Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Psychoneuroimmunology wikipedia , lookup
Neonatal infection wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Germ theory of disease wikipedia , lookup
Globalization and disease wikipedia , lookup
Hepatitis B wikipedia , lookup
Onchocerciasis wikipedia , lookup
Infection control wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
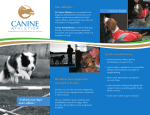
Review Canine leishmaniosis – new concepts and insights on an expanding zoonosis: part one Gad Baneth1*, Alexander F. Koutinas2*, Laia Solano-Gallego3*, Patrick Bourdeau4* and Lluis Ferrer5* 1 School of Veterinary Medicine, Hebrew University, P.O. Box 12, Rehovot 76100, Israel Companion Animal Clinic, Faculty of Veterinary Medicine, Aristotle University of Thessaloniki, 11 St Voutyra Street, 54627 Thessaloniki, Greece 3 Royal Veterinary College, Department of Pathology and Infectious Diseases, Hawkshead Lane, North Mymms, Hatfield, Herts AL9 7TA, UK 4 Ecole Nationale Veterinaire de Nantes, Route de Gachet, BP 40706, Nantes Cedex 03, France 5 Departament de Medicinia i Cirurgia Animals, Universitat Autonoma de Barcelona, 08193-Bellaterra, Spain 2 Recent research has provided new insights on the epidemiology, pathology and immunology of canine leishmaniosis (CanL) and its genetic basis. The prevalence of infection in endemic areas is considerably higher than that of apparent clinical illness. In addition, infection spreads rapidly among dogs in the presence of optimal conditions for transmission. Infection involves a variety of granulomatous and harmful immunemediated responses, and susceptibility to the disease is influenced by a complex genetic basis. These concepts will be instrumental for devising control programs. This review, the first in a series of two articles on CanL, presents an updated view on progress in elucidating the epidemiology and pathogenesis of this challenging disease, and the second part focuses on advances in diagnosis, treatment and prevention. An expanding complex zoonosis Canine leishmaniosis (CanL) is caused by Leishmania infantum, or its New World synonym Leishmania chagasi, and is a major potentially fatal zoonotic infection in regions of Europe, Africa, Asia and America. The domestic dog is the main reservoir of human infection, and phlebotomine sand flies are the biological vectors of this protozoal disease. It has been estimated that at least 2.5 million dogs are infected in southwestern Europe alone [1], and the disease is spreading north into the foothills of the Alps and the Pyrenees [2]. The number of infected dogs in South America also is estimated in millions, and there are high infection rates in some areas of Venezuela and Brazil, where a high prevalence of canine infection is associated with high risk of human disease [3]. The term ‘CanL’ used in this review describes infection with L. infantum, which affects both the viscera and skin of dogs, but does not encompass canine tegumentary leishmaniosis caused by Leishmania spp. in the New World or Leishmania tropica, a rare cause of disease in dogs in the Old World [4]. Corresponding author: Baneth, G. ([email protected]). The authors are members of the LeishVet European Clinical Standardization Group. * 324 CanL is a complex disease that has a high prevalence of infection, involving as much as 63%–80% of the population [5–7], and is accompanied by a lower rate of apparent clinical disease. Dogs that do show disease manifest different clinical signs and variable degrees of severity. Substantial research published recently on the pathogenesis of CanL and immune responses during infection has contributed considerably to our understanding of this complex zoonosis and its epidemiology [5,8,9]. Current studies have revealed new facts about the prevalence and spread of infection and established novel concepts on its evolution and dynamics [2,3,5,6,8]. These new insights impact on efforts to prevent and control the disease and its spread into human populations. Epidemiology of CanL in endemic regions – major concepts Two major concepts have arisen from epidemiological research with molecular diagnostic techniques for CanL. The first concept is that infection in endemic areas is widespread, but not all infected dogs develop the disease. An early study employing cellular immunity and serological assays demonstrated that a spectrum of immune responses to Leishmania infection is present among asymptomatic dogs in an endemic area [10]. An experimental model of infection showed that dogs mounted variable immune responses, and although some developed the disease, other infected dogs remained asymptomatic over a 5year observation period [11]. Studies using PCR in endemic areas have confirmed that the prevalence of infection in dogs is much higher than the proportion that actually develops symptomatic disease [5,7,12]. A study of 100 dogs from a municipal pound in the island of Mallorca, Spain, indicated that 13% had apparent clinical disease, 26% were seropositive and 63% were found to be positive for Leishmania DNA when tested by PCR [5]. Of 73 clinically healthy hunting dogs in Greece, 12.3% tested positive by using serology, whereas 63% tested positive by using PCR [6]. Longitudinal studies in endemic areas have shown that the natural history of the infected dogs can evolve in 1471-4922/$ – see front matter ß 2008 Elsevier Ltd. All rights reserved. doi:10.1016/j.pt.2008.04.001 Available online 29 May 2008 Review different ways [8,13]. Two major patterns of progression have been documented. In some dogs severe clinical signs of the disease appear shortly after infection. It is thought that animals with severe disease are unable to develop an effective cellular immune response, although they have a strong but ineffective humoral response [14,15]. A second group of dogs remains infected for a long period of time (years or lifelong), but they are able to avoid the appearance of lesions and clinical disease [11,14]. However, a change in the health status of these dogs or, for instance, the administration of an immunosuppressive drug or a severe immunosuppressive disease can lead to the activation of a latent infection and the development of clinical signs. The second concept is that when favorable conditions for disease transmission (such as high vector sand-fly and canine-host densities) are present, the infection spreads quickly and extensively among the dog population [8,16,17]. The evolution of a cohort of naı̈ve dogs exposed to three consecutive transmission seasons in Naples, Italy, indicated that at the end of the study, 97.3% of the dogs were positive by bone-marrow-nested PCR and 75.7% were seropositive. This extremely high prevalence of infection was attributed to a high density of Phlebotomus perniciosus vectors in the disease focus and the lack of control measures to protect the dogs [8]. These two concepts (Box 1) have clarified that clinical CanL is only the tip of the iceberg in endemic areas, and the majority of the population is exposed and becomes infected without showing clinical evidence of disease or serum antiLeishmania antibodies (Figure 1). Canine leishmaniosis in nonendemic regions Canine visceral leishmaniosis is often diagnosed in nonendemic countries, and the need for detection and treatment of this disease also is imperative in northern Europe and other areas where no natural transmission occurs [18–20]. This mostly is due to the increased travel of dogs in and out of endemic areas. A study from Holland found that about 58 000 dogs are taken yearly to southern Europe with their owners on vacation, and the risk of acquiring leishmaniosis is 0.027%–0.23% [18]. Importation and relocation of dogs from endemic countries is responsible for the growing numbers of dogs with this disease in Germany [19]. The Pet Travel Scheme has eased the movement of dogs from EU countries, the USA and rabies-free islands to the UK. The change in quarantine restrictions and the increased numbers of traveling and imported companion animals has raised serious concerns about the introduction of CanL into the UK [20]. The risk for autochthonous transmission from traveled dogs in the absence of sand-fly vectors is probably small; however, infection has been described in Box 1. New concepts on the epidemiology of canine leishmaniosis Infection in the canine population in endemic areas is widespread, and the rate of infected dogs is much higher than the fraction that shows clinical illness. Infection spreads quickly and extensively among the dog population when environmental conditions for transmission are optimal. Trends in Parasitology Vol.24 No.7 Figure 1. A schematic presentation of the distribution of leishmaniosis among the canine population in an endemic focus, as seen in a cross-sectional study. The peak of the pyramid (orange) consists of a relatively small subset of dogs showing clinical signs of the disease. Seropostive dogs with no signs of disease represent a second subset (beige). Most of the dogs in the clinical disease and the asymptomatic seropositive subsets would be PCR+. A third subset includes asymptomatic PCR+ but seronegative infected dogs (purple), and a fourth subset includes dogs that are seronegative and do not harbor parasites (blue). A minority of dogs might be seropositive and PCR- (not shown in this model). A study from the Island of Mallorca, Spain [5], showed that 13% of the dogs had clinical disease, 26% were seropositive, 63% were PCR positive and 67% had evidence of infection either by serology or by PCR. dogs with no travel history living together with imported infected dogs, pups born to infected dams or animals receiving blood transfusions from infected canine donors [21–23]. Canine visceral leishmaniosis in the USA was reported rarely before 2000, when infection was implicated as the cause of mortality in a foxhound kennel in New York State [24]. A serosurvey revealed that canine infection, predominantly involving foxhounds, is present in 18 states and two Canadian provinces [25]. No autochthonous human cases were reported, and sand-fly transmission in the USA has not been demonstrated. This unique situation is currently being investigated with major concern regarding the possibility of spread to humans. Update on canine pathology during the disease Canine visceral leishmaniosis is a multisystemic disease with variable clinical signs [4,26–29]. The majority of dogs are presented with poor body condition, generalized muscular atrophy, lymphadenomegaly and excessive skin scaling (Table 1 and Figure 2). The typical histopathological finding in their tissues is a granulomatous inflammatory reaction associated with the presence of Leishmania amastigotes within macrophages. The dermal changes in CanL include exfoliative, ulcerative, nodular and pustular dermatitis [27,30,31]. Extracellular matrix assessment in the skin of symptomatic dogs demonstrated a decrease in collagen type I and an increase in collagen type III fibers proportional to the severity of the skin lesion and tissue destruction [32]. Dermal lesions in CanL are not necessarily provoked by an inflammatory response to the physical presence of parasites in the skin 325 Review Trends in Parasitology Vol.24 No.7 Table 1. Clinical findings in dogs with symptomatic canine leishmaniosis Clinical examination finding Skin disease Enlargement of lymph nodes Eye disease Pallor of mucous membranes Enlarged spleen Cachexia Fever Nose bleeding (epistaxis) Abnormal nails (onychogryposis) Percentage of symptomatic dogs 81%–89% 62%–90% 16%–81% 58% 10%–53% 10%–48% 4%–36% 6%–10% 20%–31% Refs [4,27] [4,26,27] [4,27,41,42] [27] [4,26,27] [4,26,27] [26,27] [26,27] [4,26,27] because normal-looking skin also harbors large numbers of parasites in symptomatic dogs. Furthermore, a similar parasite load was found in skin with macroscopic lesions and normal-looking skin from symptomatic dogs [30,31]. The marked enlargement of lymph nodes in CanL is caused by the increased number and size of lymphoid follicles and the marked hypertrophy and hyperplasia of medullary macrophages in the cords and sinuses [33]. The parasitic load in enlarged lymph nodes frequently is not correlated with the type and severity of lesions in other organs [33,34]. The enlargement of the spleen in CanL is associated with increased monocyte and macrophage cellularity and changes in the microvasculature structure with abundant pulp venules and veins and increased reticular fibers [35]. The kidneys are affected in virtually all dogs with CanL, and renal disease might be the only apparent abnormality in infected dogs. A study of seropositive dogs from Brazil identified glomerulonephritis in all 55 dogs, of which 13 were asymptomatic. Interstitial nephritis was present in 78% of the dogs, and glomerular deposition of parasite antigen was seen in 91% [36]. Renal disease can progress from asymptomatic proteinuria to nephrotic syndrome or chronic renal failure with glomerulonephritis, tubulointerstitial nephritis and amyloidosis [27]. Glomerulonephritis frequently is associated with the renal deposition of immune complexes [37]. Despite the high prevalence of kidney pathology, azotemia with the elevation of serum creatinine and urea typical of kidney failure are evident only when the majority of nephrons are dysfunctional, which happens rather late during disease progression. Joint and bone lesions frequently are present in infected dogs [38]. A study on skeletal lesions in CanL found that of 58 dogs with CanL, 45% had gait abnormalities. Both erosive and nonerosive polyarthritis were observed with Leishmania amastigotes detected by microscopy in the synovial fluid [38]. Affected bones typically have periosteal and intramedulary proliferative lesions with frequent cortical and medullary osteolysis [37–39]. Progressive muscle atrophy is associated with chronic polymyositis characterized by the presence of mononuclear infiltrates with Leishmania amastigotes, neutrophilic vasculitis and IgG immune complexes in muscle tissues in conjunction with serum anti-myofiber antibodies [40]. Ocular lesions are present in 16% to 80.5% of dogs with symptomatic CanL [26,27,41,42]. These consist of anterior uveitis, conjunctivitis, dry keratoconjunctivitis, blepharitis or a combination of these. Eye lesions are the sole presenting complaint in up to 16% of symptomatic cases. In dry keratoconjunctivitis, inflammatory infiltrates located around the lacrimal ducts cause secretory retention and a decrease in tear production [42]. Nose bleeding (epistaxis), hematuria and hemorrhagic diarrhoea in CanL are associated with tissue ulceration and alterations in primary and secondary hemostasis. Hemostatic disorders described in CanL include platelet aggregation abnormalities leading to platelet dysfunction, low platelet number, decreased coagulation factor activities and fibrinolysis [43]. Profuse epistaxis can appear as Figure 2. Clinical manifestations of symptomatic canine leishmaniosis: (a) purulent keratoconjunctivitis with periocular dermatitis, (b) facial skin lesions with multifocal exfoliative dermatitis, (c) epistaxis, (d) onychogryposis and (e) skin ulceration on the ear. 326 Review the only presenting sign of disease and can be a cause of death because of uncontrollable blood loss. The underlying mechanism involves pyogranulomatous or lymphoplasmacytic rhinitis, (with or without ulceration), thrombocytopathy and hyperglobulinemia [44]. Anemia is present in the majority of symptomatic dogs because of chronic renal disease or decreased erythropoiesis caused by chronic disease and can be aggravated by blood loss or immunemediated destruction of red blood cells [26,27]. Genetics of susceptibility and resistance to canine visceral leishmaniosis Evidence that the host’s genetics could play a major role in susceptibility or resistance to CanL has come from different sources. Investigations on the genetics of human visceral leishmaniasis have indicated that several genes are involved in disease susceptibility. Studies on kala-azar (visceral leishmaniosis) caused by Leishmania donovani in endemic areas in Sudan showed that although more than 90% of the villagers showed immunological evidence of infection, only 30% developed kala-azar. Candidate gene testing revealed linkage to polymorphism in the natural resistance-associated macrophage protein 1 (NRAMP1) gene later named the Slc11a1 gene [45]. The Slc11a1 gene encodes a proton divalent cation antiporter with a role in regulating macrophage function – including upregulation of chemokine and cytokine genes, such as tumor necrosis factor (TNF) and interleukin-1b (IL-1b) – and induction of nitric oxide synthase [46]. These investigations demonstrated that in humans there is a complex genetic basis for susceptibility to developing visceral leishmaniasis, which involves several mechanisms and additional genes such as the interleukin-4 (IL-4) and interferon-g receptor [47]. Epidemiological studies in canine populations suggested a role for genetics in the resistance to developing the disease (Box 2). The Ibizian hound, a local breed from the Balearic islands, was reported to develop a primarily cellular immune response, detected by the leishmanin skin test, and very rarely develop clinical disease [48]. So far, two genes have been implicated in susceptibility to CanL. In a cohort of Brazilian mongrel dogs, a study on the genetic variation in major histocompatabillity complex class II (MHC II), termed ‘the dog leukocyte antigen (DLA) system’ in the dog, has detected a significant association between the presence of the DLA–DRB1*01502 allele and susceptibility to CanL [49]. In another study haplotypes of the canine Slc11a1 gene were identified as associated with susceptibility to CanL in Spain [50]. Moreover, singlenucleotide polymorphism mutations in the promoter Box 2. Evidence that resistance or susceptibility to canine leishmaniosis is genetic The dog breed Ibizian hound typically develops a strong cellular immune response to leishmaniosis and rarely shows clinical disease in Mallorca [48]. Susceptibility to leishmaniosis is associated with a major histocompatabillity complex class II (MHC II) genotype [49]. Certain Slc11a1 (formerly NRAMP1) genotypes are associated with susceptibility to leishmaniosis [50]. Trends in Parasitology Vol.24 No.7 region of the Slc11a1 gene were associated with susceptibility to CanL, as also described in humans [46], and one haplotype (TAG-8-141) was associated with boxers’ predisposition to CanL [51]. These recent findings associating genetics with susceptibility to CanL are probably only pieces of a more complex multigenic puzzle that determines the individual dog’s natural resistance to infection. Nevertheless, susceptibility to developing the disease also is influenced by non-genetic factors such as nutritional status, concomitant infections and parasitism, parasite virulence and previous exposure to CanL. Cellular and humoral immune responses A spectrum of innate and acquired immune responses to L. infantum infection is mounted by the canine host [10,52]. The two opposite extreme poles of this spectrum are protective immunity that is T-cell mediated and susceptibility to overt disease associated with a marked nonprotective humoral immune response and a depressed cell-mediated immunity (CMI) [14,15]. Based on in vitro and in vivo studies, it is widely accepted that macrophages play a central role in the control of Leishmania infection. Cytokines such as interferon-g (IFN-g), IL-2 and tumor necrosis factor-a (TNF-a) secreted by activated T cells induce macrophage anti-leishmanial activity. Nitric oxide (NO) produced by macrophages has been found to be the principal effector molecule mediating intracellular killing of Leishmania amastigotes by apoptotic cell death controlled by proteasome inhibitors [53]. Cellular immune responses It is now widely accepted that protective immunity against Leishmania parasites is mediated by CD4+ T helper1 (Th1) cellular responses [54]. In contrast to the findings in experimental murine cutaneous leishmaniasis, visceral disease in humans, dogs and experimental rodents does not show a clear Th1/Th2 dichotomy pattern [54]. Leishmania infantum appears to induce mixed Th1 and Th2 responses in which the control of parasite replication, disease progression or cure are determined by the balance between these two dichotomous directions (Figure 3). Understanding the profile of cytokines expressed in CanL is complex because of the limited number of studies reported, the broad spectrum of clinical disease stages investigated, the different tissues analyzed and the differences between experimental and natural infection. In naturally infected dogs expression levels of IFN-g in the bone marrow or spleen were similar in symptomatic and asymptomatic dogs [9,55,56], and a predominant induction of both IFN-g (Th1 cytokine) and IL-4 was evident in stimulated Leishmania antigen-peripheral blood mononuclear cells from asymptomatic dogs [57]. Spleen cells from infected dogs showed a predominant expression of IL-10 that was positively correlated with parasitic load and clinical status severity [56]. IL-10 is considered a regulator of the Th1 activity that maintains balance between Th1 and Th2 responses and inhibits the microbicidal activity of infected macrophages [15,58]. Longitudinal experimental CanL infection studies mostly have indicated a mixed Th1 and Th2 pattern 327 Review Trends in Parasitology Vol.24 No.7 Figure 3. A view of the complex interaction between the Th1 and Th2 responses in visceral leishmaniosis focused on current understanding of these responses in CanL. Mixed Th1 and Th2 responses occur in infected dogs, and it is assumed that the balance between these responses tilts in the Th2 direction in dogs that succumb to clinical illness, whereas a stronger protective Th1 activity directs to resistance. The cytokines IFN-g, IL-2 and TNF-a induce macrophage activation and NO killing of parasites in the Th1 response. By contrast, IL-10, TGF-b and IL-4 are involved in the parasite dissemination associated with increased B-cell (B) and plasma-cell (P) activity and hyperglobulinemia related to the Th2 response. Th1 responses are downregulated by IL-10 produced by T-regulatory (Treg) cells. IL-10 also is produced by cells of the Th1 lineage and is proposed to be beneficial in limiting secondary immunopathology triggered by infection, but it also prevents sterile immunity and allows persistence of low-level infection. [54]. Cytokine expression in blood showed an initial asymptomatic phase with an absence of or low expression during a period of ‘silent establishment of parasite’ followed by a short-term production of Th1-type cytokines before the appearance of clinical signs [59]. In another study cytokine and chemokine expression in the spleen revealed an initial elevation in IL4 one month postinfection followed by an increase in the Th1-associated IFN-g and chemokines Tbet, IP-10 and RANTES [54]. The cellular basis and mechanisms for the development of T-cell unresponsiveness in CanL are not understood fully. The majority of infected dogs are likely to develop positive specific CMI expressed as proliferation of lymphocytes stimulated in vitro by Leishmania antigen or in vivo by a positive skin test early in infection. However, as the disease progresses in susceptible dogs, these responses diminish. Blood parasite load and Leishmania-specific CMI were shown to be inversely correlated during a longitudinal follow-up of experimentally infected dogs [60]. It has been postulated that CMI unresponsiveness in progressive disease is due to the decrease in peripheral CD4+ T-cell numbers or the decreasing expression of co-stimulatory molecules such as B7 [12,15,61,62]. Humoral immune response Canine leishmaniosis frequently is associated with a marked humoral response, which is not protective and signifies failure to control the infection. The levels of Leishmania-specific immunoglobulins detected in symptomatic dogs are greater than those detected in infected but asymptomatic dogs, and a marked association was found between these levels, the clinical status and tissue parasite density [63]. 328 The levels of the canine IgG subclasses IgG1 and IgG2 have been studied extensively in an attempt to establish a correlation between the subclass level, the type of Th response and the clinical outcome of infection. Studies evaluating IgG1 and IgG2 using polyclonal antibodies frequently have reached conflicting outcomes, possibly because of a lack of specificity of commercial reagents [58]. Moreover, investigations employing monoclonal antibodies to canine IgG1 and IgG2 have shown a steady increase in the production of both subclasses during natural and experimental CanL without indicating a practical use for these levels [17,54]. Transmission of canine leishmaniosis The natural cycle of Leishmania infection involves a phlebotomine sand-fly vector in which promastigotes replicate after transformation from intracellular amastigotes taken during the bloodmeal. There are numerous sand-fly species, and only a minority of these are competent vectors of CanL [64]. Dogs with symptomatic as well as asymptomatic infections are infectious to sand flies. However, infectiousness appears to be higher in dogs with clinical disease. In a study from Brazil, 28% of seropositive symptomatic dogs were infectious to Lutzomyia longipalpis sand flies, whereas only 5.4% of the asymptomatic dogs were infectious [65]. Infectiousness of dogs is related to immunosuppression as manifested by levels of circulating Th cells. An inverse relationship was found between the CD4+ T-cell count in naturally infected dogs and their infectiousness to sand flies, as found for HIV+ people coinfected with L. infantum [62,66]. Although sand flies are the only biologically adapted vectors of leishmaniosis, a possible role in transmission for other hematophagous ectoparasites, such as ticks and Review fleas, has been proposed. Transmission of leishmaniosis to laboratory hamsters was achieved under experimental conditions when Rhipicephalus sanguineus ticks and Ctenocephalides felis fleas from naturally infected dogs were macerated and orally inoculated into hamsters [67,68]. However, the significance of transmission to dogs by these arthropods has not been verified in natural conditions. Congenital transmission of visceral leishmaniasis from infected mother to offspring is reported in humans and has been studied experimentally in mice. Canine vertical infection was demonstrated experimentally in puppies born to infected male and female beagles, and transmission was assumed to be transplacental [22]; however, investigations in naturally infected dogs have reported conflicting outcomes [69,70]. In addition to the option of transmission by blood transfusion [23], direct dog-to-dog transmission by contact has been suggested to take place in the USA in an effort to explain the spread of CanL among kennel foxhounds in the absence of proven sand-fly vectors and human infection [25]. Modalities of infection other than sand-fly transmission should be further studied; however, at present it is not known whether they play an important role in the epidemiology of CanL. Summary Recent research has revealed the extensive distribution and expansion of CanL in large areas of the world. The slow and progressive nature of this severe zoonosis and the high infectiousness of dogs to sand flies are of major concern. It is clear that control efforts and preventative measures should encompass total dog populations in endemic regions to be effective. The second part of this review will address updates on diagnosis, treatment, prevention and public health concerns. It will integrate concepts described in this part with further insights leading to improved possibilities for future control programs. References 1 Moreno, J. and Alvar, J. (2002) Canine leishmaniasis: epidemiological risk and the experimental model. Trends Parasitol. 18, 399–405 2 Ferroglio, E. et al. (2005) Canine leishmaniasis. Italy. Emerg. Infect. Dis. 11, 1618–1620 3 Werneck, G.L. et al. (2006) Multilevel modeling of the incidence of visceral leishmaniasis in Teresina, Brazil. Epidemiol. Infect. 135, 195– 201 4 Baneth, G. et al. (2006) Leishmaniases.. In Infectious Diseases of the Dog and Cat (3rd edn) (Greene, C.E., ed.), pp. 685–698, Saunders 5 Solano-Gallego, L. et al. (2001) Prevalence of Leishmania infantum infection in dogs living in an area of canine leishmaniasis endemicity using PCR on several tissues and serology. J. Clin. Microbiol. 39, 560–563 6 Leontides, L.S. et al. (2002) A cross-sectional study of Leishmania spp. Infection in clinically healthy dogs with polymerase chain reaction and serology in Greece. Vet. Parasitol. 109, 19–27 7 Berrahal, F. et al. (1996) Canine leishmaniasis: identification of asymptomatic carriers by polymerase chain reaction and immunoblotting. Am. J. Trop. Med. Hyg. 55, 273–277 8 Oliva, G. et al. (2006) Incidence and time course of Leishmania infantum infections examined by parasitological, serologic, and nested-PCR techniques in a cohort of naı̈ve dogs exposed to three consecutive transmission seasons. J. Clin. Microbiol. 44, 1318–1322 9 Quinnell, R.J. et al. (2001) Tissue cytokine responses in canine visceral leishmaniasis. J. Infect. Dis. 183, 1421–1424 10 Cabral, M. et al. (1998) The immunology of leishmaniosis: strong evidence for a developing disease spectrum from asymptomatic dogs. Vet. Parasitol. 76, 173–180 Trends in Parasitology Vol.24 No.7 11 Killick-Kendrick, R. et al. (1994) A laboratory model of canine leishmaniasis: the inoculation of dogs with Leishmania infantum promstigotes from midguts of experimentally infected phlebotomine sandflies. Parasite 1, 311–318 12 Alvar, J. et al. (2004) Canine leishmaniasis. Adv. Parasitol. 57, 1–88 13 Quinnell, R.J. et al. (2001) Detection of Leishmania infantum by PCR, serology and cellular response in a cohort of Brazilian dogs. Parasitology 122, 253–261 14 Pinelli, E. et al. (1994) Cellular and humoral immune reponses in dogs experimentally and naturally infected with Leishmania infantum. Infect. Immun. 62, 229–235 15 Barbieri, C.L. (2006) Immunology of canine leishmaniasis. Parasite Immunol. 28, 329–337 16 Quinnell, R.J. et al. (1997) The epidemiology of canine leishmaniasis: transmission rates estimated from a cohort study in Amazonian Brazil. Parasitology 115, 143–156 17 Quinnell, R.J. et al. (2003) IgG subclass responses in a longitudinal study of canine visceral leishmaniasis. Vet. Immunol. Immunopathol. 91, 161–168 18 Teske, E. et al. (2002) Risk of infection with Leishmania spp. in the canine population in the Netherlands. Acta Vet. Scand. 43, 195–201 19 Gothe, R. et al. (1997) Leishmaniasis in dogs in Germany: epidemiological case analysis and alternatives to conventional therapy. Tierarztl. Prax. 25, 68–73 20 Shaw, S.E. et al. (2003) Review of exotic infectious diseases in small animals entering the United Kingdom from abroad diagnosed by PCR. Vet. Rec. 152, 176–177 21 Diaz-Espineira, M.M. and Slappendel, R.J. (1997) A case of autochthonous canine leishmaniasis in the Netherlands. Vet. Q. 19, 69–71 22 Rosypal, A.C. et al. (2005) Transplacental transmission of a North American isolate of Leishmania infantum in an experimentally infected beagle. J. Parasitol. 91, 970–972 23 De Freitas, E. et al. (2006) Transmission of Leishmania infantum via blood transfusion in dogs: potential for infection and importance of clinical factors. Vet. Parasitol. 137, 159–167 24 Gaskin, A.A. et al. (2002) Visceral leishmaniasis in a New York foxhound kennel. J. Vet. Intern. Med. 16, 34–44 25 Duprey, Z.H. et al. (2006) Canine visceral leishmaniasis, United States and Canada, 2000-2003. Emerg. Infect. Dis. 12, 440–446 26 Ciaramella, P. et al. (1997) A retrospective clinical study of canine leishmaniosis in 150 dogs naturally infected by Leishmania infantum. Vet. Rec. 141, 539–543 27 Koutinas, A.F. et al. (1999) Clinical considerations on canine visceral leishmaniasis in Greece: a retrospective study of 158 cases (1989 – 1996). J. Am. Anim. Hosp. Assoc. 35, 376–383 28 Adamama-Moraitou, K.K. et al. (2007) Asymptomatic colitis in naturally infected dogs with Leishmania infantum: a prospective study. Am. J. Trop. Med. Hyg. 76, 53–57 29 Rallis, T. et al. (2005) Chronic hepatitis associated with canine leishmaniasis (Leishmania infantum): a clinicopathological study of 26 cases. J. Comp. Pathol. 132, 145–152 30 Solano-Gallego, L. et al. (2004) Histological and immunohistochemical study of clinically normal skin of Leishmania infantum-infected dogs. J. Comp. Pathol. 130, 7–12 31 Papadogiannakis, E.I. et al. (2005) Cellular immunophenotyping of exfoliative dermatitis in canine leishmaniosis (Leishmania infantum). Vet. Immunol. Immunopathol. 104, 227–237 32 Giunchetti, R.C. et al. (2006) Relationship between canine visceral leishmaniosis and the Leishmania (Leishmania) chagasi burden in dermal inflammatory foci. J. Comp. Pathol. 135, 100–107 33 Lima, W.G. et al. (2004) Canine visceral leishmaniasis: a histopathological study of lymph nodes. Acta Trop. 92, 43–53 34 Mylonakis, M.E. et al. (2005) Cytologic patterns of lymphadenopathy in dogs infected with Leishmania infantum. Vet. Clin. Pathol. 34, 243–247 35 Alexandre-Pires, G. et al. (2006) Leishmaniosis – a report about the microvascular and cellular architecture of the infected spleen in Canis familiaris. Microsc. Res. Tech. 69, 227–235 36 Costa, F.A. et al. (2003) Histopathological patterns of nephropathy in naturally acquired canine visceral leishmaniasis. Vet. Pathol. 40, 677–684 37 Nieto, C.G. et al. (1992) Pathological changes in kidneys of dogs with natural Leishmania infection. Vet. Parasitol. 45, 33–47 329 Review 38 Agut, A. et al. (2003) Clinical and radiographic study of bone and joint lesions in 26 dogs with leishmaniasis. Vet. Rec. 153, 648–652 39 Blavier, A. et al. (2001) Atypical forms of canine leishmaniasis. Vet. J. 162, 108–120 40 Vamvakidis, C.D. et al. (2000) Masticatory and skeletal muscle myositis in canine leishmaniasis (Leishmania infantum). Vet. Rec. 146, 698–703 41 Peña, M.T. et al. (2000) Ocular and periocular manifestations of leishmaniasis in dogs: 105 cases (1993 – 1998). Vet. Ophthalmol. 3, 35–41 42 Naranjo, C. et al. (2005) Characterization of lacrimal gland lesions and possible pathogenic mechanisms of keratoconjunctivitis sicca in dogs with leishmaniosis. Vet. Parasitol. 133, 37–47 43 Ciaramella, P. et al. (2005) Altered platelet aggregation and coagulation disorders related to clinical findings in 30 dogs naturally infected by Leishmania infantum. Vet. J. 169, 465–467 44 Juttner, C. et al. (2001) Evaluation of the potential causes of epistaxis in dogs with natural visceral leishmaniasis. Vet. Rec. 149, 176–179 45 Bucheton, B. et al. (2003) Genetic control of visceral leishmaniasis in a Sudanese population: candidate gene testing indicates a linkage to the NRAMP1 region. Genes Immun. 4, 104–109 46 Blackwell, J.M. et al. (2001) Slc11a1 (formerly NRAMP1) gene and disease resistance. Cell. Microbiol. 3, 773–784 47 Mohamed, H.S. et al. (2003) Genetic susceptibility to visceral leishmaniasis in the Sudan: linkage and association with IL4 and IFNGR1. Genes Immun. 4, 351–355 48 Solano-Gallego, L. et al. (2000) The Ibizian hound presents a predominantly cellular immune response against natural Leishmania infection. Vet. Parasitol. 90, 37–45 49 Quinnell, R.J. et al. (2003) Susceptibility to visceral leishmaniasis in the domestic dog is associated with MHC class II polymorphism. Immunogenetics 55, 23–28 50 Altet, L. et al. (2002) Mapping and sequencing of the canine NRAMP1 gene and identification of mutations in leishmaniasis-susceptible dogs. Infect. Immun. 70, 2763–2771 51 Sánchez-Robert, E. et al. (2005) Polymorphism of Slc11a1 (Nramp1) gene and canine leishmaniasis in a case-control study. J. Hered. 96, 755–758 52 Reis, A.B. et al. (2006) Phenotypic features of circulating leucocytes as immunological markers for clinical status and bone marrow parasite density in dogs naturally infected by Leishmania chagasi. Clin. Exp. Immunol. 146, 303–311 53 Holzmuller, P. et al. (2006) Phenotypical characteristics, biochemical pathways, molecular targets and putative role of nitric oxide-mediated programmed cell death in Leishmania. Parasitology 132 (Suppl.), S19– S32 54 Strauss-Ayali, D. et al. (2007) Splenic immune responses during canine visceral leishmaniasis. Vet. Res. 38, 547–564 330 Trends in Parasitology Vol.24 No.7 55 Correa, A.P. et al. (2007) Evaluation of transformation growth factor b1, interleukin-10, and interferon-g in male symptomatic and asymptomatic dogs naturally infected by Leishmania (Leishmania) chagasi. Vet. Parasitol. 143, 267–274 56 Lage, R.S. et al. (2007) Analysis of the cytokine profile in spleen cells from dogs naturally infected by Leishmania chagasi. Vet. Immunol. Immunopathol. 115, 135–145 57 Chamizo, C. et al. (2005) Semi-quantitative analysis of cytokine expression in asymptomatic canine leishmaniasis. Vet. Immunol. Immunopathol. 103, 67–75 58 Day, M.J. (2007) Immunoglobulin G subclass distribution in canine leishmaniosis: a review and analysis of pitfalls in interpretation. Vet. Parasitol. 147, 2–8 59 Santos-Gomes, G.M. et al. (2002) Cytokine expression during the outcome of canine experimental infection by Leishmania infantum. Vet. Immunol. Immunopathol. 88, 21–30 60 Rodriguez-Cortes, A. et al. (2007) A long term experimental study of canine visceral leishmaniasis. Int. J. Parasitol. 37, 683–693 61 Pinelli, E. et al. (1999) Compensation for decreased expression of B7 molecules on Leishmania infantum-infected canine macrophages results in restoration of parasite-specific T-cell proliferation and gamma interferon production. Infect. Immun. 67, 237–243 62 Guarga, J.L. et al. (2000) Canine leishmaniasis transmission: higher infectivity amongs naturally infected dogs to sand flies is associated with lower proportions of T helper cells. Res. Vet. Sci. 69, 249–253 63 Reis, A.B. et al. (2006) Isotype patterns of immunoglobulins: hallmarks for clinical status and tissue parasite density in Brazilian dogs naturally infected by Leishmania (Leishmania) chagasi. Vet. Immunol. Immunopathol. 112, 102–116 64 Killick-Kendrick, R. (1999) The biology and control of phlebotomine sand flies. Clin. Dermatol. 17, 279–289 65 Michalsky, E.M. et al. (2007) Infectivity of seropositive dogs, showing different clinical forms of leishmaniasis, to Lutzomyia longipalpis phlebotomine sand flies. Vet. Parasitol. 147, 67–76 66 Molina, R. et al. (1999) Infection of sand flies by humans coinfected with Leishmania infantum and human immunodeficiency virus. Am. J. Trop. Med. Hyg. 60, 51–53 67 Coutinho, M.T.Z. et al. (2005) Participation of Rhipicephalus sanguineus (Acari: Ixodidae) in the epidemiology of canine visceral leishmaniasis. Vet. Parasitol. 128, 149–155 68 Coutinho, M.T.Z. and Linardi, P.M. (2007) Can fleas from dogs infected with canine visceral leishmaniasis transfer the infection to other mammals? Vet. Parasitol. 147, 320–325 69 Andrade, H.M. et al. (2002) Leishmania (Leishmania) chagasi is not vertically transmitted in dogs. Vet. Parasitol. 103, 71–81 70 Diniz, S.A. et al. (2005) Genital lesions associated with visceral leishmaniasis and shedding of Leishmania sp. in the semen of naturally infected dogs. Vet. Pathol. 42, 650–658