelle L, Sichez N, Denvil D, Lopes M, Sichez JP, et al. Intraoperative mapping of the subcortical language pathways using direct stimulations. An anatomo-functional study. Brain 2002; 125: 199–214. Duffau H, Gatignol P, Denvil D, Lopes M, Capelle L. The articulatory loop: study of the subcortical connectivity by electrostimulation. Neuroreport. 2003a; 14: 2005–8. Duffau H, Capelle L, Denvil D, Sichez N, Gatignol P, Taillandier L, et al. Usefulness of intraoperative electrical subcortical mapping during surgery for low-grade gliomas located within eloquent brain regions: functional results in a consecutive series of 103 patients. J Neurosurg. 2003b; 98: 764–78. Duffau H, Capelle L, Denvil D, Gatignol P, Sichez N, Lopes M, et al. The role of dominant premotor cortex in language: a study using intraoperative functional mapping in awake patients. Neuroimage 2003c; 20: 1903–14. Duffau H, Capelle L, Denvil D, Sichez N, Gatignol P, Lopes M, et al. Functional recovery after surgical resection of low grade gliomas in eloquent brain: hypothesis of brain compensation. J Neurol Neurosurg Psychiatry 2003d; 74: 901–7. Embick D, Marantz A, Miyashita Y, O’Neil W, Sakai KL. A syntactic specialization for Broca’s area. Proc Natl Acad Sci USA 2000; 97: 6150–54. Fiez J. Phonology, semantics, and the role of the left inferior prefrontal cortex. Hum Brain Mapp 1997; 5: 79–83. Fiez JA, Petersen SE. Neuroimaging studies of word reading. Proc Natl Acad Sci USA 1998; 95: 914–21. Connectivity of the semantic system Friederici AD, Opitz B, von Cramon DY. Segregating semantic and syntactic aspects of processing in the human brain: an fMRI investigation of different word types. Cereb Cortex 2000a; 10: 698–705. Friederici AD, Meyer M, von Cramon DY. Auditory language comprehension: an event-related fMRI study on the processing of syntactic and lexical information. Brain Lang 2000b; 74: 289–300. Friederici AD, Rüschemeyer SA, Hahne A, Fiebach CJ. The role of left inferior frontal and superior temporal cortex in sentence comprehension: localizing syntactic and semantic processes. Cereb Cortex 2003; 13: 170–177. Fuster JM. Linkage at the top. Neuron 1998; 21: 1223–4. Gabrieli JDE, Desmond JE, Demb JB, Wagner AD. Functional magnetic resonance imaging of semantic memory processes in the frontal lobes. Psychol Sci 1996; 7: 278–83. Gabrieli JDE, Poldrack RA, Desmond JE. The role of left prefrontal cortex in language and memory. Proc Natl Acad Sci USA 1998; 95: 906–13. Gatignol P, Capelle L, Le Bihan R, Duffau H. Double dissociation between picture naming and comprehension: an electrostimulation study. Neuroreport 2004; 15: 191–5. Gloor P. The temporal lobe and the limbic system. New York: Oxford University Press; 1997. Gold BT, Buckner RL. Common prefrontal regions coactivate with dissociable posterior regions during controlled semantic and phonological tasks. Neuron 2002; 35: 803–12. Goodglass H, Kaplan E. The assessment of aphasia and related disorders. Philadelphia: Lea and Fibiger; 1972. Hamberger MJ, Seidel WT, Goodman RR, Perrine K, McKhann GM. Temporal lobe stimulation reveals anatomic distinction between auditory and naming processes. Neurology 2003; 60: 1478–83. Hart J Jr, Gordon B. Delineation of single-word semantic comprehension deficits in aphasia, with anatomical correlations. Ann Neurol 1990; 27: 226–31. Heim S, Opitz B, Friederici AD. Broca’s area in the human brain is involved in the selection of grammatical gender for language production: evidence from event-related functional magnetic resonance imaging. Neurosci Lett 2002; 328: 101–4. Heim S, Opitz B, Friederici AD. Distributed cortical networks for syntax processing: Broca’s area as the common denominator. Brain Lang 2003a; 85: 402–8. Heim S, Opitz B, Müller K, Friederici AD. Phonological processing during language production: fMRI evidence for a shared production– comprehension network. Cogn Brain Res 2003b; 16: 285–96. Homae F, Hashimoto R, Nakajima K, Miyashita Y, Sakai KL. From perception to sentence comprehension: the convergence of auditory and visual information in the left inferior frontal cortex. Neuroimage 2002; 16: 883–900. Horwitz B. The elusive concept of brain connectivity. Neuroimage 2003; 19: 466–70. Horwitz B, Rumsey JM, Donohue BC. Functional connectivity of the angular gyrus in normal reading and dyslexia. Proc Natl Acad Sci USA 1998; 95: 8939–44. Ilmberger J, Eisner W, Schmid U, Reulen HJ. Performance in picture naming and word comprehension: evidence for common neuronal substrates from intraoperative language mapping. Brain Lang 2001; 76: 111–118. Jobard G, Crivello F, Tzourio-Mazoyer N. Evaluation of the dual route theory of reading: a metanalysis of 35 neuroimaging studies. Neuroimage 2003; 20: 693–712. Jones DK, Simmons A, Williams SCR, Horsfield MA. Non-invasive assessment of axonal fiber connectivity in the human brain via diffusion tensor MRI. Magn Reson Med 1999; 42: 37–41. Just MA, Carpenter PA, Keller TA, Eddy WF, Thulborn KR. Brain activation modulated by sentence comprehension. Science 1996; 274: 114–16. Kang A, Constable R, Gore J, Avrutin S. An event-related fMRI study of implicit phrase level syntactic and semantic processing. Neuroimage 1999; 10: 555–61. 809 Kapur S, Rose R, Liddle PF, Zipursky RB, Brown GM, Stuss D, et al. The role of the left prefrontal cortex in verbal processing: semantic processing or willed action? Neuroreport 1994; 5: 2193–6. Keller T, Carpenter P, Just MA. The neural bases of sentence comprehension: an fMRI examination of syntactic and lexical processing. Cereb Cortex 2001; 11: 223–37. Lehéricy S, Cohen L, Bazin B, Samson S, Giacomini E, Rougetet R, et al. Functional MR evaluation of temporal and frontal language dominance compared with the Wada test. Neurology 2000; 54: 1625–33. Lüders H, Lesser RP, Hahn J, Dinner DS, Morris HH, Wyllie E, Godoy J. Basal temporal language area. Brain 1991; 114: 743–54. Mazoyer B, Dehaene S, Tzourio N, Frak V, Cohen L, Murayama N, et al. The cortical representation of speech. J Cog Neurosci 1993; 5: 467–79. Mesulam MM. Principles of behavioral neurology. Philadelphie: F.A. Davis; 1985. Mesulam MM. Large-scale neurocognitive networks and distributed processing for attention, language and memory. Ann Neurol 1990; 28: 597–613. Metz-Lutz MN, Kremin H, Deloche G, Hannequin D, Ferrand L, Perrier D, et al. Standardisation d’un test de dénomination orale: contrôle des effets de l’âge, du sexe et du niveau de scolarité chez les sujets adultes normaux. Rev Neuropsychol 1991; 1: 73–95. Michael EB, Keller TA, Carpenter PA, Just MA. FMRI investigation of sentence comprehension by eye and by ear: modality fingerprints on cognitive processes. Hum Brain Mapp 2001; 13: 239–52. Moro A, Tettamanti M, Perani D, Donati C, Cappa SF, Fazio F. Syntax and the brain: disentangling grammar by selective anomalies. Neuroimage 2001; 13: 110–8. Müller RA, Rothermel RD, Behen ME, Muzik O, Mangner TJ, Chakraborty PK, et al. Receptive and expressive language activations for sentences: a PET study. Neuroreport 1997; 8: 3767–70. Mummery CJ, Ashburner J, Scott SK, Wise RJ. Functional neuroimaging of speech perception in six normal and two aphasic subjects. J Acoust Soc Am 1999; 106: 449–57. Nieuwenhuys R, Voogd J, van Huijen C. The human central nervous system. Berlin: Springer-Verlag; 1988. Newman SD, Just MA, Carpenter PA. The synchronization of the human cortical working memory network. Neuroimage 2002; 15: 810–22. Nobre AC, Allison T, McCarthy G. Word recognition in the human inferior temporal lobe. Nature 1994; 372: 260–3. Noesselt T, Jon Shah N, Jäncke L. Top-down and bottom-up modulation of language related areas—an fMRI study. BMS Neurosci 2003; 4:13. Noppeney U, Price CJ. A PET study of stimulus- and task-induced semantic processing. Neuroimage 2002; 15: 927–35. Ojemann GA, Ojemann JG, Lettich E, Berger MS. Cortical language localization in left, dominant hemisphere. An electrical stimulation mapping investigation in 117 patients. J Neurosurg 1989; 71: 316–26. Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 1971; 9: 97–113. Otsuki M, Soma Y, Koyama A, Yoshimura N, Furukawa H, Tsuji S. Transcortical sensory aphasia following left frontal infarction. J Neurol 1998; 245: 69–76. Papathanassiou D, Etard O, Mellet E, Zago L, Mazoyer B, TzourioMazoyer N. A common language network for comprehension and production: a contribution to the definition of language epicenters with PET. Neuroimage 2000; 11: 347–57. Paulesu E, Frith CD, Frackowiak RSJ. The neural correlates of the verbal component of working memory. Nature 1993; 362: 342–5. Petrides M, Pandya DN. Association fiber pathways to the frontal cortex from the superior temporal region in the Rhesus monkey. J Comp Neurol 1988; 273: 52–66. Poldrack RA, Wagner AD, Prull MW, Desmond JE, Glover GH, Gabrieli JD. Functional specialization for semantic and phonological processing in the left inferior prefrontal cortex. Neuroimage 1999; 10: 15–35. Price CJ. The anatomy of language: contributions from functional neuroimaging. J Anat 2000; 3: 335–59. 810 H. Duffau et al. Rutten GJ, van Rijen PC, van Veelen CW, Ramsey NF. Language area localization with three-dimensional functional magnetic resonance imaging matches intrasulcal electrostimulation in Broca’s area. Ann Neurol 1999; 46: 405–8. Saygin AP, Dick F, Wilson W, Dronkers F, Bates E. Neural resources for processing language and environmental sounds: evidence from aphasia. Brain 2003; 126: 928–45. Schäffler L, Luders HO, Dinner DS, Lesser RP, Chelune GJ. Comprehension deficits elicited by electrical stimulation of Broca’s area. Brain. 1993; 116: 695–715. Schäffler L, Lüders HO, Beck GJ. Quantitative comparison of language deficits produced by extraoperative electrical stimulation of Broca’s, Wernicke’s, and basal temporal language areas. Epilepsia 1996; 37: 463–75. Schlosser MJ, Aoyagi N, Fulbright RK, Gore JC, McCarthy G. Functional MRI studies of auditory comprehension. Hum Brain Mapp 1998; 6: 1–13. Scott SK, Blank CC, Rosen S, Wise RJ. Identification of a pathway for intelligible speech in the left temporal lobe. Brain 2000; 123: 2400–6. Skirboll SS, Ojemann GA, Berger MS, Lettich E, Winn R. Functional cortex and subcortical white matter located within gliomas. Neurosurgery 1996; 38: 678–85. Stromswold K, Caplan D, Alpert N, Rauch S. Localization of syntactic comprehension by positron emission tomography. Brain Lang 1996; 52: 452–73. Szatkowska I, Grabowska A, Szymanska O. Phonological and semantic fluencies are mediated by different regions of the prefrontal cortex. Acta Neurobiol Exp (Wars) 2000; 60: 503–8. Thompson-Schill SL, D’Esposito M, Aguirre GK, Farah MJ. Role of left inferior prefrontal cortex in retrieval of semantic knowledge: a reevaluation. Proc Natl Acad Sci USA 1997; 94: 14792–7. Thompson-Schill SL, Swick D, Farah MJ, D’Esposito M, Kan IP, Knight RT. Verb generation in patients with focal lesion lesions: a neuropsychological test of neuroimaging findings. Proc Natl Acad Sci USA 1998; 95: 15855–60. Tomita H, Ohbayashi M, Nakahara K, Hasegawa I, Miyashita Y. Top-down signal from prefrontal cortex in executive control of memory retrieval. Nature 1999; 401: 699–703. Tulving E, Kapur S, Markowitsch HJ, Craik FIM, Habib R, Houle S. Neuroanatomical correlates of retrieval in episodic memory: auditory sentence recognition. Proc Natl Acad Sci USA 1994; 91: 2012–5. Tyler LK, Stamatakis EA, Dick E, Bright P, Fletcher P, Moss H. Objects and their actions: evidence for a neurally distributed semantic system. Neuroimage 2003; 18: 542–57. Tzourio-Mazoyer N. Les réseaux neuraux dédiés au langage chez l’adulte. In: Etard O, Tzourio-Mazoyer N, editors. Traité des sciences cognitives: cerveau et langage. Paris: Hermes; 2003. p. 67–101. Wagner A, Desmond J, Demb J, Glover G, Gabrieli JD. Semantic repetition priming for verbal and pictorial knowledge. J Cogn Neurosci 1997; 9: 714–26. Wagner AD, Pare-Blagoev EJ, Clark J, Poldrack RA. Recovering meaning: left prefrontal cortex guides controlled semantic retrieval. Neuron 2001; 31: 329–38. Warburton E, Wise RJ, Price CJ, Weiller C, Hadar U, Ramsay S, et al. Noun and verb retrieval by normal subjects. Studies with PET. Brain 1996; 119: 159–79. Wise R, Chollet F, Hadar U, Friston K, Hoffner E, Frackowiak R. Distribution of cortical networks involved in word comprehension and word retrieval. Brain 1991; 114: 1803–18. Wise R, Scott S, Blamk S, Mummery C, Murphy K, Warburton E. Separate neural subsystems within ‘Wernicke’s area’. Brain 2001; 124: 83–95. Zatorre RJ, Evans AE, Meyer E, Gjedde A. Lateralization of phonetic and pitch discrimination in speech processing. Science 1992; 256: 846–7.