Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
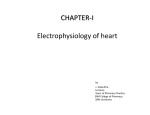
Interdependence of Modulated Dispersion and Tissue Structure in the Mechanism of Unidirectional Block Kenneth R. Laurita, David S. Rosenbaum Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 Abstract—We previously showed that a premature stimulus can significantly alter vulnerability to arrhythmias by modulating spatial gradients of ventricular repolarization (ie, modulated dispersion). However, it is not clear if such changes in arrhythmia vulnerability can be attributed to the formation of an electrophysiological substrate for unidirectional block and what the potential role is of tissue structure in this process. Therefore, the main objective of the present study was to examine the concomitant effect repolarization gradients and tissue structure have on unidirectional block. Optical action potentials were recorded from 128 ventricular sites (1 cm2) in 8 Langendorffperfused guinea pig hearts. Propagation was confined to the epicardial surface using an endocardial cryoablation procedure, and a 12-mm barrier with a 1.5-mm isthmus was etched with a laser onto the epicardium. A premature stimulus (S2) was delivered over a range of S1S2 coupling intervals to modulate repolarization gradients in a predictable fashion. When a second premature stimulus (S3) was delivered from the center of the isthmus, the occurrence and orientation of unidirectional block were highly dependent on repolarization gradients created by the S2 beat. In this model, a local repolarization gradient of 3.2 ms/mm was required for unidirectional block at this isthmus. In addition, the formation of unidirectional block was critically dependent on the presence of the source-sink mismatch imposed by the isthmus. These results may explain how the interplay between spatial heterogeneities of repolarization and tissue structure form a substrate for unidirectional block and reentry. (Circ Res. 2000;87:922-928.) Key Words: optical mapping 䡲 source-sink mismatch 䡲 repolarization 䡲 reentry 䡲 premature stimulation W e previously found that intrinsic properties of cellular repolarization vary systematically between cells across the epicardial surface of the guinea pig heart despite the presence of normal cell-to-cell coupling.1 From this work and other studies,2– 4 it is abundantly apparent that repolarization properties vary extensively throughout the heart. However, the implication such diversity has on the formation of arrhythmogenic substrates in the heart is not well appreciated. Early studies have established a close association between heterogeneity of repolarization and cardiac arrhythmogenesis.5– 8 Furthermore, we have shown that vulnerability to arrhythmias is significantly influenced by spatial gradients of repolarization that form, disappear, and reform on the epicardial surface during premature stimulation in a coupling interval– dependent manner (ie, modulated dispersion).9 However, the mechanism underlying such dynamic formation of the arrhythmogenic substrate was not clear. It is also well recognized that impulse propagation is highly dependent on the structural arrangement of tissue10,11 and wavefront geometry.12,13 For example, tissue branching14 and propagation through a narrow isthmus15 can create an abrupt change in electrical load, resulting in an imbalance between the current available upstream and the actual current required to excite cells downstream (ie, source-sink mis- match). The source-sink mismatch imposed by an isthmus or abrupt tissue expansion has been shown, in experimental models and theoretical studies, to significantly influence the safety factor of propagation11,12,16 and the initiation of reentrant excitation.17 It is clear that such source-sink mismatches play an important role in impulse propagation. However, what is less clear is the relative importance functional heterogeneity of repolarization properties between cells and source-sink mismatch have in the formation of unidirectional block, a fundamental requirement of reentrant excitation. This question has important implications to the mechanisms of arrhythmias in the atria10,18 and ventricle,19,20 where discontinuities of tissue structure caused by valvular orifices, muscle bundles, veins, arteries, and scar tissue are known to coexist with regional heterogeneities of cellular ionic properties. The main objective of the present study was to investigate the relative importance of dynamically modulated repolarization gradients and the source-sink mismatch imposed by a fixed isthmus in the determination of unidirectional block. Because of limitations of conventional recording techniques, it is difficult to track the dynamic changes in spatial gradients of repolarization and their direct effect on the electrophysiological substrate for reentry. Therefore, high-resolution action Received August 21, 2000; revision received September 7, 2000; accepted September 7, 2000. From the Heart and Vascular Research Center, MetroHealth Campus, Case Western Reserve University, Cleveland, Ohio. Correspondence to Kenneth R. Laurita, PhD, MetroHealth Campus, Case Western Reserve University, 2500 MetroHealth Dr, Rammelkamp, 6th floor, Cleveland, Ohio 44109-1998. E-mail [email protected] © 2000 American Heart Association, Inc. Circulation Research is available at http://www.circresaha.org 922 Laurita et al Mechanisms of Unidirectional Block 923 potential mapping with voltage-sensitive dye was used to measure spatial gradients of cellular repolarization and the propagation of an extrastimulus in the wake of such gradients. The mechanism of unidirectional block could not be explained by repolarization gradients or source-sink mismatch alone but was critically dependent on both influences. Materials and Methods Experimental Preparation Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 All experiments were carried out in accordance with Public Health Service guidelines for the care and use of laboratory animals. Guinea pigs (n⫽8) were anesthetized (30 mg/kg pentobarbital, IP), and their hearts were rapidly excised and perfused as Langendorff preparations (perfusion pressure 70 mm Hg) with oxygenated (95% O2, 5% CO2) Tyrode’s solution containing (mmol/L) NaCl 130, NaHCO3 25, MgSO4 1.2, KCl 4.75, dextrose 5, and CaCl2 1.25 (pH 7.4, 31°C to 33°C). The right and left atria were excised to avoid competitive simulation from the SA node and to provide access to the ventricles for the cryoablation procedure (see below). Hearts were stained with voltage-sensitive dye di-4-ANEPPS (10 mol/L) by direct coronary perfusion for 10 minutes. Beating and perfused hearts were immersed in a Tyrode-filled custom-built Lexan chamber. Gentle pressure was applied with a movable piston to the posterior surface of the heart during action potential recordings, allowing the heart to contract freely except for within the mapping field. Because gentle pressure may cause transient ischemia, recordings were brief and action potentials were continually monitored for signs of ischemia (eg, triangulated action potentials). If ischemia was evident, the experiment was not included in the analysis. Cardiac rhythm was monitored using 3 silver disk electrodes fixed to the chamber in positions corresponding to ECG limb leads I, II, and III. The ECG signals were filtered (0.3 to 300 Hz), amplified (1000⫻), and displayed on a digital recorder (WINDOGRAF, Gould Inc). The optical mapping system used in this study has been described in detail elsewhere.1,21,22 In the present study, an optical magnification of 1.8⫻ was used, corresponding to a mapping field of 1⫻1 cm and 0.08 cm spatial resolution between recording pixels. Experimental Protocol To confine propagation to the epicardial surface and avoid the confounding influence of subepicardial breakthrough from the HisPurkinje system, the endocardial muscle layers were eliminated using a cryoablation procedure described previously.22 To create a source-sink mismatch, a linear barrier containing a 1.5-mm isthmus was etched precisely (⫾1 m) onto the epicardial surface (n⫽5) using a 5W argon ion laser guided by computer controlled micropositioners (Figure 1).22 The width of the isthmus was based on findings by Cabo et al,12 who demonstrated that isthmus widths between 1.3 and 2 mm were sufficient to cause unidirectional block in ventricular myocardium. Software provided the ability to preprogram the position and size of barriers, ensuring reproducibility between experiments. The barrier extended in depth to the endocardial cryoablation zone to create a line of anatomical block that was parallel to and 2 mm to the right of the left anterior descending coronary artery on the anterior free wall of the left ventricle. In addition, the position of the barrier was perpendicular to the orientation of repolarization typically found in guinea pig.1 In 3 additional control hearts, no barrier was created. Baseline pacing (S1S1⫽600 ms) and a single premature stimulus (S2) were delivered at 2⫻ diastolic threshold using a Teflon-coated silver bipolar electrode (DTU 101, Bloom Associates LTD) from the same site near the base of the left ventricle corresponding to the basal end of the laser barrier, when present (Figure 1). The location of S1S2 stimulation was carefully chosen with respect to the barrier to reduce the possibility of unequal conduction delays on either side of the isthmus. Four different S1S2 coupling intervals were tested in each experiment, decrementing from a coupling interval equal to the baseline pacing cycle length down to a short coupling interval just Figure 1. Diagram of the mapping field (1 cm2) and its position relative to the intact heart. RV indicates right ventricle; LV, left ventricle. The S3 impulse was always delivered just beyond the effective refractory period of the S2 beat from the center of an isthmus (S3) within a linear anatomical barrier (arrows). In hearts without a barrier, the site of S3 stimulation was from the center of the mapping field. Baseline pacing (S1) and the first premature stimulus (S2) were always delivered from the same site (S1S2) near the base of the LV. White squares indicate the 2 regions from which the local repolarization gradient was calculated. above the refractory period of the S1 beat. For each S1S2 coupling interval tested, a second premature stimulus (S3) was delivered at 2⫻ diastolic threshold from the center of the isthmus (or from the center of the mapping field in the absence of a barrier) using a Teflon-coated silver unipolar electrode (0.1 mm diameter) connected to a second stimulator (DCI-1114, Digital Cardiovascular Instruments Inc). The S3 stimulus was always delivered just above the effective refractory period (⬍2 ms) of the S2 beat. Data Analysis In all experiments and for each S1S2 coupling interval tested, automated algorithms were used to determine depolarization time and repolarization time relative to a single fiducial point (ie, the stimulus).9 Repolarization time was defined as the maximum positive curvature (maximum positive second derivative) during repolarization23 and corresponds to ⬇95% repolarization24 (ie, APD95%). To quantify the local gradient of repolarization surrounding the isthmus, the average repolarization times from 2 regions (3⫻3 pixels), each immediately adjacent to either side of the isthmus without overlapping the barrier, were subtracted and divided by the center-to-center distance between each region (⬇2 to 3 mm). Shown in Figure 1 are the 2 regions chosen (white squares) from a representative experiment. The direction of the local repolarization gradient was defined as either positive (left ventricle apex to right ventricle base repolarization sequence) or negative (right ventricle base to left ventricle apex repolarization sequence). Local repolarization gradients were determined for all coupling intervals tested. Successful propagation was defined as cell-to-cell impulse propagation occurring across at least 3 recording sites. Results Modulated Dispersion After a Premature Stimulus Shown in Figure 2 is a representative example of depolarization and repolarization during premature stimulation in the 924 Circulation Research November 10, 2000 during baseline pacing became earliest during the short premature coupling interval and vice versa. Shown in the Table are summary data of the local repolarization gradient at baseline pacing and for premature stimuli delivered at an intermediate and short coupling interval for every experiment with a barrier. In hearts without a barrier (ie, control), repolarization gradients were modulated in a similar fashion, as previously reported.1 Modulated Dispersion and Unidirectional Block Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 Figure 2. Contour maps of depolarization (top) and repolarization (bottom) during a premature stimulus delivered at a coupling interval equal to the baseline pacing cycle length (A), at an intermediate coupling interval (B), and at a short coupling interval near the effective refractory period (C). All values shown are in ms unless otherwise indicated. Local repolarization gradient near the isthmus within the linear barrier (black rectangles) was calculated for each S1S2 coupling interval tested. presence of a barrier. For an S1S2 coupling interval equal to the baseline drive train (Figure 2A), the impulse initiated by S2 propagated simultaneously down either side of the barrier. Significant gradients of action potential duration were present across the epicardial surface (not shown), as evidenced by gradients of repolarization orientated perpendicular to the direction of depolarization and the barrier. A premature stimulus introduced at an intermediate coupling interval (Figure 2B) produced no significant change in the pattern of depolarization compared with baseline pacing. However, repolarization gradients were substantially reduced, resulting in a local repolarization gradient of 0 ms/mm near the isthmus. When a premature stimulus was introduced at a short coupling interval near refractoriness (Figure 2C), the overall pattern of depolarization was unchanged. In contrast, repolarization gradients reappeared and were reversed in direction compared with baseline; ie, where repolarization was latest To determine if coupling interval– dependent changes in repolarization determine the occurrence of unidirectional block, we examined the characteristics of propagation of an S3 stimulus delivered from the center of an isthmus in the wake of repolarization gradients established by an S2 beat. Shown in Figure 3 are data from a representative experiment where S1S2 coupling interval was shortened from 600 ms to 225 ms. The contour maps across the top show the pattern of repolarization surrounding the isthmus after each S2 beat. Shown below each repolarization map is a contour map demonstrating depolarization of an S3 beat in the wake of repolarization gradients established by each S2 beat. For an S1S2 coupling interval equal to the baseline cycle length (Figure 3A), a gradient of repolarization is present that delays repolarization on the left side of the isthmus. An S3 impulse delivered in the wake of this repolarization pattern failed to propagate to the left side of the isthmus in the direction of the repolarization gradient. However, propagation (velocity⫽0.44⫾0.11 m/sec) was successful to the right (ie, unidirectional block) and continued around both ends of the barrier in a pattern like figure-of-eight reentry. This is also reflected in the action potentials shown at the bottom of Figure 3 that were recorded from equally spaced sites perpendicular to the barrier. Propagation failed in the direction of site a but was successful in the direction of site b, continuing around, much later, to site a. Thus, during baseline pacing, the electrophysiological requirements for unidirectional block were present. An S3 stimulus was again introduced from the same location in the same heart, but in this case after a shorter (ie, Influence of Premature Coupling Interval on the Local Repolarization Gradient and on Unidirectional Block Coupling Interval, ms Local Repolarization Gradient, ms/mm Unidirectional Block Experiment No. BASE INTER SHORT BASE INTER SHORT BASE INTER SHORT 1 600 270 160 ⫹5.6 ⫹1.6 ⫺8.5 ⫹ None ⫺ 2 600 300 225 ⫹7.5 ⫺3.7 ⫺12.1 ⫹ None ⫺ ⫺ 3 600 270 230 ⫹14.0 ⫺0.1 ⫺3.2 ⫹ None 4 600 290 220 ⫹9.3 ⫹2.0 ⫺5.9 ⫹ None ⫺ 5 600 230 200 ⫹7.1 ⫹1.4 ⫺3.6 ⫹ None ⫺ 8.7⫾3.2 1.8⫾1.3 6.7⫾3.7 Mean⫾SD Summary of experimental data demonstrating the effect of premature stimulation coupling interval on the local repolarization gradient and the occurrence of unidirectional block in the presence of a lesion. Shown are results for baseline stimulation (BASE), premature stimulation at an intermediate coupling interval when repolarization gradients were minimum (INTER), and premature stimulation at a short coupling interval near refractoriness (SHORT). The absolute value of the local repolarization gradient was used to determine the mean response. The direction of unidirectional block is either toward the right ventricular base perpendicular to the barrier (positive, ⫹) or toward the left ventricular apex perpendicular to the barrier (negative, ⫺). Laurita et al Mechanisms of Unidirectional Block 925 Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 Figure 3. Unidirectional block of an S3 impulse (S3) delivered from the center of an isthmus within a linear barrier (white rectangles). Three different premature coupling intervals were tested: baseline pacing (A) (600 ms), an intermediate coupling interval (B) (300 ms), and a short coupling interval (C) (225 ms). Contour maps on top show the pattern of repolarization of the S2 beat surrounding the isthmus. Contour maps in the middle show propagation of the S3 beat in the wake of repolarization gradients established by the S2 beat. Shown at the bottom are action potentials of the S3 beat recorded from equally spaced sites perpendicular to the barrier. The S3 stimulus was always introduced just beyond the effective refractory period of the S2 beat. intermediate) S1S2 coupling interval (Figure 3B). It is evident that after this premature stimulus, gradients of repolarization were greatly attenuated, and repolarization was nearly simultaneous on both sides of the isthmus. Under these circumstances, propagation after the S3 stimulus never blocked unidirectionally, but either propagated successfully (velocity⫽0.39⫾0.12 m/sec) in both directions (Figure 3B) or failed to capture the tissue at all (not shown). Thus, at an intermediate coupling interval, the electrophysiological requirements for unidirectional block were eliminated because of eradication of repolarization gradients. Finally, at a short S1S2 coupling interval (Figure 3C), the repolarization gradient is restored to a similar magnitude as that seen during baseline pacing; however, the orientation of the gradient is reversed. In this case, the S3 impulse failed to propagate to the right side of the barrier but successfully propagated (0.45⫾0.10 m/sec) to the left and continued around both ends of the barrier, meeting on the other side of the isthmus. Thus, at a short S1S2 coupling interval, the electrophysiological requirements for unidirectional block were restored; however, at this coupling interval, unidirectional block occurred on the opposite side of the isthmus, following the direction of the repolarization gradient. Shown in the Table are the occurrence and direction of block as a function of S1S2 coupling interval and local repolarization gradient. In the absence of a barrier, unidirectional block was observed only once for all coupling intervals tested (n⫽12, not shown). Reentrant beats after the S3 stimulus were observed in 3 of 5 experiments performed with a barrier and in no experiment when an isthmus was absent (ie, control). Shown in Figure 4 are examples of ECGs and action potentials recorded during premature stimulation, the formation of unidirectional block, and during multiple reentrant beats in 3 separate experiments. The activation sequence, determined from all 128 action potential recordings made during each episodes (not shown), indicates that unidirectional block of the S3 impulse initiated reentrant excitation. Requirements for Unidirectional Block When pacing from the center of the isthmus, the likelihood of unidirectional block was highly dependent on the magnitude and direction of the local repolarization gradient surrounding the isthmus. Shown in Figure 5 are summary data for all Figure 4. Shown is the ECG (top) and 1 optically recorded ventricular transmembrane potential (bottom) measured during the initiation of several reentrant beats after premature stimulation in 3 different experiments. For each example, the last 2 beats of drive train pacing (S1) and the first premature stimulus (S2) followed by the onset of several spontaneous beats are shown. 926 Circulation Research November 10, 2000 Figure 5. Association between the local repolarization gradient and the formation of unidirectional block in the presence of a barrier. Unidirectional block occurred when local repolarization gradients were ⬎3.2 ms/mm. Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 experiments indicating the local repolarization gradient (ms/ mm) that was associated with the formation (right) or lack of formation (left) of unidirectional block on either side of the isthmus. Local repolarization gradients for all S1S2 coupling intervals tested are shown. When pacing from the center of the isthmus, unidirectional block was induced 14 times out of 20 coupling intervals tested. In each of the 14 cases of unidirectional block, a local repolarization gradient ⬎3.2 ms/mm was present. However, block did not occur when the repolarization gradient was ⬍3.7 ms/mm (n⫽5). Thus, in this model there seems to be a distinct repolarization gradient threshold that is required for unidirectional block. In contrast, in the absence of a barrier over the same range of S1S2 coupling intervals tested (ie, control hearts), unidirectional block of the S3 beat was observed only once for 12 coupling intervals tested despite the presence of repolarization gradients (3.8⫾1.3 m/sec) ⬎3.2 ms/mm. Therefore, the sourcesink mismatch created by the isthmus seems to play a significantly important role in the formation of unidirectional block (2, P⬍0.005). To test the relative importance of tissue structure and repolarization gradients on the occurrence of unidirectional block, in 2 experiments the S3 stimulus electrode was moved from the center of the isthmus to one side, at the basal entrance to the isthmus. In this configuration, the repolarization gradient is unchanged; however, the source-sink mismatch is no longer equal on both sides of the isthmus. On the basal side of the isthmus, the source-sink mismatch is absent, and on the apical side, it is present as the impulse propagates through the isthmus. Shown in Figure 6 is a representative example where a sufficiently large repolarization gradient (panel A) resulted in unidirectional block of the S3 beat when pacing from the center of the isthmus (panel B). The contour map demonstrates successful propagation to the apical side of the barrier, where repolarization was earliest (arrows), and propagation failure to the basal side of the barrier, where repolarization was latest. When the S3 stimulus was moved from the center of the isthmus to the basal entrance of the isthmus (panel C), propagation was successful toward the base of the heart, against the repolarization gradient (arrows). However, propagation failed toward the apex of the heart, in the direction of the source-sink mismatch. Therefore, in this configuration unidirectional block formed as a result of the source-sink mismatch imposed by the isthmus, not the local gradient of repolarization. These results additionally demonstrate that repolarization gradients, even in the presence of a barrier, are not sufficient to create block unless a source-sink mismatch is present. Discussion In this study, we report a potentially important mechanism for the initiation of reentrant excitation on the basis of the direct effect a premature stimulus has on modulating the electrophysiological substrate for reentry. We found that the electrophysiological requirements for unidirectional block were modulated in a coupling interval– dependent manner by pacing-induced modulation of repolarization gradients. Such changes in the formation of unidirectional block may underlie the mechanism of arrhythmia vulnerability associated with modulated dispersion, as we have shown previously.9 In addition, our results suggest that the source-sink mismatch imposed by tissue structure also plays a critically important role in the occurrence of unidirectional block. Modulated Dispersion and Arrhythmia Vulnerability We previously showed that a premature stimulus can systematically modulate spatial gradients of action potential duration and repolarization in a coupling interval– dependent manner, which was explained on the basis of heterogeneities of repolarization kinetics between ventricular cells.1 In the present study we have shown a similar response in the presence of a barrier, where repolarization gradients were modulated in a systematic fashion perpendicular to the barrier (Figure 2). Even though the modulated dispersion response, Figure 6. Shown is the influence tissue structure has on the formation of unidirectional block. When pacing from the center of the isthmus (B), block occurred in the direction of the repolarization gradient where repolarization was latest (A). When pacing from the basal entrance to the isthmus (C), the direction of block reversed and occurred as the impulse propagated through the isthmus, toward the apex of the heart. Laurita et al Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 in general, was not altered in the presence of a barrier, we did observe repolarization gradients that were greater in magnitude compared with control. This might be attributable to an insulating effect of the barrier that reveals intrinsic regional ionic properties. Nevertheless, in control hearts the local repolarization gradient (3.8⫾1.3 ms/mm) generally failed to produce unidirectional block, whereas comparable gradients (6.4⫾4.2 ms/mm) did cause unidirectional block in the presence of an isthmus. The results of the pullback experiment (Figure 6) provide additional evidence that the sourcesink mismatch created by the isthmus is critically important, even if larger repolarization gradients are present because of the barrier. In this experiment, the insulating effect of the barrier is present, but the source-sink mismatch is absent on one side of the isthmus. In this case, despite the larger repolarization gradient in the presence of the barrier, block only occurred in the direction of the source-sink mismatch (Figure 6C). Therefore, even though the barrier creates slightly larger gradients of repolarization, it is the source-sink mismatch that seems to play a more important role. The fact that large repolarization gradients could not be achieved in the absence of a barrier is expected, because hearts are not normally prone to arrhythmias. However, it is possible to attain very large repolarization gradients and unidirectional block without a barrier, such as those seen during discordant repolarization alternans.25 We found that stimulus-induced changes in repolarization gradients directly influenced the electrophysiological requirements for unidirectional block. As S1S2 coupling interval was shortened to an intermediate value, dispersion of repolarization decreased such that unidirectional block of a second premature beat was much less likely to occur. Additional shortening of S1S2 coupling interval to a value just longer than the effective refractory period markedly increased repolarization gradients, which, in-turn, restored the conditions necessary for the development of unidirectional block. We previously found that vulnerability to ventricular fibrillation is also influenced in a coupling interval– dependent fashion,9 where vulnerability decreased at intermediate coupling intervals when repolarization gradients were minimal. It is possible that such changes in vulnerability to fibrillation were a direct result of changes in the requirements for unidirectional block. Taken together, these data provide compelling evidence that in normal hearts a premature stimulus can significantly modulate the electrophysiological substrate for reentry. Combined Role of Repolarization Gradients and Tissue Structure in the Formation of Unidirectional Block In this study, we designed an experimental system that allowed us to investigate the direct relationship between repolarization gradients, a source-sink mismatch imposed by an isthmus, and the formation of unidirectional block. In a series of control experiments, we found that in hearts without a barrier, unidirectional block of a second premature (S3) beat was rarely observed despite the presence of significant repolarization gradients generated by the S2 stimulus. Similarly, we found that the source-sink mismatch created when Mechanisms of Unidirectional Block 927 stimulating from the center of an isthmus was not sufficient to produce unidirectional block unless a significant repolarization gradient (ie, ⬎3.2 ms/mm) was present. Previously, it was shown that abrupt tissue expansion during propagation through an isthmus12 or at sites of tissue branching10,16 are sufficient to cause slow conduction or block. For example, Cabo et al12 showed that in the setting of uniform reduced excitability, an isthmus width ⬍1.14 mm caused block. This is comparable with our results, where an isthmus of 1.5 mm did not create block in the presence of uniform reduced excitability. We found that when pacing from the center of the isthmus, unidirectional block could only be achieved when the local repolarization gradient was ⬎3.2 ms/mm. These data suggest a critically important interplay between repolarization gradients and tissue structure in the formation of unidirectional block. When the site of S3 stimulation was moved from the center of the isthmus to the entrance of the isthmus, an unequal source-sink mismatch was created (Figure 6). In this situation, we found that unidirectional block occurred in the direction of the source-sink mismatch, opposite to the direction of the repolarization gradient. Therefore, moving the S3 stimulus location must have increased the source-sink mismatch such that a repolarization gradient was not required to obtain block. It is also possible that the lack of a source-sink mismatch on the side of the pacing site made propagation safer, thereby increasing the repolarization gradient required for block. Indeed, this may be the case, because in the absence of a source-sink mismatch (ie, in hearts without an isthmus), block was rarely observed despite the presence of significant repolarization gradients. In either case, these data suggest that a source-sink mismatch can be an overriding determinant of unidirectional block. These findings highlight the important interplay between tissue structure and repolarization heterogeneities that, in conjunction, define the electrophysiological substrate for reentrant arrhythmias. On the basis of these and other12 results, one would predict that in situations where very large repolarization gradients are present, such as in long-QT syndrome,26 only minimal or no structural elements are required to form a substrate for block, whereas in the presence of marked structures discontinuities in tissue, the development of even small gradients of repolarization can contribute significantly to the substrate for reentry. Other studies have shown that both repolarization heterogeneities and tissue structure can play an important role in the initiation of reentrant excitation.17,27,28 In particular, Spach et al27 showed in atrial tissue how repolarization heterogeneities interact with anisotropic conduction and discontinuities of axial resistance at muscle bundle junctions to produce delayed conduction and unidirectional block, respectively. Implications The geometrical characteristics of this experimental model may be analogous to several clinical situations where structural discontinuities in myocardial tissue exist, such as those imposed by a healing myocardial infarct,29 surgical suture lines,30 accessory pathways,31 and the complex structure of atrial endocardial tissue.10,18,32 In particular, the isthmus lo- 928 Circulation Research November 10, 2000 Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 cated between the tricuspid annulus and the eustachian ridge, anterior to the inferior vena cava, has been shown to play a critically important role in the initiation and maintenance of atrial flutter.33 The occurrence of slow conduction and block at the isthmus34 may be explained by the interplay between tissue structure and heterogeneities of refractoriness. Such source-sink mismatches imposed by propagation through an isthmus may not necessarily result from distinct anatomical structures but may also form during reentry. For example, during figure-of-eight reentry, a central common pathway is formed where propagation through an isthmus is associated with spontaneous termination.19 Our results are not necessarily limited to source-sink mismatches imposed by an isthmus but can be extrapolated to other forms of source-sink mismatch, such as that associated with wave front curvature.12,13,22 Additional studies are required to determine how such source-sink mismatches interact with heterogeneities of repolarization and influence the initiation and maintenance of reentrant excitation. Acknowledgments This work was supported by the Medical Research Service of the Department of Veterans Affairs, National Institutes of Health (grant HL54807), Whitaker Foundation, and American Heart Association. References 1. Laurita KR, Girouard SD, Rosenbaum DS. Modulation of ventricular repolarization by a premature stimulus: role of epicardial dispersion of repolarization kinetics demonstrated by optical mapping of the intact guinea pig heart. Circ Res. 1996;79:493–503. 2. Litovsky SH, Antzelevitch C. Transient outward current prominent in canine ventricular epicardium but not endocardium. Circ Res. 1988;62: 116 –126. 3. Fedida D, Giles WR. Regional variations in action potentials and transient outward current in myocytes isolated from rabbit left ventricle. J Physiol (Lond). 1991;442:191–209. 4. Sicouri S, Antzelevitch C. A subpopulation of cells with unique electrophysiological properties in the deep subepicardium of the canine ventricle: the M cell. Circ Res. 1991;68:1729 –1741. 5. Mines GR. On dynamic equilibrium in the heart. J Physiol (Lond). 1913;46:349 –383. 6. Allessie A, Bonke FI, Schopman FJG. Circus movement in rabbit atrial muscle as a mechanism of tachycardia: the role of nonuniform recovery of excitability in the occurrence of unidirectional block as studied with multiple microelectrodes. Circ Res. 1976;39:169 –177. 7. Han J, Moe G. Nonuniform recovery of excitability in ventricular muscle. Circ Res. 1964;14:44 – 60. 8. Gough W, Mehra R, Restivo M, Zeiler R, El-Sherif N. Reentrant ventricular arrhythmias in the late myocardial infarction period in the dog, 13: correlation of activation and refractory maps. Circ Res. 1985;57: 432– 442. 9. Laurita KR, Girouard SD, Akar FG, Rosenbaum DS. Modulated dispersion explains changes in arrhythmia vulnerability during premature stimulation of the heart. Circulation. 1998;98:2774 –2780. 10. Spach MS, Miller WT, Dolber PC, Kootsey JM, Sommer JR, Mosher CE. The functional role of structural complexities in the propagation of depolarization in atrium of the dog: cardiac conduction disturbances due to discontinuities of effective axial resistivity. Circ Res. 1982;50: 175–191. 11. Fast VG, Kléber AG. Cardiac tissue geometry as a determinant of unidirectional conduction block: assessment of microscopic excitation spread by optical mapping in patterned cell cultures and in a computer model. Cardiovasc Res. 1995;29:697–707. 12. Cabo C, Pertsov AM, Baxter WT, Davidenko JM, Gray RA, Jalife J. Wave-front curvature as a cause of slow conduction and block in isolated cardiac muscle. Circ Res. 1994;75:1014 –1028. 13. Fast VG, Kléber AG. Role of wavefront curvature in propagation of cardiac impulse. Cardiovasc Res. 1997;33:258 –271. 14. Mendez C, Mueller WJ, Urguiaga X. Propagation of impulses across the Purkinje fiber-muscle junctions in the dog heart. Circ Res. 1970;26: 135–150. 15. de la Fuente D, Sasyniuk B, Moe GK. Conduction through a narrow isthmus in isolated canine atrial tissue: a model of the W-P-W syndrome. Circulation. 1971;44:803– 809. 16. Kucera JP, Kléber AG, Rohr S. Slow conduction in cardiac tissue, II: effects of branching tissue geometry. Circ Res. 1998;83:795– 805. 17. Quan W, Rudy Y. Unidirectional block and reentry of cardiac excitation: a model study. Circ Res. 1990;66:367–382. 18. Gray RA, Pertsov AM, Jalife J. Incomplete reentry and epicardial breakthrough patterns during atrial fibrillation in the sheep heart. Circulation. 1996;94:2649 –2661. 19. Schmitt H, Wit AL, Coromilas J, Waldecker B. Mechanisms for spontaneous termination of monomorphic, sustained ventricular tachycardia: results of activation mapping of reentrant circuits in the epicardial border zone of subacute canine infarcts. J Am Coll Cardiol. 1998;31:460 – 472. 20. Antzelevitch C, Nesterenko VV, Yan G-X. Role of M cells in acquired long QT syndrome, U waves, and torsade de pointes. J Electrocardiol. 1996;28(suppl):131–138. 21. Girouard SD, Laurita KR, Rosenbaum DS. Unique properties of cardiac action potentials recorded with voltage-sensitive dyes. J Cardiovasc Electrophysiol. 1996;7:1024 –1038. 22. Girouard SD, Pastore JM, Laurita KR, Gregory KW, Rosenbaum DS. Optical mapping in a new guinea pig model of ventricular tachycardia reveals mechanisms for multiple wavelengths in a single reentrant circuit. Circulation. 1996;93:603– 613. 23. Rosenbaum DS, Kaplan DT, Kanai A, Jackson L, Garan H, Cohen RJ, Salama G. Repolarization inhomogeneities in ventricular myocardium change dynamically with abrupt cycle length shortening. Circulation. 1991;84:1333–1345. 24. Efimov IR, Huang DT, Rendt JM, Salama G. Optical mapping of repolarization and refractoriness from intact hearts. Circulation. 1994;90: 1469 –1480. 25. Pastore JM, Girouard SD, Laurita KR, Akar FG, Rosenbaum DS. Mechanism linking T-wave alternans to the genesis of cardiac fibrillation. Circulation. 1999;99:1385–1394. 26. Shimizu W, Antzelevitch C. Sodium channel block with mexiletine is effective in reducing dispersion of repolarization and preventing torsade de pointes in LQT2 and LQT3 models of the long-QT syndrome. Circulation. 1997;96:2038 –2047. 27. Spach MS, Dolber PC, Heidlage JF. Interaction of inhomogeneities of repolarization with anisotropic propagation in dog atria: a mechanism for both preventing and initiating reentry. Circ Res. 1989;65:1612–1631. 28. Brugada J, Boersma L, Kirchhof C, Heynen V, Allessie M. Reentrant excitation around a fixed obstacle in uniform anisotropic ventricular myocardium. Circulation. 1991;84:1296 –1306. 29. Ursell P, Gardner P, Albala A, Fenoglio J, Wit A. Structural and electrophysiological changes in the epicardial border zone of canine myocardial infarcts during infarct healing. Circ Res. 1985;56:436 – 451. 30. Gandhi SK, Bromberg BI, Rodefeld MD, Schuessler RB, Boineau JP, Cox JL, Huddleston CB. Lateral tunnel suture line variation reduces atrial flutter after the modified Fontan operation. Ann Thorac Surg. 1996;61: 1299 –1309. 31. Kuck K, Friday KJ, Kunze K, Schluter M, Lazzara R, Jackman WM. Sites of conduction block in accessory atrioventricular pathways. Circulation. 1990;82:407– 417. 32. Olgin JE, Kalman JM, Lesh MD. Conduction barriers in human atrial flutter: correlation of electrophysiology and anatomy. J Cardiovasc Electrophysiol. 1996;7:1112–1126. 33. Feld GK, Fleck RP, Chen P-S, Boyce K, Bahnson TD, Stein JB, Calisi CM, Ibarra M. Radiofrequency catheter ablation for the treatment of human type 1 atrial flutter: identification of a critical zone in the reentrant circuit by endocardial mapping techniques. Circulation. 1992;86: 1233–1240. 34. Olgin JE, Kalman JM, Saxon LA, Lee RJ, Lesh MD. Mechanism of initiation of atrial flutter in humans: site of unidirectional block and direction of rotation. J Am Coll Cardiol. 1997;29:376 –384. Interdependence of Modulated Dispersion and Tissue Structure in the Mechanism of Unidirectional Block Kenneth R. Laurita and David S. Rosenbaum Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 Circ Res. 2000;87:922-928 doi: 10.1161/01.RES.87.10.922 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2000 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/87/10/922 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/