Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
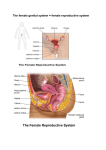
A Guide to Hysteroscopy Patient Education QUESTIONS AND ANSWERS ABOUT HYSTEROSCOPY Your doctor has recommended that you have a procedure called a hysteroscopy. Naturally, you may have questions about how and why the procedure is done, what to expect, and how much risk and discomfort it may involve. This brochure will help to answer many of the questions and concerns you might have about hysteroscopy. G L O S S A RY Benign: Noncancerous. Cervix: The portion of the uterus that extends out into the cavity of the vagina. Dilation and curettage (D&C): Temporary widening of the cervix and scraping of the endothelium (inner lining of the uterus) in order to diagnose diseases, treat abnormal vaginal bleeding, or remove the products of contraception. Endometrium: The lining of the uterus. Fallopian tubes: The tubes through which the ovum (egg) is carried to the uterus. Fibroid (myoma): A benign tumor of the uterus. Foley catheter: A hollow, flexible rubber tube usually used to drain the bladder after surgery. Hysterectomy: Surgical removal of the uterus. Hysteroscope: A thin, telescopic instrument that allows doctors to examine the uterus and fallopian tubes and perform some types of surgery. Infertility: The inability to conceive. Intrauterine adhesion: A band of scar tissue within the lining of the uterus. Intrauterine device (IUD): A reversible contraception device that is inserted into the uterine cavity. Polyp: A benign growth that projects from a mucous membrane surface, such as the lining of the uterus. Uterine septum: A condition, present at birth, in which there is an extra fold of tissue down the center of the uterus, which may cause infertility. Uterus: The woman’s internal reproductive organ, sometimes referred to as the “womb.” 2 Questions and Answers About Hysteroscopy What is a hysteroscopy? Hysteroscopy is a technique that allows a doctor to look directly into your cervical canal and uterus. It is typically done during the first week or so after your period. A thin, telescopic instrument called a hysteroscope is inserted into the uterus through the cervix, allowing the doctor to examine the interior shape and lining of your uterus and fallopian tubes. The purpose is to look for any evidence of abnormalities or disease and to decide which approach to take for treatment. Fallopian Tubes Uterus Ovary Cervix Why perform a hysteroscopy? The most common reason for performing a hysteroscopy is to determine the cause of heavy or abnormal vaginal bleeding. Your doctor can also look for the underlying causes of infertility (the inability to conceive a child) or repeated miscarriages. Hysteroscopy can uncover and sometimes immediately treat many types of irregularities, most of which are benign (noncancerous) in nature, including: Questions and Answers About Hysteroscopy 3 Submucous Myoma Polyp • Fibroids (myomas)—firm, benign growths of the uterus that can be found in an estimated 30 percent of women over the age of 35. Women with large fibroids are at greater risk for abnormal uterine bleeding and miscarriages. Fibroids can also cause pain and abdominal pressure. • Polyps—soft growths that project from mucous membrane surfaces, such as the lining of the cervix and the endometrium (the lining of the uterus). They are usually benign and may cause abnormal uterine bleeding. • Uterine septum—an extra fold of tissue down the center of the uterus, present from birth and associated with infertility and miscarriages. Septum • Intrauterine adhesions—bands of scar tissue between the walls of the uterus. They may cause amenorrhea (the absence of normal menstrual periods) and infertility. • Blocking of the fallopian tubes—a condition that may cause infertility. Repairing these obstructions may increase your chances of becoming pregnant. What are the benefits of hysteroscopy? Hysteroscopies can be performed quickly and conveniently in the doctor’s office, surgical center, or hospital. Diagnostic hysteroscopy only takes a few minutes, and you can go home shortly after the procedure. Even when an operative procedure is performed, the recovery time is very short. Almost all patients go home the same day after hysteroscopic surgery. Unlike some other procedures, there is very little pain after hysteroscopic surgery and problems such as injury to the cervix or the uterus, infection, or heavy bleeding occur in less than one percent of patients. 4 Questions and Answers About Hysteroscopy What types of hysteroscopy are there? Hysteroscopy can be either diagnostic (finding the cause of a disorder) or operative (surgically treating the cause of the disorder). Operative hysteroscopy can also be used for permanent sterilization by placing a small device into the tube at the junction with the uterus. What is diagnostic hysteroscopy? In diagnostic hysteroscopy, a hysteroscope is used to look for growths and other abnormalities in the uterus. It can be done in the doctor’s office in only a few minutes. It may be used instead of— or in addition to—dilation and curettage (D&C), a procedure in which the lining of the uterus is scraped and a tissue sample can be taken and analyzed. Diagnostic hysteroscopy is used to evaluate the cause of infertility, repeated miscarriages, or abnormal bleeding. How is diagnostic hysteroscopy done? To prepare for diagnostic hysteroscopy, the doctor may first use an antiseptic in the vagina and then numb your cervix to prevent discomfort during dilation, which is done to extend the cervix to better see during the procedure. Your vagina and cervix are then washed with an antiseptic solution. A tiny video camera and light are attached to the hysteroscope to allow the doctor to see inside the uterus. The hysteroscope is inserted through the opening of the cervix and into the uterus. Meanwhile, fluid or carbon dioxide gas is pumped into the uterus to keep it inflated and allow the doctor to see more easily. The doctor looks for fibroids, polyps, or other problems that may be causing bleeding. A small plastic tube may also be used to take tissue samples from the lining of the uterus. Normally, the procedure takes several minutes. What is operative hysteroscopy? Operative hysteroscopy is used to treat many of the irregularities or disorders that may be uncovered during diagnostic hysteroscopy. It can be used to remove polyps, fibroids situated within the uterine cavity, or intrauterine devices (IUDs) that have become embedded in the wall of the uterus. Hysteroscopy can also be Questions and Answers About Hysteroscopy 5 used to repair certain structural abnormalities you may have had since birth, such as a uterine septum. It can also be used to perform endometrial ablation, also known as uterine resection (removal of the lining of the uterus), to treat abnormal bleeding. In some cases, endometrial ablation is an alternative to hysterectomy (removal of the uterus), with a shorter recovery time and better patient satisfaction. Hysteroscopy can be used to relieve tubal blockage at the junction with the uterus, to promote fertility, or to close the tube for permanent sterilization. How is operative hysteroscopy done? Operative hysteroscopy can often be performed during the same visit as a diagnostic hysteroscopy, or it can be done at a later time. It is much like diagnostic hysteroscopy except that a slightly wider instrument might be used to allow surgical instruments, such as scissors, biopsy forceps, electrosurgical or laser instruments, and graspers to be inserted into the uterus. Depending on which procedures are performed, it may take anywhere from several minutes to over an hour. Ask your doctor how long the procedure will take. Operative hysteroscopy can be performed under general, regional, or local anesthesia, depending on the doctor’s preference and the type of procedure expected. As in diagnostic hysteroscopy, the doctor will dilate your cervix, insert the hysteroscope into the uterine cavity, and fill the uterus with gas or fluid to get a better view. The instruments are used to remove fibroids, scar tissue, and polyps, and to repair structural abnormalities such as a uterine septum. Operative hysteroscopy can also be used to perform endometrial ablation (removal of the uterine lining to treat heavy bleeding). In this case, the doctor may refer to the procedure as a “resection.” Operative hysteroscopy may also be used to open blocked tubes or insert a small device to close off the tubes for sterilization. Following your surgery, a Foley catheter or IUD may be placed inside the uterus to prevent the uterine walls from sticking together and forming scar tissue. The doctor may prescribe antibiotics and/or hormone medications after uterine surgery to prevent infection and to speed up healing. 6 Questions and Answers About Hysteroscopy What happens after the procedure? If local anesthesia is used, you may be able to go home shortly after the procedure. If regional or general anesthesia is used, you may need to be watched for several hours before going home. After operative hysteroscopy, you may have mild cramping, which usually is gone by the next morning. You may also have some shoulder pain if gas is used to inflate the uterus. You may experience light bleeding for several days following operative hysteroscopy. You should alert your doctor if you develop any of the following symptoms: • Abnormal discharge • Heavy vaginal bleeding • Fever (over 101˚ F) • Inability to urinate • Severe lower abdominal pain • Vomiting • Shortness of breath What are the risks of hysteroscopy? Hysteroscopy is a relatively safe procedure with few complications. Complications only occur in less than one percent of patients. When complications do occur, they are rarely severe or life-threatening. Questions and Answers About Hysteroscopy 7 Summary Diagnosing and correcting disorders of the uterus once required major surgery and many days in the hospital. Hysteroscopy now allows physicians to diagnose and correct many of these disorders without requiring a hospital stay. Recovery time is generally short, taking only a few hours after diagnostic hysteroscopy and two to three days after operative hysteroscopy, with only minimal discomfort. Before you have a hysteroscopy, you and your doctor should discuss any concerns you may have about these procedures, including their risks. Notes 8 Questions and Answers About Hysteroscopy