Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
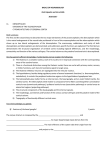
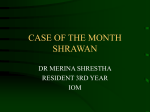
Characterization of Cortical Microvascularization in Adult Moyamoya Disease Marcus Czabanka, MD; Pablo Peña-Tapia, MD; Gerrit A. Schubert, MD; Johannes Woitzik, MD; Peter Vajkoczy, MD; Peter Schmiedek, MD Downloaded from http://stroke.ahajournals.org/ by guest on June 17, 2017 Background and Purpose—Increased cortical microvascularization has been proposed to be a Moyamoya disease (MMD)–specific characteristic. It was the aim of our study to characterize the anatomic pattern and microhemodynamics of cortical microvascularization in MMD. Methods—Intraoperative indocyanine green videoangiography was performed in 16 adult MMD patients, 15 patients with atherosclerotic cerebrovascular disease (ACVD), and 10 control patients. Cortical microvascularization and microvascular hemodynamics were categorized and analyzed according to anatomic and functional indocyanine green angiographic aspects. Anatomic analysis included microvascular density, microvascular diameter, and microvascular surface per analyzed area. Microhemodynamic analysis included microvascular transit time, arterial microvascular transit time, and venous microvascular transit time. Results—Microvascular density and diameter were significantly increased in MMD patients (1.8⫾0.2 mm/mm2 and 0.24⫾0.03 mm, respectively) compared with those in ACVD patients (1.5⫾0.2 mm/mm2 and 0.20⫾0.02 mm, respectively) and controls (1.5⫾0.1 mm/mm2 and 0.19⫾0.03 mm, respectively). This resulted in significantly increased microvascular surface per analyzed area in MMD (67⫾13%) vs ACVD patients (47⫾7%) and controls (45⫾6%). Anatomic changes were paralleled by significantly increased microvascular and arterial microvascular transit times in MMD patients (11.55⫾3.50 and 6.79⫾2.96 seconds, respectively) compared with those in ACVD patients (8.13⫾1.78 and 4.34⫾1.30 seconds, respectively) and controls (8.04⫾2.16 and 4.50⫾1.87 seconds, respectively). Conclusion—Cortical microvascularization in MMD is characterized by significantly increased microvascular density and microvascular diameter, leading to increased microvascular surface. These anatomic alterations are accompanied by prolonged microvascular hemodynamics. These observations might represent an MMD-specific compensation mechanism for impaired cerebral blood flow. (Stroke. 2008;39:1703-1709.) Key Words: Moyamoya disease 䡲 cortical vascularization 䡲 indocyanine green videoangiography 䡲 cerebral blood flow 䡲 compensation mechanism M oyamoya disease (MMD) is a rare and unique cerebrovascular disease. It is characterized by progressive occlusion of the basal arteries of the circle of Willis in association with a network of fine “moyamoya vessels” at the base of the brain.1 Furthermore, there are several additional mechanisms in MMD, like transdural and extracranialintracranial collateral formation, dilation of peripheral cerebral arteries, or the development of leptomeningeal anastomoses, that compensate for the reduced cerebral blood flow (CBF).2 Despite those compensating mechanisms, MMD patients have chronic cerebral ischemia with cerebrovascular hemodynamic insufficiency. Therefore, surgical revascularization represents an effective treatment option for this disease. Cortical vascularization plays an important role in regulating cerebral perfusion and blood flow.3 Many reports suggest increased cortical microvascularization in MMD as a compensating mechanism for chronically impaired CBF.2,4 However, cortical microvascularization has not been thoroughly analyzed in MMD so far, and consequently, there is little knowledge about cortical microvascularization and microhemodynamics in this form of cerebrovascular disease. With the introduction of intraoperative indocyanine green (ICG) videoangiography, visualization and investigation of cortical vascularization have become possible.5,6 With this technique, it was the aim of our study to characterize the anatomic and microhemodynamic aspects of cortical microvascularization Received September 4, 2007; final revision received October 22, 2007; accepted October 30, 2007. From the Department of Neurosurgery (M.C., P.P.-T., G.A.S., P.S.), Klinikum Mannheim, Medical Faculty Mannheim, University of Heidelberg, Heidelberg, and the Department of Neurosurgery (M.C., J.W., P.V.), Charité-Universitätsmedizin Berlin, Berlin, Germany. Correspondence to Marcus Czabanka, MD, Department of Neurosurgery, Charité-Universitätsmedizin Berlin, Campus Virchow Klinikum, Am Augustenburgerplatz 1, 13353 Berlin, Germany. E-mail [email protected] © 2008 American Heart Association, Inc. Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.107.501759 1703 1704 Stroke June 2008 A A2 23 sec. 14 sec. 10 sec. x1 A2 Arterial peak fluorescence activity x3 x2 V1 V2 Parenchym peak fluorescence activity Venous peak fluorescence activity B 100 MVTT AMVTT 80 x1 60 VMVTT x3 x2 Downloaded from http://stroke.ahajournals.org/ by guest on June 17, 2017 40 20 0 0 5 10 15 20 25 Figure 1. A, Photographs of the analysis procedure: example of postoperative analysis of microvascular hemodynamics in an MMD patient. Left image, ICG videoangiography 10 seconds after start of the analysis process, showing peak fluorescence activity in A2 vessels (arterial compartment). x1 encircles the analysis-relevant A2 vessel. Middle image, ICG videoangiography 14 seconds after start of the analysis process, showing peak fluorescence activity in the cortical parenchyma (capillary compartment). x2 indicates the analysisrelevant brain parenchyma; delineation of microvascularization illustrates analysis of MD (length of microvessels per ROI), with 3 ROIs and the corresponding microvessels within those areas. Right image, ICG videoangiography 23 seconds after start of the analysis process, showing peak fluorescence activity in V2 vessels (venous compartment). x3 encircles the analysis-relevant V2 vessel. B, Schematic illustration of intravascular fluorescence evaluation (x1 indicates arterial compartment; x2, capillary compartment; and x3, venous compartment). Arrows demonstrate calculation of MVTT, AMVTT, and VMVTT. Time (sec.) in MMD. As a reference, we analyzed cortical microvascularization and microhemodynamics in patients with atherosclerotic cerebrovascular disease (ACVD) with coexisting hemodynamic compromise and in control patients with physiologic cortical angioarchitecture and microhemodynamics. cerebral surface before intraoperative ICG videoangiography guaranteed dimensional accuracy during postoperative analysis. During application of the fluorescent marker, blood pressure monitoring was recorded and evaluated to exclude hemodynamic alterations that could interfere with cerebral perfusion during ICG injection. Cortical Vascularization Subjects and Methods Patient Population and Surgical Procedures Between March 2006 and February 2007, a total of 41 patients were included in our study. Of these, 16 patients were diagnosed with MMD according to diagnostic criteria.7 MMD patients received combined cerebral revascularization by standard extracranialintracranial bypass surgery in combination with encephalomyosynangiosis. Fifteen patients with ACVD and hemodynamic compromise were included in our study. All ACVD patients received standard extraintracranial arterial bypass surgery. As a control group, 10 patients with physiologic cortical angioarchitecture and microhemodynamics were analyzed. Nine of these patients underwent surgery for an unruptured intracranial aneurysm, and 1 patient underwent surgery via a transtentorial approach for a cerebellar tumor. All surgeries were performed with use of the Pentero OPMI surgical microscope (Carl Zeiss AG, Jena, Germany) with an integrated ICG videoangiography system. Preoperatively, MMD and ACVD patients underwent conventional catheter digital subtraction angiography and morphological imaging by magnetic resonance imaging. Functional regional cerebral blood flow (rCBF) measurements were made at rest and after the administration of acetazolamide (15 mg/kg body weight) by stable xenon computed tomography (Xe-CT; DDP Inc, Houston, Tex). Cerebrovascular reserve capacity (CVRC) was calculated as described elsewhere in detail.8 To obtain CBF values for the region analyzed by ICG videoangiography, regions of interest (ROIs) on the Xe-CT images were located in the vascular territory under investigation (eg, vascular territory of the middle cerebral artery). ICG Videoangiography In all patients, ICG videoangiography was performed according to the surgical indications. Placement of a millimeter-scale grid on the For analysis of cortical vascularization, we categorized arterial and venous macrovascularization as well as cortical microvascularization according to the functional ICG angiographic aspects. The early filling arteries (A1) and their direct branches (A2) and the last draining veins (V1) and their direct branches (V2) were referred to as cortical macrovascularization. All vessels that appeared between A2 and V2 vessels were regarded as cortical microvascularization (Figure 1). Microvascularization was quantified postoperatively by a computer-assisted analysis system (CAPIMAGE, Zeintl Software Engineering, Heidelberg, Germany). For quantification of cortical microvascularization, we analyzed 3 suitable ROIs per cerebral cortex. ROIs were characterized as an area of 25 to 100 mm2 without A1, A2, V1, or V2 vessels within that area. According to a previously described procedure,9 quantification of microvascular density (MD) was performed by measuring the length of all microvessels per analyzed ROI (Figure 1). Furthermore, microvascular diameter (D) was analyzed, and microvascular surface area (MVS) per analyzed ROI was calculated from the following formula: MVS⫽⫻D/2⫻MD. Microhemodynamic Analysis of Cortical Microvascularization Microhemodynamic analysis was performed postoperatively with IC-CALC 1.1 software (Pulsion Medical Systems). For analysis of cortical microhemodynamics, we analyzed fluorescence intensity in 3 distinct compartments in a time-dependent manner: ie, the arterial compartment (A2 vessels), capillary compartment (brain parenchyma), and venous compartment (V2 vessels). Figure 1A demonstrates the different compartments during ICG videoangiography. By comparing the time points of peak fluorescence intensity in the arterial (A2 vessels) and venous (V2 vessels) compartments, we Czabanka et al Cortical Microvascularization in Adult Moyamoya Disease were able to measure the time required for the fluorescent dye to pass the cortical microvascularization. This time was defined as microvascular transit time (MVTT). Furthermore, we analyzed the time difference of peak fluorescence intensity between the arterial (A2 vessels) and capillary compartments. This time was defined as arterial microvascular transit time (AMVTT). According to this procedure, venous microvascular transit time (VMVTT) was defined as the time difference between the capillary and venous (V2 vessels) compartments. Figure 1B demonstrates microhemodynamic definitions and illustrates the analysis procedure. Statistical Analysis For comparisons between 3 groups, 1-way ANOVA and subsequent comparison with Fisher’s least significant difference test were used. Student’s t test was applied for comparisons of CBF values between MMD and ACVD patients. Differences were considered statistically significant for P⬍0.05. All values are given as mean⫾SD. Results Patient Population Downloaded from http://stroke.ahajournals.org/ by guest on June 17, 2017 The mean age of the MMD patient group was 41⫾12 years. In the ACVD patient group, the mean age was 57⫾10 years, and the mean age of control patients was 53⫾9 years. There was a significant difference in mean age between the MMD patients and the ACVD and control patients. No difference was observed between ACVD patients and controls. Detailed descriptions of the patient groups are illustrated in Table. rCBF Assessed by Xe-CT We analyzed rCBF in 13 MMD patients. Measurement of CBF could not be performed in 3 patients due to intolerance of the procedure: nausea and vomiting in 2 cases and asthma bronchiale in 1 patient. Therefore, a total of 13 CBF measurements were included in our study. Mean basal CBF was 52⫾20 mL/100 g per min, and mean stimulated CBF was 55⫾22 mL/100 g per min. CVRC was 7⫾25%. In the ACVD patient group, we included 14 CBF measurements, as 1 patient did not tolerate the Xe-CT due to nausea and vomiting. Mean basal CBF was 49⫾10 mL/100 g per min, and mean stimulated CBF was 53⫾18 mL/100 g per min. CVRC was 6⫾26%. There was no significant difference in rCBF and CVRC values between both patient groups. Table summarizes CBF values of the ACVD and MMD patients. Intraoperative Blood Pressure Monitoring Mean systolic blood pressure during ICG videoangiography in MMD patients was 134⫾16 mm Hg, and mean diastolic blood pressure was 69⫾10 mm Hg (Table). In ACVD patients, mean systolic blood pressure was 129⫾11 mm Hg, whereas mean diastolic blood pressure was 66⫾8 mm Hg (Table). Mean systolic blood pressure in control patients was 129⫾8 mm Hg, and mean diastolic pressure was 69⫾6 mm Hg (Table). There was no statistical difference in systolic and diastolic blood pressures between all groups. Cortical Microvascularization Cortical MD of MMD patients was 1.8⫾0.2 mm/mm2. In ACVD patients, cortical MD was 1.5⫾0.2 mm/mm2, and control patients showed an MD of 1.5⫾0.1 mm/mm2. There was a statistically significant difference between MMD patients and the 2 other groups. We found no difference 1705 between ACVD patients and controls. Furthermore, D in MMD patients was 0.24⫾0.03 mm. In ACVD patients, D was 0.20⫾0.02 mm, and in controls, 0.19⫾0.03 mm. There was a statistically significant difference in D between MMD patients versus ACVD and patients controls. MVS was found to be 67⫾13% in MMD patients compared with 47⫾7% in ACVD and 45⫾6% in control groups. There was a statistically significant difference in MVS between MMD patients and the other 2 groups. We found no significant differences in MD, D, and MVS between ACVD patients and control patients. Figure 2A comprises intraoperative images of cortical microvascularization and the corresponding ICG videoangiogram; Figure 2B is a graphical illustration of our results for MD, D, and MVS. Cortical Microhemodynamics Functional analysis revealed an MVTT for MMD patients of 11⫾3 seconds. MVTT in ACVD patients was 8⫾2 seconds, and in controls, it was 8⫾2 seconds. Statistical analysis revealed a significantly increased MVTT in MMD patients compared with the 2 other patient groups. There was no statistically significant difference between ACVD patients and controls. In terms of AMVTT, functional analysis revealed an AMVTT for MMD patients of 6⫾3 seconds. ACVD patients displayed an AMVTT of 4⫾1 seconds, and in control patients, AMVTT was 4⫾2 seconds. There was a statistically significant difference in AMVTT between MMD patients versus ACVD patients and controls. We found no difference in AMVTT between ACVD patients and controls. VMVTT in MMD patients was 5⫾2 seconds. In ACVD patients VMVTT was 4⫾2 seconds, and in control patients it was 3⫾2 seconds. We found no significant differences in VMVTT between all patient groups. Figure 3 demonstrates the graphical results of microhemodynamic analysis. Discussion In our study, we observed significant increases in MD, D, MVS, and MVTT in adult MMD patients compared with ACVD patients and controls. Adult MMD patients are additionally characterized by significantly prolonged AMVTT compared with that in ACVD patients and controls. In terms of VMVTT, we found no differences between our patient groups. Therefore, we have demonstrated an MMD-specific structural increase in cortical microvessels and significantly prolonged cortical microhemodynamics in MMD. These observations might represent an MMD-specific compensation mechanism for the reduced CBF and oxygen supply. The brain uses a number of compensating mechanisms to adapt to chronic ischemia, like collateral blood flow from the other hemisphere via the circle of Willis, a reduction in cerebral metabolism, maximal dilation of basal cerebral arteries, and the development of leptomeningeal and extraintracranial anastomoses.10 However, these mechanisms vary on an individual basis10 and often do not completely restore CBF. Patients with chronically decreased CVRC are at particular risk for ischemic stroke.11,12 In our study, MMD as well as ACVD patients displayed typical features of hemodynamic cerebral ischemia11 with impaired CVRC.13 1706 Stroke Table. June 2008 Summary of Patient Groups Included in our Study Case Age, y, Sex CBF, Basal/Stimulated, mL/100 g per min CVRC, % Blood Pressure, mm Hg Diagnosis Surgical Procedure 1 45, M 44.68/36.30 ⫺7.38 150/70 MMD Bypass/EMS 2 34, F 32.50/40.87 8.37 140/80 MMD Bypass/EMS 3 20, F NP (COPD) 130/70 MMD Bypass/EMS 4 38, F 57.19/59.77 2.58 130/70 MMD Bypass/EMS 5 44, F 58.00/37.70 ⫺20.30 150/80 MMD Bypass/EMS 6 50, F NP (N&V) NP (N&V) 140/70 MMD Bypass/EMS 7 26, F 76.70/95.70 19.00 140/75 MMD Bypass/EMS 8 42, F 74.10/84.97 10.69 120/60 MMD Bypass/EMS Downloaded from http://stroke.ahajournals.org/ by guest on June 17, 2017 9 51, F 36.30/38.08 10 30, F NP (N&V) 11 50, F 12 43, F 13 14 NP (COPD) 1.78 150/70 MMD Bypass/EMS NP (N&V) 105/50 MMD Bypass/EMS 33.04/47.60 14.56 125/65 MMD Bypass/EMS 91.74/84.79 ⫺6.95 110/60 MMD Bypass/EMS 48, M 28.62/23.98 ⫺4.64 140/80 MMD Bypass/EMS 22, F 43.66/65.32 21.66 120/60 MMD Bypass/EMS 15 47, M 63.90/56.24 ⫺7.66 160/90 MMD Bypass/EMS 16 64, M 43.56/50.54 6.98 140/60 MMD Bypass/EMS 17 59, M NP (N&V) NP (N&V) 120/60 L ICA occlusion Bypass 18 50, M 54.59/54.5 ⫺0.09 140/70 L ICA occlusion Bypass 19 63, F 37.06/27.28 ⫺9.78 130/60 R ICA stenosis Bypass 20 50, F 58.42/70.72 12.3 130/70 R ICA occlusion Bypass 21 72, M 69.60/67.76 ⫺1.84 140/70 R ICA occlusion Bypass 22 65, M 42.55/50.70 8.15 120/60 L ICA occlusion Bypass 23 67, M 43.40/30.59 ⫺12.81 140/70 L ICA stenosis Bypass 24 65, M 41.44/31.00 ⫺10.44 140/70 R ICA occlusion Bypass 25 53, M 53.10/60.96 7.86 110/60 R ICA T-stenosis Bypass 26 43, F 35.36/33.35 ⫺2.01 110/50 L ICA occlusion Bypass 27 38, F 55.90/69.56 13.66 120/80 R ICA stenosis Bypass 28 60, F 42.35/61.06 18.71 130/60 R ICA stenosis Bypass 29 48, M 40.30/47.36 7.06 140/70 R ICA occlusion Bypass 30 51, F 58.22/45.44 ⫺12.78 140/80 R ICA occlusion Bypass 31 39, F NP NP 140/80 R MCA aneurysm Clipping 32 60, F NP NP 125/60 R MCA aneurysm Clipping 34 62, F NP NP 120/55 Cerebellar tumor Resection 35 55, M NP NP 120/70 R MCA aneurysm Clipping 36 47, F NP NP 144/80 R MCA aneurysm Clipping 37 57, F NP NP 120/70 R MCA aneurysm Clipping 38 49, M NP NP 130/70 L MCA aneurysm Clipping 39 68, M NP NP 130/70 L MCA aneurysm Clipping 40 40, F NP NP 125/60 R MCA aneurysm Clipping 41 50, M NP NP 135/70 L MCA aneurysm Clipping M indicates male; F, female; NP, not performed; COPD, chronic obstructive pulmonary disease; N&V, nausea and vomiting; Bypass, standard extraintracranial arterial bypass; EMS, encephalomyosynangiosis; R, right; L, left; ICA, internal carotid artery; and MCA, middle cerebral artery. A negative CVRC value indicates steal phenomenon during acetazolamide stimulation. Extracranial-intracranial bypass surgery has been shown to restore CVRC and thus, represents an efficient treatment option for patients with such reductions.11 Especially in MMD, surgical revascularization represents a very effective treatment option for restoring CBF and for preventing cerebral ischemia. In MMD, cortical microvascularization is of special interest, as Takeuchi et al4 described surgically exposed cortical surfaces that appeared reddish intraoperatively due to multiple leptomeningeal anastomoses and dilated pial arteries. Our surgical experience in the treatment of MMD confirms this observation.2 Intraoperative ICG videoangiography allows excellent visualization of cortical vascularization and has already been applied successfully to study cortical perfusion after decom- Czabanka et al ACVD Control A Cortical Microvascularization in Adult Moyamoya Disease MMD B 15 10 5 Control ACVD MMD Microvascular surface (%) * Microvascular diameter (mm) 20 100 0,4 # 0 *# 0,3 0,2 0,1 *# 80 60 18 16 14 20 0 0,0 Control ACVD MMD AMVTT VMVTT MVTT Control ACVD MMD *# 12 *# 10 8 6 4 2 0 Control Figure 2. A, Photographs of intraoperative cortical microvascularization and corresponding ICG videoangiograms. B, Graphs of MD, D, and microvascular surface per ROI. Left graph demonstrates MD in controls (n⫽10), ACVD patients (n⫽15), and MMD patients (n⫽16). *#Significant differences vs controls and ACVD patients, respectively. Middle graph demonstrates D in controls (n⫽10), ACVD patients (n⫽15), and MMD patients (n⫽16). *#Significant differences vs controls and ACVD patients, respectively. Right graph demonstrates MVS per analyzed ROI in controls (n⫽10), ACVD patients (n⫽15), and MMD patients (n⫽16). *#Significant differences vs controls and ACVD patients, respectively. 40 pressive craniectomy for malignant stroke.5 Using this technique, we observed a 20% increase in MD paralleled by significantly increased D and MVS in MMD patients, whereas ACVD patients with a comparable ischemic deficit displayed values comparable to those of controls. MMD has significant neoangiogenic potential, which might explain our observation of increased MD, D, and MVS.14,15 However, until now, no molecular mechanism has been identified, and it remains unclear whether MMD-associated neovascularization is a result of a distinct disease-related molecular pathway or an adaptive mechanism to cope with impaired cerebral hemodynamics. Cerebral hemodynamics in MMD differs substantially from hemodynamics in ACVD. First of all, MMD is defined by bilateral steno-occlusive lesions of the basal cerebral arteries.16 ACVD does not refer to bilateral steno-occlusive lesions but it Microvascular transit time (sec.) Downloaded from http://stroke.ahajournals.org/ by guest on June 17, 2017 Microvascular density (cm/cm²) 25 1707 ACVD MMD Figure 3. Graph illustrating results for MVTT, AMVTT, and VMVTT in controls (n⫽10), ACVD patients (n⫽15), and MMD patients (n⫽16). *#Significant differences vs controls and ACVD patients, respectively. includes unilateral steno-occlusive lesions. In MMD, the posterior circulation may also be affected; therefore, compensation for low CBF by cross-flow through the circle of Willis might be more limited in certain MMD patients. In atherosclerosis, leptomeningeal arteries and ophthalmic collaterals play a major role in compensating for low CBF.17 In MMD, collateralization via the ophthalmic artery is not possible, as the definition of MMD includes supraophthalmic steno-occlusive lesions of basal cerebral arteries.7 However, leptomeningeal anastomoses are also observed in MMD patients and are regarded as significant contributors to the collateral blood supply.18 We evaluated the vascular territory of the middle cerebral artery in all cases except for one. Leptomeningeal anastomoses are defined as arteries between 2 major cerebral arteries that supply 2 different cortical territories.18 Therefore, cortical microvascularization according to our definition does not refer to leptomeningeal anastomoses. However, we expect similar effects, as observed in our study, on the level of leptomeningeal anastomoses. In contrast to ACVD patients, compensation for low CBF in MMD is achieved by a unique MMD-specific neoangiogenic process. Neovascularization in the form of moyamoya vessels at the base of the brain has been demonstrated to lead to significantly increased CBF and cerebrovascular CO2 reactivity in the basal ganglia of MMD compared with ACVD patients.19 Because cortical vascularization plays an important role in regulating CBF,3 increased MD, D, and MVS might exert significant effects on cerebral microhemodynamics and thus, contribute to the compensation for hemodynamic impairment. Increased MD, D, and MVS might consequently compensate for the impaired CBF either by increasing collateral blood flow or by reducing microvascular 1708 Stroke June 2008 Downloaded from http://stroke.ahajournals.org/ by guest on June 17, 2017 resistance. As mentioned earlier, MMD is characterized by multiple stenotic lesions of the circle of Willis20,21; therefore, increasing collateral blood flow might represent a rather inefficient mechanism.7 In this scenario, decreasing microvascular resistance might be the more efficient mechanism for compensating for impaired CBF. To investigate cerebral microhemodynamics, we measured MVTT, AMVTT, and VMVTT. According to our definitions, MVTT indirectly represents microvascular blood flow velocity, as the time from maximum fluorescence intensity in A2 to V2 vessels represents the time required for peak blood flow to pass the cortical microvascularization. This parameter was significantly increased in MMD patients compared with ACVD and control groups. Our results are supported by results from Taki et al,22 who demonstrated prolonged cerebral circulation time in MMD patients. Cortical arterial microvascularization plays an important role in regulating cerebral perfusion, as more than half of the total cerebrovascular resistance is located in the extraparenchymal vessel segments.3 An increase in arteriolar resistance vessels leads to an increase in microvascular cross-sectional area and thus, decreased peripheral microvascular resistance. Therefore, conductance of the microvascular segment in the organ vasculature is increased, resulting in decreased blood flow velocity. By measuring AMVTT and VMVTT, we were able to localize the vascular compartment responsible for the reduction in MVTT. According to our results, MVTT was lost in the arterial compartment in MMD patients. The observation of increased AMVTT in combination with increased MD, D, and MVS suggests decreased peripheral microvascular resistance as the mechanism of choice. In support of this hypothesis, Okada et al23,24 were able to demonstrate diminished vascular resistance between cortical arteries of the middle cerebral artery territory and the corresponding veins in MMD patients. Moreover, there is experimental evidence that an increase in cortical arterial microvascularization represents a suitable mechanism for the compensation of reduced CBF. Schneider et al25 demonstrated an increase in the number of extraparenchymal and intraparenchymal arterioles in response to application of granulocyte-macrophage colony stimulating factor in a rat model of cerebrovascular occlusive disease. The authors showed that increasing the number of pial arterial resistance vessels led to decreased total peripheral resistance and a concomitant restoration of CVRC.25 Therefore, we propose a potentially new compensation mechanism in MMD: ie, increased MD, D, and MVS at the level of cerebral microvascularization, potentially resulting in decreased peripheral vascular resistance. Further studies will be needed to investigate and characterize the clinical significance of this potential new compensation mechanism in MMD. Summary Intraoperative ICG videoangiography was used to investigate and characterize cortical microvascularization and microhemodynamics in MMD compared with ACVD patients and in subjects with normal cerebral microvascularization. On an anatomic level, we demonstrated increases in MD, D, and MVS in MMD patients compared with the other 2 groups. In terms of microhemodynamic characteristics, we demonstrated increases in MVTT and AMVTT in MMD patients compared with ACVD patients and controls. Our observations might represent an MMD-specific compensation mechanism for reduced CBF, either by increasing collateral blood flow or by reducing peripheral vascular resistance. Acknowledgment We thank Peter Horn, MD, for revisions to the manuscript and substantial advice. Disclosures None. References 1. Handa J, Handa H. Progressive cerebral arterial occlusive disease: analysis of 27 cases. Neuroradiology. 1972;3:119 –133. 2. Horn P, Vajkoczy P, Schmiedek P. Spontaneous occlusion of the circle of Willis (moyamoya disease): diagnosis and therapy. Nervenarzt. 2001;72: 406 – 415 (in German). 3. Baumbach GL, Heistad DD. Regional, segmental, and temporal heterogeneity of cerebral vascular autoregulation. Ann Biomed Eng. 1985;13: 303–310. 4. Takeuchi S, Ishii R, Tsuchida T, Tanaka R, Kobayashi K, Ito J. Cerebral hemodynamics in patients with moyamoya disease: a study of the epicerebral microcirculation by fluorescein angiography. Surg Neurol. 1984; 21:333–340. 5. Woitzik J, Pena-Tapia PG, Schneider UC, Vajkoczy P, Thome C. Cortical perfusion measurement by indocyanine-green videoangiography in patients undergoing hemicraniectomy for malignant stroke. Stroke. 2006; 37:1549 –1551. 6. Raabe A, Beck J, Gerlach R, Zimmermann M, Seifert V. Near-infrared indocyaninegreen videoangiography: a new method for intraoperative assessment of vascular flow. Neurosurgery. 2003;52:132–139; discussion 139. 7. Fukui M. Guidelines for the diagnosis and treatment of spontaneous occlusion of the circle of Willis (‘Moyamoya’ disease): research committee on spontaneous occlusion of the circle of Willis (Moyamoya disease) of the Ministry of Health and Welfare, Japan. Clin Neurol Neurosurg. 1997;99(suppl 2):S238 –S240. 8. Horn P, Vajkoczy P, Thome C, Muench E, Schilling L, Schmiedek P. Xenon-induced flow activation in patients with cerebral insult who undergo xenon-enhanced CT blood flow studies. AJNR Am J Neuroradiol. 2001;22:1543–1549. 9. Vajkoczy P, Schilling L, Ullrich A, Schmiedek P, Menger MD. Characterization of angiogenesis and microcirculation of high-grade glioma: an intravital multifluorescence microscopic approach in the athymic nude mouse. J Cereb Blood Flow Metab. 1998;18:510 –520. 10. Sipos C. Modalities of compensation of cerebral circulation through the circle of Willis in stenoses and occlusions of extracranial arteries. Neurol Res. 1992;14:149 –151. 11. Schmiedek P, Piepgras A, Leinsinger G, Kirsch CM, Einhupl K. Improvement of cerebrovascular reserve capacity by EC-IC arterial bypass surgery in patients with ICA occlusion and hemodynamic cerebral ischemia. J Neurosurg. 1994;81:236 –244. 12. Gratzl O, Rem J, Mueller HR, Radue EW, Mueller-Brand J. Cerebral blood flow and common carotid flow in neurologically asymptomatic carotid endarterectomy patients. Neurol Res. 1990;12:26 –28. 13. Ueno M, Nishizawa S, Toyoda H, Shimono T, Miyamoto S, Hashimoto N, Konishi J. Assessment of cerebral hemodynamics before and after revascularization in patients with occlusive cerebrovascular disease by means of quantitative IMP-SPECT with double-injection protocol. Ann Nucl Med. 2001;15:209 –215. 14. Lim M, Cheshier S, Steinberg GK. New vessel formation in the central nervous system during tumor growth, vascular malformations, and Moyamoya. Curr Neurovasc Res. 2006;3:237–245. 15. Kassner A, Zhu XP, Li KL, Jackson A. Neoangiogenesis in association with Moyamoya syndrome shown by estimation of relative recirculation based on dynamic contrast-enhanced MR images. AJNR Am J Neuroradiol. 2003;24:810 – 818. 16. Natori Y, Ikezaki K, Matsushima T, Fukui M. ‘Angiographic Moyamoya’: its definition, classification, and therapy. Clin Neurol Neurosurg. 1997;99(suppl 2):S168 –S172. Czabanka et al Cortical Microvascularization in Adult Moyamoya Disease 17. Yamauchi H, Kudoh T, Sugimoto K, Takahashi M, Kishibe Y, Okazawa H. Pattern of collaterals, type of infarcts, and haemodynamic impairment in carotid artery occlusion. J Neurol Neurosurg Psychiatry. 2004;75: 1697–1701. 18. Brozici M, van der Zwan A, Hillen B. Anatomy and functionality of leptomeningeal anastomoses: a review. Stroke. 2003;34:2750 –2762. 19. Obara K, Fukuuchi Y, Kobari M, Watanabe S, Dembo T. Cerebral hemodynamics in patients with Moyamoya disease and in patients with atherosclerotic occlusion of the major cerebral arterial trunks. Clin Neurol Neurosurg. 1997;99(suppl 2):S86 –S89. 20. Miyamoto S, Kikuchi H, Karasawa J, Nagata I, Ihara I, Yamagata S. Study of the posterior circulation in Moyamoya disease, part 2: visual disturbances and surgical treatment. J Neurosurg. 1986;65:454 – 460. 21. Miyamoto S, Kikuchi H, Karasawa J, Nagata I, Ikota T, Takeuchi S. Study of the posterior circulation in Moyamoya disease: clinical and neuroradiological evaluation. J Neurosurg. 1984;61:1032–1037. 1709 22. Taki W, Yonekawa Y, Kobayashi A, Ishikawa M, Kikuchi H, Nishizawa S, Yonekura Y, Tanada S, Fukuyama H. Cerebral circulation and metabolism in adults’ Moyamoya disease: PET study. Acta Neurochir (Wien). 1989;100:150 –154. 23. Okada Y, Shima T, Nishida M, Yamane K, Yamada T, Yamanaka C. Effectiveness of superficial temporal artery–middle cerebral artery anastomosis in adult moyamoya disease: cerebral hemodynamics and clinical course in ischemic and hemorrhagic varieties. Stroke. 1998;29:625– 630. 24. Okada Y, Shima T, Matsumura S, Nishida M, Yamada T, Okita S. Pathophysiological studies in Moyamoya disease by rCBF and cortical artery pressure measurements in comparison to those in ICA or MCA occlusion. No To Shinkei. 1988;40:899 –903 (in Japanese). 25. Schneider UC, Schilling L, Schroeck H, Nebe CT, Vajkoczy P, Woitzik J. Granulocyte-macrophage colony-stimulating factor-induced vessel growth restores cerebral blood supply after bilateral carotid artery occlusion. Stroke. 2007;38:1320 –1328. Downloaded from http://stroke.ahajournals.org/ by guest on June 17, 2017 Characterization of Cortical Microvascularization in Adult Moyamoya Disease Marcus Czabanka, Pablo Peña-Tapia, Gerrit A. Schubert, Johannes Woitzik, Peter Vajkoczy and Peter Schmiedek Downloaded from http://stroke.ahajournals.org/ by guest on June 17, 2017 Stroke. 2008;39:1703-1709; originally published online April 10, 2008; doi: 10.1161/STROKEAHA.107.501759 Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2008 American Heart Association, Inc. All rights reserved. Print ISSN: 0039-2499. Online ISSN: 1524-4628 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://stroke.ahajournals.org/content/39/6/1703 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Stroke is online at: http://stroke.ahajournals.org//subscriptions/